Building social currency with foreskin cuts: a coping mechanism of Papua New Guinea health workers...
10
Building social currency with foreskin cuts: a coping mechanism of Papua New Guinea health workers and the implications for new programmes Anna Tynan, 1 * Andrew Vallely, 2,3 Angela Kelly, 2,4 Martha Kupul, 2 Richard Naketrumb, 2 Herick Aeno, 2 Peter Siba, 2 John M Kaldor 3 and Peter S Hill 1 1 Australian Centre for International & Tropical Health, School of Population Health, The University of Queensland, Herston Road, Herston, Queensland 4006, Australia, 2 Sexual & Reproductive Health Unit, Papua New Guinea Institute of Medical Research, PO Box 60, Goroka Eastern Highlands Province 441, Papua New Guinea, 3 Public Health Interventions Research Group, The Kirby Institute, University of New South Wales, 45 Beach Street Coogee, New South Wales 2034, Australia and 4 International HIV Research Group, School of Public Health and Community Medicine, The University of New South Wales, Sydney, Australia *Corresponding author. Australian Centre for International & Tropical Health, School of Population Health, The University of Queensland, Herston Road, Herston, Queensland, 4006, Australia. E-mail: [email protected] Accepted 28 August 2013 Background Recent research as part of a multi-disciplinary investigation on the acceptability and impact of male circumcision for HIV prevention in Papua New Guinea (PNG) has shown that health workers (HWs) undertake unauthorized forms of penile cutting practices in public health facilities or in community settings, at times within a traditional context. Participation in these activities shares common features with coping mechanisms, strategies used by HWs to alleviate the burden of unsatisfactory living and working conditions. Coping mechanisms, however, are typically described as motivated by economic advantage, but in PNG evidence exists that the behaviours of HWs are also influenced by opportunities for social capital. Methods Twenty-five in-depth interviews (IDIs) were completed with a variety of HWs from 2009 until 2011 and were triangulated with findings from 45 focus group discussions and 82 IDIs completed with community members as part of a wider qualitative study. Thematic analysis examined HW participation in unauthorized penile cutting services. Results The emergence of unauthorized practices as a coping mechanism in PNG is compelled by mutual obligations and social capital arising from community recognition and satisfaction of moral, professional and cultural obligations. Using the example of unauthorized penile cutting practices amongst HWs in PNG, the research shows that although economic gains are not expli- citly derived, evidence exists that they meet other community and socio cultural responsibilities forming a social currency within local traditional economies. Conclusions Coping mechanisms create an opportunity to extend the boundaries of a health system at the discretion of the HW. Fragile health systems create opportunities for coping mechanisms to become institutionalized, pre-empting appropriate policy development or regulation in the introduction of new programmes. In order to ensure the success of new programmes, the existence of such practices and their potential implications must be addressed within programme design, and in implementation and regulation. Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine ß The Author 2013; all rights reserved. Health Policy and Planning 2013;1–10 doi:10.1093/heapol/czt072 1 Health Policy and Planning Advance Access published October 8, 2013 at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from at UQ Library on October 17, 2013 http://heapol.oxfordjournals.org/ Downloaded from
Transcript of Building social currency with foreskin cuts: a coping mechanism of Papua New Guinea health workers...

Building social currency with foreskin cutsa coping mechanism of Papua New Guineahealth workers and the implications fornew programmesAnna Tynan1 Andrew Vallely23 Angela Kelly24 Martha Kupul2 Richard Naketrumb2
Herick Aeno2 Peter Siba2 John M Kaldor3 and Peter S Hill1
1Australian Centre for International amp Tropical Health School of Population Health The University of Queensland Herston Road HerstonQueensland 4006 Australia 2Sexual amp Reproductive Health Unit Papua New Guinea Institute of Medical Research PO Box 60 GorokaEastern Highlands Province 441 Papua New Guinea 3Public Health Interventions Research Group The Kirby Institute University of NewSouth Wales 45 Beach Street Coogee New South Wales 2034 Australia and 4International HIV Research Group School of Public Healthand Community Medicine The University of New South Wales Sydney Australia
Corresponding author Australian Centre for International amp Tropical Health School of Population Health The University of QueenslandHerston Road Herston Queensland 4006 Australia E-mail annatynanuqconnecteduau
Accepted 28 August 2013
Background Recent research as part of a multi-disciplinary investigation on the acceptability
and impact of male circumcision for HIV prevention in Papua New Guinea
(PNG) has shown that health workers (HWs) undertake unauthorized forms of
penile cutting practices in public health facilities or in community settings at
times within a traditional context Participation in these activities shares
common features with coping mechanisms strategies used by HWs to alleviate
the burden of unsatisfactory living and working conditions Coping mechanisms
however are typically described as motivated by economic advantage but in
PNG evidence exists that the behaviours of HWs are also influenced by
opportunities for social capital
Methods Twenty-five in-depth interviews (IDIs) were completed with a variety of HWs
from 2009 until 2011 and were triangulated with findings from 45 focus group
discussions and 82 IDIs completed with community members as part of a wider
qualitative study Thematic analysis examined HW participation in unauthorized
penile cutting services
Results The emergence of unauthorized practices as a coping mechanism in PNG is
compelled by mutual obligations and social capital arising from community
recognition and satisfaction of moral professional and cultural obligations
Using the example of unauthorized penile cutting practices amongst HWs
in PNG the research shows that although economic gains are not expli-
citly derived evidence exists that they meet other community and socio
cultural responsibilities forming a social currency within local traditional
economies
Conclusions Coping mechanisms create an opportunity to extend the boundaries of a health
system at the discretion of the HW Fragile health systems create opportunities
for coping mechanisms to become institutionalized pre-empting appropriate
policy development or regulation in the introduction of new programmes In
order to ensure the success of new programmes the existence of such practices
and their potential implications must be addressed within programme design
and in implementation and regulation
Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine
The Author 2013 all rights reserved
Health Policy and Planning 20131ndash10
doi101093heapolczt072
1
Health Policy and Planning Advance Access published October 8 2013 at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
at U
Q L
ibrary on October 17 2013
httpheapoloxfordjournalsorgD
ownloaded from
Keywords Coping mechanisms unauthorized practices penile foreskin cutting social
capital Papua New Guinea health system
KEY MESSAGES
Coping mechanisms have been typically described as motivated by economic advantages however in Papua New Guinea
evidence exists that the behaviours of public servants are influenced by capital derived from relationships or satisfaction
of religious cultural or moral obligations
Fragile health systems create opportunities for unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new programmes are introduced
The success of health programmes underpinned by informal systems will not be achieved merely through bureaucratic
regulation but with strategies that encompass and recognize differences within organizational cultures and communities
IntroductionCoping mechanisms are strategies used by health workers
(HWs) to alleviate the burden of unsatisfactory living and
working conditions such as poor supervision inadequate or
intermittent remuneration or working in hostile environments
in low- and middle-income countries (McPake et al 2000
Schwalbach et al 2000 Macq et al 2001 van Lerberghe et al
2002 Ferrinho et al 2004a) Along with health system failures
coping mechanisms are shaped by social political and institu-
tional environments in which HWs operate and are as import-
ant in shaping how health services function and are perceived
as are planned health reforms and management (Roenen et al
1997 Schwalbach et al 2000 Macq et al 2001 van Lerberghe
et al 2002) Coping mechanisms include unauthorized practices
or activities that fall outside standard treating practices that can
impact on service delivery and may include illegal and non-
illegal activities This article will examine Papua New Guinean
(PNG) HWs engagement in unauthorized penile cutting
activities
Coping mechanisms and their relationship withhealth systems
Coping mechanisms arise due to extreme discrepancies between
social economic and professional expectations of HWs and real-
life situations (Table 1) (Schwalbach et al 2000 van Lerberghe
et al 2002 Garcıa-Prado and Gonzalez 2007) There are a
number of different types of coping mechanisms which are
described in the literature These include HWs receiving
informal payments or under-the-counter payments for other-
wise free services (Delcheva et al 1997 Giedion et al 2001
Falkingham 2004 Lindelow and Serneels 2006 Tediosi 2008
Liu and Sun 2012) misappropriating drugs or other supplies
(Israr et al 2000 Ferrinho et al 2004a Lindelow and Serneels
2006) moonlighting in other roles or dual practice (Ferrinho
et al 2004a Jan et al 2005 Gonzalez and Macho-Stadler 2013)
preferential treatment including accelerated access to health
services for friends family or those who are able to afford
bribes or under-the-counter payments (Roenen et al 1997) and
other unexplained absenteeism (Chaudhury et al 2005 Manzi
et al 2012) There has also been a move to acknowledge other
potential coping strategies for HWs such as receiving in-kind or
in-gratitude payments like access to accommodation or food for
services they perform (Roenen et al 1997 Chereches et al
2013) using time or resourcesmdashsuch as health service ve-
hiclesmdashfrom government projects for personal use (McPake
et al 1999 Macq et al 2001 Ferrinho et al 2004b) and
exploitation of allowances and per diems designed to enable
supervision or attendance at courses (McCoy et al 2008 Smith
2003 Vian et al 2011)
Engagement in coping mechanisms has consequences for the
equity and efficiency of health systems and quality of health
care (Garcıa-Prado and Gonzalez 2007 Jumpa et al 2007
Kiwanuka et al 2011) Health system impacts include compe-
tition for time (due to HWs being less available at public
facilities thereby compromising service delivery) conflict of
interest (for example when HWs lower the quality of services
they provide in the public sector in order to drive patients to the
private sector) and brain drain (or inequitable distribution of
HWs between public and private rural and urban primary and
tertiary and poor and rich settings) (Macq et al 2001 van
Lerberghe et al 2002 Ferrinho et al 2004b Kiwanuka et al
2011 Ashmore 2013) Misuse by HWs of their privileged access
to resources such as pharmaceuticals contributes to financial
losses in the health-care system as well as the growing sense of
mistrust and disrespect for HWs and their institutions
(Ferrinho et al 2004a) Informal payments or under-the-counter
payments provide a financial barrier to those who canrsquot afford
to pay and as a result again jeopardize the necessary trust
between user and provider and public expectations of health
service delivery (van Lerberghe et al 2002 Dabalen and Wane
2008) Inappropriate or unnecessary attendance at training
sessions primarily to obtain the per diem allowances creates
inefficiencies in health systems including reduced HW avail-
ability (van Lerberghe et al 2002 Conteh and Kingori 2010
Vian et al 2011)
Although coping mechanisms may be considered a part of
corrupt practices of government employees or labelled as the
result of poor motivation or inefficient practice there is
evidence that coping mechanisms are not necessarily due to
predatory behaviour but a strategy to deal with difficult
situations that can have positive impacts as well
2 HEALTH POLICY AND PLANNING
Ta
ble
1
Typ
eso
fco
pin
gst
rate
gie
sam
on
gH
Ws
curr
ency
exch
an
ged
an
dim
pact
on
hea
lth
syst
em
Are
ao
rp
roce
sso
fh
ea
lth
syst
em
fail
ure
Co
pin
gst
rate
gy
Typ
es
of
curr
en
cye
xch
an
ge
dP
oss
ible
resu
lt
Hu
man
reso
urc
ing
In
ad
equ
ate
hu
man
reso
urc
ing
In
ad
equ
ate
train
ing
an
dsu
per
visi
on
of
HW
s
Lack
of
com
pu
lso
ryed
uca
tio
n
H
Wass
um
eso
ther
role
san
dre
spo
nsi
-
bil
itie
so
uts
ide
train
ing
R
elia
nce
on
info
rmal
net
wo
rks
for
gu
id-
an
ceo
nap
pro
pri
ate
pra
ctic
e
Reg
ula
ratt
end
an
ceat
wo
rksh
op
san
dtr
ain
ing
(in
clu
din
go
vers
eas)
S
oci
al
reco
gn
itio
nan
dp
rest
ige
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
P
rofe
ssio
nal
sati
sfact
ion
an
dse
lf-
fulf
ilm
ent
thro
ugh
ach
ievi
ng
oth
ersk
ills
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
In
crea
sed
com
pli
cati
on
s
Red
uce
dco
mm
un
ity
tru
stin
hea
lth
wo
rker
san
dth
eir
inst
itu
tio
ns
H
Wst
ress
an
dd
issa
tisf
act
ion
wit
hh
ealt
h
syst
em
Hea
lth
fin
an
cin
g
L
imit
edfu
nd
ing
for
serv
ice
D
iffi
cult
ies
ob
tain
ing
fun
din
g
Lo
ww
ages
H
Ws
rece
ivin
gin
form
al
paym
ents
for
oth
erw
ise
free
serv
ice
R
ecei
vin
ggif
tslsquoi
nk
ind
rsquo
Mo
on
ligh
tin
gin
oth
erro
les
incl
ud
ing
pri
vate
hea
lth
sect
or
or
agri
cult
ure
usi
ng
tim
eo
rre
sou
rces
fro
mgo
vern
men
t
pro
ject
s
Pil
feri
ng
dru
gs
an
dm
edic
ines
P
erd
iem
sfo
rtr
ave
lan
dtr
ain
ing
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
Pro
fess
ion
al
sati
sfact
ion
an
dse
lf-f
ulf
il-
men
tb
yp
art
icip
ati
ng
ino
ther
role
s
So
cial
use
skil
lsas
HW
togain
com
mu
-n
ity
pre
stig
ean
dre
cogn
itio
n
C
om
pet
itio
nfo
rti
me
O
utf
low
of
reso
urc
esfr
om
the
pu
bli
c
sect
or
C
on
flic
tso
fin
tere
st
Hig
hp
rice
of
hea
lth
care
D
iscr
imin
ati
on
of
pati
ents
acc
ord
ing
to
cap
aci
tyto
pay
In
ad
equ
ate
serv
ice
del
iver
y
Med
icin
esan
dte
chn
olo
gy
In
suff
icie
nt
med
icin
esan
dte
chn
ical
equ
ipm
ent
for
the
man
agem
ent
of
pate
nts
G
ener
al
lack
of
basi
csu
pp
lies
M
isap
pro
pri
ati
ng
dru
gs
or
oth
ersu
pp
lies
for
fam
ily
or
oth
eracq
uain
tan
ces
O
verc
harg
ing
pati
ents
for
dru
gs
an
d
oth
ersu
pp
lies
H
Ws
usi
ng
reso
urc
esto
pro
vid
eu
nre
c-o
gn
ized
ad
dit
ion
al
serv
ices
of
the
org
an
izati
on
S
oci
al
usi
ng
acc
ess
tore
sou
rces
as
aH
W
tosa
tisf
yco
mm
un
ity
or
cult
ura
lo
bli
gati
on
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
Deg
rad
ati
on
of
qu
ali
tyca
re
Co
un
terf
eit
dru
gs
F
inan
cial
loss
toth
eh
ealt
hsy
stem
Hea
lth
info
rmati
on
syst
ems
P
oo
racc
ou
nta
bil
ity
an
dre
cord
kee
pin
g
Lim
ited
acc
ess
top
rofe
ssio
nal
dev
elo
p-
men
tan
dre
sou
rces
U
nex
pla
ined
ab
sen
teei
sm
Eco
no
mic
su
pp
lem
ent
low
sala
ries
wit
h
cash
an
dtr
ad
itio
nal
eco
no
mie
s
So
cial
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s
fost
erin
gre
lati
on
ship
s
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
W
ork
do
ne
inp
riva
tese
cto
rn
ot
cap
ture
d
Hea
lth
serv
ices
L
imit
edse
rvic
eava
ilab
ilit
y
Po
or
wo
rkin
gco
nd
itio
ns
incl
ud
ing
po
or
faci
liti
esan
dre
sou
rces
W
ork
ing
inch
all
engin
gan
dd
an
ger
ou
s
envi
ron
men
ts
N
epo
tism
for
bet
ter
hea
lth
serv
ice
F
aci
lita
tio
no
fq
ueu
eju
mp
ing
for
rela
-
tive
san
dfr
ien
ds
S
oci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs
Un
exp
lain
edab
sen
teei
sm
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
g
rela
tio
nsh
ips
E
con
om
ic
acc
ess
totr
ad
itio
nal
eco
no
my
or
lsquoin
kin
drsquo
paym
ents
D
iscr
imin
ato
ryp
ract
ice
L
ow
uti
liza
tio
no
fse
rvic
e
Sta
teH
Ws
bec
om
ele
ssava
ilab
leto
wo
rk
inth
ep
ub
lic
sect
or
bu
td
on
ot
resi
gn
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
HW
fati
gu
e
Lea
der
ship
an
dgo
vern
an
ce
P
oo
rle
ad
ersh
ipan
du
nd
erst
an
din
go
f
com
mu
nit
yse
rvic
en
eed
s
HW
ass
um
esre
spo
nsi
bil
itie
sfo
rall
face
tso
fth
ese
rvic
esan
dra
tio
nali
zes
act
ion
s
them
selv
es
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
gre
lati
on
ship
s
Mo
ral
sati
sfact
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
N
ocl
ear
un
der
stan
din
go
fh
ow
pu
bli
cse
cto
rex
ists
E
mer
gen
tp
ract
ices
bec
om
ein
stit
uti
on
ali
zed
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 3
(van Lerberghe et al 2002 Ferrinho et al 2004a) These positive
impacts include increased HW motivation mobilization of
additional resources minimizing the budgetary burden on the
public sector to retain skilled staff as HWs and stabilization of
qualified personnel (van Lerberghe et al 2002 Ferrinho et al
2004a Ferrinho et al 2004b Kiwanuka et al 2011) They also
offer an opportunity to address a number of other difficulties
HWs face in developing countries including poor resource
availability lack of trust for the department of health poor
perceived career opportunities inadequate staffing and a range
of other challenges (Table 1) (Garcıa-Prado and Gonzalez 2007
Kiwanuka et al 2011 Ashmore 2013) Coping mechanisms have
also been typically described as motivated by economic advan-
tage but in PNG a country known for health system
difficulties in implementing even basic programmes (Izard
and Dugue 2003 Thomason 2006 Davy and Patrickson 2012
Tynan et al 2012) evidence also exists that the behaviours of
public servants are influenced by social benefits such as capital
derived from relationships or satisfaction of religious cultural
or moral obligations (van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Jayasuriya 2011 Razee et al 2012
Tynan et al 2013)
This article explores how engaging in unauthorized penile
cutting practices in PNG forms a type of coping strategy that is
not primarily motivated by personal financial gains but the
acquisition and exchange of social currency including mutual
obligation social recognition and prestige professional satis-
faction and self-fulfilment (Macq et al 2001 van Lerberghe
et al 2002) Exploration of HW engagement in penile cutting
practices provides particular and unique insights into coping
mechanisms in PNG Understanding how and why
unauthorized practices exist will not only provide an oppor-
tunity to develop strategies to address concerns or deal with
possible consequences but also provide insight into the extent
of adaptation of health systems to the sociocultural environ-
ment in which they operate
Unauthorized penile cutting in PNG
Penile cutting practices have become of significant interest
since large-scale clinical trials in Africa showed that male
circumcision (MC) has a protective efficacy of around 60 in
preventing HIV acquisition in heterosexual men (Auvert et al
2005 Bailey et al 2007 Gray et al 2007 WHOUNAIDS 2007
Siegfried et al 2009) In some communities where MC for HIV
prevention is being considered evidence exists of a considerable
variety of already established penile cutting practices within
communities that have not been shown to be protective against
HIV (Brown et al 2001 Vincent 2008 Hill et al 2012) That is
these penile cutting practices often do not involve full circum-
ferential cut and removal of the foreskin but rather incisions
that do not alter the size of the foreskin or minimize the
exposure of langerhans cells that have been described as
vulnerable to the HIV virus (McCoombe and Short 2006 Pask
et al 2008 Kigozi et al 2009 Doyle et al 2010) PNG is one such
context where a recent study categorizing the various types of
penile cutting demonstrated that these cuts do not conform
with the guidelines for medical circumcision (Hill et al 2012)
Penile cutting in PNG has a complex history embedded in
religion and traditional ritual and more recently has included
contemporary practices that are the outcome of peer influence
and the evolving sociocultural environment (Williamson 1990
Kempf 2002 MacLaren et al 2011a Hill et al 2012 Kelly et al
2012a Kelly et al 2012b) HWs in PNG have been observed to
be engaging in these penile cutting practices justifying their
actions on both medical and non-medical grounds utilizing
health system resources without the formal approval of the
Department of Health (MacLaren et al 2011b Tynan et al 2011
Hill et al 2012) In a recent study almost a quarter of the 33
frontline HWs interviewed reported regularly engaging in penile
cutting services that operated outside the current regulations of
the PNG health system and a number of other HWs reported
that they were aware of colleagues being involved in
unauthorized penile cutting practices (Tynan et al 2011)
Services included providing instructions on how to perform a
foreskin cut for non-health-related purposes supplying equip-
ment such as spatula scalpel plaster bandage and gauze from
the health facility to men to perform penile cutting at home or
providing penile cutting services to their communities for
contemporary or traditional reasons (Tynan et al 2011) These
findings are supported by another study of 483 PNG men with
a penile foreskin cut for non-health-related reasons who
reported that HWs were the second most likely persons to
have performed the procedure (MacLaren et al 2011b)
Community obligations and other sociocultural responsibil-
ities play an important role in the fabric of many PNG
communities and potentially interface with the health system
(de Renzio 2000 van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Bainton 2008 Reilly and Phillpot
2008) Strong links to community responsibilities have been
shown to outweigh other organizational ties in PNG resulting
in some HWs performing duties outside their role description
(Razee et al 2012 Tynan et al 2013) Further to this the wantok
system in PNGmdashloosely defined as a set of obligations between
individuals of similar geographic origin kinship language
group andor social or religious associationsmdashhas particular
application for engaging in certain practices (de Renzio 2000
Tivinarlik and Wanat 2006 Reilly and Phillpot 2008) In the
public service this clan-based allegiance has been shown to
commonly override the responsibilities of organizational pro-
cesses inadvertently leading to conflict of interest and nepo-
tism within education business and health service networks in
PNG (de Renzio 2000) The wantok system thus serves as a form
of social economy where social capital or resources derived
from specific social structures can be accumulated by actors
(including HWs) within the community and then used to
pursue their own interests (Baker 1990)
MethodsStudy design
This research is part of a multi-disciplinary investigation on the
acceptability and impact of male circumcision for HIV preven-
tion in PNG and used qualitative methods to explore HW
participation in unauthorized penile cutting practices in PNG
Unauthorized practices were defined as those activities that
were not considered a part of a HWrsquos expected role within the
health system or did not conform to standard treating practice
however involved the use of HWrsquos medical skills health system
4 HEALTH POLICY AND PLANNING
supplies or impacted on delivery of other services The quali-
tative research methods included in-depth interviews (IDIs)
with 25 frontline HWs involved in sexual and reproductive
health and data triangulation with findings from an additional
45 focus group discussions (FGDs) and 82 IDIs completed with
community members as part of a wider qualitative study on
community perceptions about masculinity and penile foreskin
cutting and penile modifications in PNG The fieldwork was
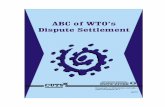
completed in five diverse social and geographical locations
around PNG including Central Province (CP) Eastern
Highlands Province (EHP) East Sepik Province (ESP)
Madang Province (MP) and West New Britain Province
(WNB) from 2009 until 2011 (Figure 1) Approval for the
research was obtained from research ethics committees at both
the PNG Institute of Medical Research (PNGIMR) and the
University of Queensland
Sampling and data collection for fieldwork
An iterative purposive sampling technique was used to identify
potential study participants following initial interviews with key
national and local stakeholders at each study location IDIs and
FGDs were completed with a variety of HWs from various
government and non-government health facilities around PNG
men who had undergone penile cutting inserts or associated
practices and other community leaders who had unique
insights and lived experiences in the study area Interview
guides were developed following extensive literature review and
discussions among the research team and followed a number of
themes including types of services provided and knowledge of
penile foreskin cutting in PNG Interviews were completed
by the in-country research team from the PNGIMR and a
researcher from the University of Queensland Interviews were
conducted in either English or PNG pidgin (the most widely
spoken of PNGrsquos three national languages) as per the partici-
pantrsquos preference digitally recorded transcribed verbatim and
translated into English
Data analysis
The framework analysis method appropriate for the analysis of
qualitative data for policy-oriented studies was used to analyse
the data (Braun and Clarke 2006) All IDIs and FGDs were
initially double coded by the in-country research team at the
PNGIMR In cases of discrepancy in coding a third researcher
coded the selected text in question Preliminary analysis of the
HW interviews showed the differing roles that HWs played in
penile cutting in PNG Themes were further updated as the
analysis developed and organized around identification of
whether respondents discussed unauthorized penile cutting
practices or services that operated outside the rules and
regulations of the health system and reasons for their
participation These themes were further triangulated with
IDIs and FGDs completed with community members to assist in
exploring the interconnections of the sociocultural context in
which the HW was participating Final codes were developed by
the first author and adjusted as required following review from
fellow authors
Figure 1 Map of PNG with study provinces highlighted
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 5
Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

Keywords Coping mechanisms unauthorized practices penile foreskin cutting social
capital Papua New Guinea health system
KEY MESSAGES
Coping mechanisms have been typically described as motivated by economic advantages however in Papua New Guinea
evidence exists that the behaviours of public servants are influenced by capital derived from relationships or satisfaction
of religious cultural or moral obligations
Fragile health systems create opportunities for unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new programmes are introduced
The success of health programmes underpinned by informal systems will not be achieved merely through bureaucratic
regulation but with strategies that encompass and recognize differences within organizational cultures and communities
IntroductionCoping mechanisms are strategies used by health workers
(HWs) to alleviate the burden of unsatisfactory living and
working conditions such as poor supervision inadequate or
intermittent remuneration or working in hostile environments
in low- and middle-income countries (McPake et al 2000
Schwalbach et al 2000 Macq et al 2001 van Lerberghe et al
2002 Ferrinho et al 2004a) Along with health system failures
coping mechanisms are shaped by social political and institu-
tional environments in which HWs operate and are as import-
ant in shaping how health services function and are perceived
as are planned health reforms and management (Roenen et al
1997 Schwalbach et al 2000 Macq et al 2001 van Lerberghe
et al 2002) Coping mechanisms include unauthorized practices
or activities that fall outside standard treating practices that can
impact on service delivery and may include illegal and non-
illegal activities This article will examine Papua New Guinean
(PNG) HWs engagement in unauthorized penile cutting
activities
Coping mechanisms and their relationship withhealth systems
Coping mechanisms arise due to extreme discrepancies between
social economic and professional expectations of HWs and real-
life situations (Table 1) (Schwalbach et al 2000 van Lerberghe
et al 2002 Garcıa-Prado and Gonzalez 2007) There are a
number of different types of coping mechanisms which are
described in the literature These include HWs receiving
informal payments or under-the-counter payments for other-
wise free services (Delcheva et al 1997 Giedion et al 2001
Falkingham 2004 Lindelow and Serneels 2006 Tediosi 2008
Liu and Sun 2012) misappropriating drugs or other supplies
(Israr et al 2000 Ferrinho et al 2004a Lindelow and Serneels
2006) moonlighting in other roles or dual practice (Ferrinho
et al 2004a Jan et al 2005 Gonzalez and Macho-Stadler 2013)
preferential treatment including accelerated access to health
services for friends family or those who are able to afford
bribes or under-the-counter payments (Roenen et al 1997) and
other unexplained absenteeism (Chaudhury et al 2005 Manzi
et al 2012) There has also been a move to acknowledge other
potential coping strategies for HWs such as receiving in-kind or
in-gratitude payments like access to accommodation or food for
services they perform (Roenen et al 1997 Chereches et al
2013) using time or resourcesmdashsuch as health service ve-
hiclesmdashfrom government projects for personal use (McPake
et al 1999 Macq et al 2001 Ferrinho et al 2004b) and
exploitation of allowances and per diems designed to enable
supervision or attendance at courses (McCoy et al 2008 Smith
2003 Vian et al 2011)
Engagement in coping mechanisms has consequences for the
equity and efficiency of health systems and quality of health
care (Garcıa-Prado and Gonzalez 2007 Jumpa et al 2007
Kiwanuka et al 2011) Health system impacts include compe-
tition for time (due to HWs being less available at public
facilities thereby compromising service delivery) conflict of
interest (for example when HWs lower the quality of services
they provide in the public sector in order to drive patients to the
private sector) and brain drain (or inequitable distribution of
HWs between public and private rural and urban primary and
tertiary and poor and rich settings) (Macq et al 2001 van
Lerberghe et al 2002 Ferrinho et al 2004b Kiwanuka et al
2011 Ashmore 2013) Misuse by HWs of their privileged access
to resources such as pharmaceuticals contributes to financial
losses in the health-care system as well as the growing sense of
mistrust and disrespect for HWs and their institutions
(Ferrinho et al 2004a) Informal payments or under-the-counter
payments provide a financial barrier to those who canrsquot afford
to pay and as a result again jeopardize the necessary trust
between user and provider and public expectations of health
service delivery (van Lerberghe et al 2002 Dabalen and Wane
2008) Inappropriate or unnecessary attendance at training
sessions primarily to obtain the per diem allowances creates
inefficiencies in health systems including reduced HW avail-
ability (van Lerberghe et al 2002 Conteh and Kingori 2010
Vian et al 2011)
Although coping mechanisms may be considered a part of
corrupt practices of government employees or labelled as the
result of poor motivation or inefficient practice there is
evidence that coping mechanisms are not necessarily due to
predatory behaviour but a strategy to deal with difficult
situations that can have positive impacts as well
2 HEALTH POLICY AND PLANNING
Ta
ble
1
Typ
eso
fco
pin
gst
rate
gie
sam
on
gH
Ws
curr
ency
exch
an
ged
an
dim
pact
on
hea
lth
syst
em
Are
ao
rp
roce
sso
fh
ea
lth
syst
em
fail
ure
Co
pin
gst
rate
gy
Typ
es
of
curr
en
cye
xch
an
ge
dP
oss
ible
resu
lt
Hu
man
reso
urc
ing
In
ad
equ
ate
hu
man
reso
urc
ing
In
ad
equ
ate
train
ing
an
dsu
per
visi
on
of
HW
s
Lack
of
com
pu
lso
ryed
uca
tio
n
H
Wass
um
eso
ther
role
san
dre
spo
nsi
-
bil
itie
so
uts
ide
train
ing
R
elia
nce
on
info
rmal
net
wo
rks
for
gu
id-
an
ceo
nap
pro
pri
ate
pra
ctic
e
Reg
ula
ratt
end
an
ceat
wo
rksh
op
san
dtr
ain
ing
(in
clu
din
go
vers
eas)
S
oci
al
reco
gn
itio
nan
dp
rest
ige
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
P
rofe
ssio
nal
sati
sfact
ion
an
dse
lf-
fulf
ilm
ent
thro
ugh
ach
ievi
ng
oth
ersk
ills
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
In
crea
sed
com
pli
cati
on
s
Red
uce
dco
mm
un
ity
tru
stin
hea
lth
wo
rker
san
dth
eir
inst
itu
tio
ns
H
Wst
ress
an
dd
issa
tisf
act
ion
wit
hh
ealt
h
syst
em
Hea
lth
fin
an
cin
g
L
imit
edfu
nd
ing
for
serv
ice
D
iffi
cult
ies
ob
tain
ing
fun
din
g
Lo
ww
ages
H
Ws
rece
ivin
gin
form
al
paym
ents
for
oth
erw
ise
free
serv
ice
R
ecei
vin
ggif
tslsquoi
nk
ind
rsquo
Mo
on
ligh
tin
gin
oth
erro
les
incl
ud
ing
pri
vate
hea
lth
sect
or
or
agri
cult
ure
usi
ng
tim
eo
rre
sou
rces
fro
mgo
vern
men
t
pro
ject
s
Pil
feri
ng
dru
gs
an
dm
edic
ines
P
erd
iem
sfo
rtr
ave
lan
dtr
ain
ing
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
Pro
fess
ion
al
sati
sfact
ion
an
dse
lf-f
ulf
il-
men
tb
yp
art
icip
ati
ng
ino
ther
role
s
So
cial
use
skil
lsas
HW
togain
com
mu
-n
ity
pre
stig
ean
dre
cogn
itio
n
C
om
pet
itio
nfo
rti
me
O
utf
low
of
reso
urc
esfr
om
the
pu
bli
c
sect
or
C
on
flic
tso
fin
tere
st
Hig
hp
rice
of
hea
lth
care
D
iscr
imin
ati
on
of
pati
ents
acc
ord
ing
to
cap
aci
tyto
pay
In
ad
equ
ate
serv
ice
del
iver
y
Med
icin
esan
dte
chn
olo
gy
In
suff
icie
nt
med
icin
esan
dte
chn
ical
equ
ipm
ent
for
the
man
agem
ent
of
pate
nts
G
ener
al
lack
of
basi
csu
pp
lies
M
isap
pro
pri
ati
ng
dru
gs
or
oth
ersu
pp
lies
for
fam
ily
or
oth
eracq
uain
tan
ces
O
verc
harg
ing
pati
ents
for
dru
gs
an
d
oth
ersu
pp
lies
H
Ws
usi
ng
reso
urc
esto
pro
vid
eu
nre
c-o
gn
ized
ad
dit
ion
al
serv
ices
of
the
org
an
izati
on
S
oci
al
usi
ng
acc
ess
tore
sou
rces
as
aH
W
tosa
tisf
yco
mm
un
ity
or
cult
ura
lo
bli
gati
on
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
Deg
rad
ati
on
of
qu
ali
tyca
re
Co
un
terf
eit
dru
gs
F
inan
cial
loss
toth
eh
ealt
hsy
stem
Hea
lth
info
rmati
on
syst
ems
P
oo
racc
ou
nta
bil
ity
an
dre
cord
kee
pin
g
Lim
ited
acc
ess
top
rofe
ssio
nal
dev
elo
p-
men
tan
dre
sou
rces
U
nex
pla
ined
ab
sen
teei
sm
Eco
no
mic
su
pp
lem
ent
low
sala
ries
wit
h
cash
an
dtr
ad
itio
nal
eco
no
mie
s
So
cial
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s
fost
erin
gre
lati
on
ship
s
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
W
ork
do
ne
inp
riva
tese
cto
rn
ot
cap
ture
d
Hea
lth
serv
ices
L
imit
edse
rvic
eava
ilab
ilit
y
Po
or
wo
rkin
gco
nd
itio
ns
incl
ud
ing
po
or
faci
liti
esan
dre
sou
rces
W
ork
ing
inch
all
engin
gan
dd
an
ger
ou
s
envi
ron
men
ts
N
epo
tism
for
bet
ter
hea
lth
serv
ice
F
aci
lita
tio
no
fq
ueu
eju
mp
ing
for
rela
-
tive
san
dfr
ien
ds
S
oci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs
Un
exp
lain
edab
sen
teei
sm
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
g
rela
tio
nsh
ips
E
con
om
ic
acc
ess
totr
ad
itio
nal
eco
no
my
or
lsquoin
kin
drsquo
paym
ents
D
iscr
imin
ato
ryp
ract
ice
L
ow
uti
liza
tio
no
fse
rvic
e
Sta
teH
Ws
bec
om
ele
ssava
ilab
leto
wo
rk
inth
ep
ub
lic
sect
or
bu
td
on
ot
resi
gn
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
HW
fati
gu
e
Lea
der
ship
an
dgo
vern
an
ce
P
oo
rle
ad
ersh
ipan
du
nd
erst
an
din
go
f
com
mu
nit
yse
rvic
en
eed
s
HW
ass
um
esre
spo
nsi
bil
itie
sfo
rall
face
tso
fth
ese
rvic
esan
dra
tio
nali
zes
act
ion
s
them
selv
es
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
gre
lati
on
ship
s
Mo
ral
sati
sfact
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
N
ocl
ear
un
der
stan
din
go
fh
ow
pu
bli
cse
cto
rex
ists
E
mer
gen
tp
ract
ices
bec
om
ein
stit
uti
on
ali
zed
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 3
(van Lerberghe et al 2002 Ferrinho et al 2004a) These positive
impacts include increased HW motivation mobilization of
additional resources minimizing the budgetary burden on the
public sector to retain skilled staff as HWs and stabilization of
qualified personnel (van Lerberghe et al 2002 Ferrinho et al
2004a Ferrinho et al 2004b Kiwanuka et al 2011) They also
offer an opportunity to address a number of other difficulties
HWs face in developing countries including poor resource
availability lack of trust for the department of health poor
perceived career opportunities inadequate staffing and a range
of other challenges (Table 1) (Garcıa-Prado and Gonzalez 2007
Kiwanuka et al 2011 Ashmore 2013) Coping mechanisms have
also been typically described as motivated by economic advan-
tage but in PNG a country known for health system
difficulties in implementing even basic programmes (Izard
and Dugue 2003 Thomason 2006 Davy and Patrickson 2012
Tynan et al 2012) evidence also exists that the behaviours of
public servants are influenced by social benefits such as capital
derived from relationships or satisfaction of religious cultural
or moral obligations (van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Jayasuriya 2011 Razee et al 2012
Tynan et al 2013)
This article explores how engaging in unauthorized penile
cutting practices in PNG forms a type of coping strategy that is
not primarily motivated by personal financial gains but the
acquisition and exchange of social currency including mutual
obligation social recognition and prestige professional satis-
faction and self-fulfilment (Macq et al 2001 van Lerberghe
et al 2002) Exploration of HW engagement in penile cutting
practices provides particular and unique insights into coping
mechanisms in PNG Understanding how and why
unauthorized practices exist will not only provide an oppor-
tunity to develop strategies to address concerns or deal with
possible consequences but also provide insight into the extent
of adaptation of health systems to the sociocultural environ-
ment in which they operate
Unauthorized penile cutting in PNG
Penile cutting practices have become of significant interest
since large-scale clinical trials in Africa showed that male
circumcision (MC) has a protective efficacy of around 60 in
preventing HIV acquisition in heterosexual men (Auvert et al
2005 Bailey et al 2007 Gray et al 2007 WHOUNAIDS 2007
Siegfried et al 2009) In some communities where MC for HIV
prevention is being considered evidence exists of a considerable
variety of already established penile cutting practices within
communities that have not been shown to be protective against
HIV (Brown et al 2001 Vincent 2008 Hill et al 2012) That is
these penile cutting practices often do not involve full circum-
ferential cut and removal of the foreskin but rather incisions
that do not alter the size of the foreskin or minimize the
exposure of langerhans cells that have been described as
vulnerable to the HIV virus (McCoombe and Short 2006 Pask
et al 2008 Kigozi et al 2009 Doyle et al 2010) PNG is one such
context where a recent study categorizing the various types of
penile cutting demonstrated that these cuts do not conform
with the guidelines for medical circumcision (Hill et al 2012)
Penile cutting in PNG has a complex history embedded in
religion and traditional ritual and more recently has included
contemporary practices that are the outcome of peer influence
and the evolving sociocultural environment (Williamson 1990
Kempf 2002 MacLaren et al 2011a Hill et al 2012 Kelly et al
2012a Kelly et al 2012b) HWs in PNG have been observed to
be engaging in these penile cutting practices justifying their
actions on both medical and non-medical grounds utilizing
health system resources without the formal approval of the
Department of Health (MacLaren et al 2011b Tynan et al 2011
Hill et al 2012) In a recent study almost a quarter of the 33
frontline HWs interviewed reported regularly engaging in penile
cutting services that operated outside the current regulations of
the PNG health system and a number of other HWs reported
that they were aware of colleagues being involved in
unauthorized penile cutting practices (Tynan et al 2011)
Services included providing instructions on how to perform a
foreskin cut for non-health-related purposes supplying equip-
ment such as spatula scalpel plaster bandage and gauze from
the health facility to men to perform penile cutting at home or
providing penile cutting services to their communities for
contemporary or traditional reasons (Tynan et al 2011) These
findings are supported by another study of 483 PNG men with
a penile foreskin cut for non-health-related reasons who
reported that HWs were the second most likely persons to
have performed the procedure (MacLaren et al 2011b)
Community obligations and other sociocultural responsibil-
ities play an important role in the fabric of many PNG
communities and potentially interface with the health system
(de Renzio 2000 van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Bainton 2008 Reilly and Phillpot
2008) Strong links to community responsibilities have been
shown to outweigh other organizational ties in PNG resulting
in some HWs performing duties outside their role description
(Razee et al 2012 Tynan et al 2013) Further to this the wantok
system in PNGmdashloosely defined as a set of obligations between
individuals of similar geographic origin kinship language
group andor social or religious associationsmdashhas particular
application for engaging in certain practices (de Renzio 2000
Tivinarlik and Wanat 2006 Reilly and Phillpot 2008) In the
public service this clan-based allegiance has been shown to
commonly override the responsibilities of organizational pro-
cesses inadvertently leading to conflict of interest and nepo-
tism within education business and health service networks in
PNG (de Renzio 2000) The wantok system thus serves as a form
of social economy where social capital or resources derived
from specific social structures can be accumulated by actors
(including HWs) within the community and then used to
pursue their own interests (Baker 1990)
MethodsStudy design
This research is part of a multi-disciplinary investigation on the
acceptability and impact of male circumcision for HIV preven-
tion in PNG and used qualitative methods to explore HW
participation in unauthorized penile cutting practices in PNG
Unauthorized practices were defined as those activities that
were not considered a part of a HWrsquos expected role within the
health system or did not conform to standard treating practice
however involved the use of HWrsquos medical skills health system
4 HEALTH POLICY AND PLANNING
supplies or impacted on delivery of other services The quali-
tative research methods included in-depth interviews (IDIs)
with 25 frontline HWs involved in sexual and reproductive
health and data triangulation with findings from an additional
45 focus group discussions (FGDs) and 82 IDIs completed with
community members as part of a wider qualitative study on
community perceptions about masculinity and penile foreskin
cutting and penile modifications in PNG The fieldwork was
completed in five diverse social and geographical locations
around PNG including Central Province (CP) Eastern
Highlands Province (EHP) East Sepik Province (ESP)
Madang Province (MP) and West New Britain Province
(WNB) from 2009 until 2011 (Figure 1) Approval for the
research was obtained from research ethics committees at both
the PNG Institute of Medical Research (PNGIMR) and the
University of Queensland
Sampling and data collection for fieldwork
An iterative purposive sampling technique was used to identify
potential study participants following initial interviews with key
national and local stakeholders at each study location IDIs and
FGDs were completed with a variety of HWs from various
government and non-government health facilities around PNG
men who had undergone penile cutting inserts or associated
practices and other community leaders who had unique
insights and lived experiences in the study area Interview
guides were developed following extensive literature review and
discussions among the research team and followed a number of
themes including types of services provided and knowledge of
penile foreskin cutting in PNG Interviews were completed
by the in-country research team from the PNGIMR and a
researcher from the University of Queensland Interviews were
conducted in either English or PNG pidgin (the most widely
spoken of PNGrsquos three national languages) as per the partici-
pantrsquos preference digitally recorded transcribed verbatim and
translated into English
Data analysis
The framework analysis method appropriate for the analysis of
qualitative data for policy-oriented studies was used to analyse
the data (Braun and Clarke 2006) All IDIs and FGDs were
initially double coded by the in-country research team at the
PNGIMR In cases of discrepancy in coding a third researcher
coded the selected text in question Preliminary analysis of the
HW interviews showed the differing roles that HWs played in
penile cutting in PNG Themes were further updated as the
analysis developed and organized around identification of
whether respondents discussed unauthorized penile cutting
practices or services that operated outside the rules and
regulations of the health system and reasons for their
participation These themes were further triangulated with
IDIs and FGDs completed with community members to assist in
exploring the interconnections of the sociocultural context in
which the HW was participating Final codes were developed by
the first author and adjusted as required following review from
fellow authors
Figure 1 Map of PNG with study provinces highlighted
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 5
Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

Ta
ble
1
Typ
eso
fco
pin
gst
rate
gie
sam
on
gH
Ws
curr
ency
exch
an
ged
an
dim
pact
on
hea
lth
syst
em
Are
ao
rp
roce
sso
fh
ea
lth
syst
em
fail
ure
Co
pin
gst
rate
gy
Typ
es
of
curr
en
cye
xch
an
ge
dP
oss
ible
resu
lt
Hu
man
reso
urc
ing
In
ad
equ
ate
hu
man
reso
urc
ing
In
ad
equ
ate
train
ing
an
dsu
per
visi
on
of
HW
s
Lack
of
com
pu
lso
ryed
uca
tio
n
H
Wass
um
eso
ther
role
san
dre
spo
nsi
-
bil
itie
so
uts
ide
train
ing
R
elia
nce
on
info
rmal
net
wo
rks
for
gu
id-
an
ceo
nap
pro
pri
ate
pra
ctic
e
Reg
ula
ratt
end
an
ceat
wo
rksh
op
san
dtr
ain
ing
(in
clu
din
go
vers
eas)
S
oci
al
reco
gn
itio
nan
dp
rest
ige
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
P
rofe
ssio
nal
sati
sfact
ion
an
dse
lf-
fulf
ilm
ent
thro
ugh
ach
ievi
ng
oth
ersk
ills
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
In
crea
sed
com
pli
cati
on
s
Red
uce
dco
mm
un
ity
tru
stin
hea
lth
wo
rker
san
dth
eir
inst
itu
tio
ns
H
Wst
ress
an
dd
issa
tisf
act
ion
wit
hh
ealt
h
syst
em
Hea
lth
fin
an
cin
g
L
imit
edfu
nd
ing
for
serv
ice
D
iffi
cult
ies
ob
tain
ing
fun
din
g
Lo
ww
ages
H
Ws
rece
ivin
gin
form
al
paym
ents
for
oth
erw
ise
free
serv
ice
R
ecei
vin
ggif
tslsquoi
nk
ind
rsquo
Mo
on
ligh
tin
gin
oth
erro
les
incl
ud
ing
pri
vate
hea
lth
sect
or
or
agri
cult
ure
usi
ng
tim
eo
rre
sou
rces
fro
mgo
vern
men
t
pro
ject
s
Pil
feri
ng
dru
gs
an
dm
edic
ines
P
erd
iem
sfo
rtr
ave
lan
dtr
ain
ing
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
Pro
fess
ion
al
sati
sfact
ion
an
dse
lf-f
ulf
il-
men
tb
yp
art
icip
ati
ng
ino
ther
role
s
So
cial
use
skil
lsas
HW
togain
com
mu
-n
ity
pre
stig
ean
dre
cogn
itio
n
C
om
pet
itio
nfo
rti
me
O
utf
low
of
reso
urc
esfr
om
the
pu
bli
c
sect
or
C
on
flic
tso
fin
tere
st
Hig
hp
rice
of
hea
lth
care
D
iscr
imin
ati
on
of
pati
ents
acc
ord
ing
to
cap
aci
tyto
pay
In
ad
equ
ate
serv
ice
del
iver
y
Med
icin
esan
dte
chn
olo
gy
In
suff
icie
nt
med
icin
esan
dte
chn
ical
equ
ipm
ent
for
the
man
agem
ent
of
pate
nts
G
ener
al
lack
of
basi
csu
pp
lies
M
isap
pro
pri
ati
ng
dru
gs
or
oth
ersu
pp
lies
for
fam
ily
or
oth
eracq
uain
tan
ces
O
verc
harg
ing
pati
ents
for
dru
gs
an
d
oth
ersu
pp
lies
H
Ws
usi
ng
reso
urc
esto
pro
vid
eu
nre
c-o
gn
ized
ad
dit
ion
al
serv
ices
of
the
org
an
izati
on
S
oci
al
usi
ng
acc
ess
tore
sou
rces
as
aH
W
tosa
tisf
yco
mm
un
ity
or
cult
ura
lo
bli
gati
on
M
ora
lsa
tisf
act
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
E
con
om
ic
sup
ple
men
tlo
wsa
lari
esw
ith
cash
an
dtr
ad
itio
nal
eco
no
mie
s
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
Deg
rad
ati
on
of
qu
ali
tyca
re
Co
un
terf
eit
dru
gs
F
inan
cial
loss
toth
eh
ealt
hsy
stem
Hea
lth
info
rmati
on
syst
ems
P
oo
racc
ou
nta
bil
ity
an
dre
cord
kee
pin
g
Lim
ited
acc
ess
top
rofe
ssio
nal
dev
elo
p-
men
tan
dre
sou
rces
U
nex
pla
ined
ab
sen
teei
sm
Eco
no
mic
su
pp
lem
ent
low
sala
ries
wit
h
cash
an
dtr
ad
itio
nal
eco
no
mie
s
So
cial
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s
fost
erin
gre
lati
on
ship
s
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
W
ork
do
ne
inp
riva
tese
cto
rn
ot
cap
ture
d
Hea
lth
serv
ices
L
imit
edse
rvic
eava
ilab
ilit
y
Po
or
wo
rkin
gco
nd
itio
ns
incl
ud
ing
po
or
faci
liti
esan
dre
sou
rces
W
ork
ing
inch
all
engin
gan
dd
an
ger
ou
s
envi
ron
men
ts
N
epo
tism
for
bet
ter
hea
lth
serv
ice
F
aci
lita
tio
no
fq
ueu
eju
mp
ing
for
rela
-
tive
san
dfr
ien
ds
S
oci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs
Un
exp
lain
edab
sen
teei
sm
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
g
rela
tio
nsh
ips
E
con
om
ic
acc
ess
totr
ad
itio
nal
eco
no
my
or
lsquoin
kin
drsquo
paym
ents
D
iscr
imin
ato
ryp
ract
ice
L
ow
uti
liza
tio
no
fse
rvic
e
Sta
teH
Ws
bec
om
ele
ssava
ilab
leto
wo
rk
inth
ep
ub
lic
sect
or
bu
td
on
ot
resi
gn
L
ow
qu
ali
tyo
fd
iagn
osi
san
dp
resc
rip
tio
n
HW
fati
gu
e
Lea
der
ship
an
dgo
vern
an
ce
P
oo
rle
ad
ersh
ipan
du
nd
erst
an
din
go
f
com
mu
nit
yse
rvic
en
eed
s
HW
ass
um
esre
spo
nsi
bil
itie
sfo
rall
face
tso
fth
ese
rvic
esan
dra
tio
nali
zes
act
ion
s
them
selv
es
S
oci
al
sati
sfact
ion
of
cult
ura
lo
bli
gati
on
s(i
ncl
ud
ing
soci
al
pre
ssu
reto
get
spec
ial
trea
tmen
to
ro
ther
sfa
vou
rs)
fost
erin
gre
lati
on
ship
s
Mo
ral
sati
sfact
ion
of
Hip
po
crati
co
ath
or
reli
gio
us
con
vict
ion
tose
rve
G
ener
al
inef
fici
ency
of
hea
lth
serv
ice
N
ocl
ear
un
der
stan
din
go
fh
ow
pu
bli
cse
cto
rex
ists
E
mer
gen
tp
ract
ices
bec
om
ein
stit
uti
on
ali
zed
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 3
(van Lerberghe et al 2002 Ferrinho et al 2004a) These positive
impacts include increased HW motivation mobilization of
additional resources minimizing the budgetary burden on the
public sector to retain skilled staff as HWs and stabilization of
qualified personnel (van Lerberghe et al 2002 Ferrinho et al
2004a Ferrinho et al 2004b Kiwanuka et al 2011) They also
offer an opportunity to address a number of other difficulties
HWs face in developing countries including poor resource
availability lack of trust for the department of health poor
perceived career opportunities inadequate staffing and a range
of other challenges (Table 1) (Garcıa-Prado and Gonzalez 2007
Kiwanuka et al 2011 Ashmore 2013) Coping mechanisms have
also been typically described as motivated by economic advan-
tage but in PNG a country known for health system
difficulties in implementing even basic programmes (Izard
and Dugue 2003 Thomason 2006 Davy and Patrickson 2012
Tynan et al 2012) evidence also exists that the behaviours of
public servants are influenced by social benefits such as capital
derived from relationships or satisfaction of religious cultural
or moral obligations (van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Jayasuriya 2011 Razee et al 2012
Tynan et al 2013)
This article explores how engaging in unauthorized penile
cutting practices in PNG forms a type of coping strategy that is
not primarily motivated by personal financial gains but the
acquisition and exchange of social currency including mutual
obligation social recognition and prestige professional satis-
faction and self-fulfilment (Macq et al 2001 van Lerberghe
et al 2002) Exploration of HW engagement in penile cutting
practices provides particular and unique insights into coping
mechanisms in PNG Understanding how and why
unauthorized practices exist will not only provide an oppor-
tunity to develop strategies to address concerns or deal with
possible consequences but also provide insight into the extent
of adaptation of health systems to the sociocultural environ-
ment in which they operate
Unauthorized penile cutting in PNG
Penile cutting practices have become of significant interest
since large-scale clinical trials in Africa showed that male
circumcision (MC) has a protective efficacy of around 60 in
preventing HIV acquisition in heterosexual men (Auvert et al
2005 Bailey et al 2007 Gray et al 2007 WHOUNAIDS 2007
Siegfried et al 2009) In some communities where MC for HIV
prevention is being considered evidence exists of a considerable
variety of already established penile cutting practices within
communities that have not been shown to be protective against
HIV (Brown et al 2001 Vincent 2008 Hill et al 2012) That is
these penile cutting practices often do not involve full circum-
ferential cut and removal of the foreskin but rather incisions
that do not alter the size of the foreskin or minimize the
exposure of langerhans cells that have been described as
vulnerable to the HIV virus (McCoombe and Short 2006 Pask
et al 2008 Kigozi et al 2009 Doyle et al 2010) PNG is one such
context where a recent study categorizing the various types of
penile cutting demonstrated that these cuts do not conform
with the guidelines for medical circumcision (Hill et al 2012)
Penile cutting in PNG has a complex history embedded in
religion and traditional ritual and more recently has included
contemporary practices that are the outcome of peer influence
and the evolving sociocultural environment (Williamson 1990
Kempf 2002 MacLaren et al 2011a Hill et al 2012 Kelly et al
2012a Kelly et al 2012b) HWs in PNG have been observed to
be engaging in these penile cutting practices justifying their
actions on both medical and non-medical grounds utilizing
health system resources without the formal approval of the
Department of Health (MacLaren et al 2011b Tynan et al 2011
Hill et al 2012) In a recent study almost a quarter of the 33
frontline HWs interviewed reported regularly engaging in penile
cutting services that operated outside the current regulations of
the PNG health system and a number of other HWs reported
that they were aware of colleagues being involved in
unauthorized penile cutting practices (Tynan et al 2011)
Services included providing instructions on how to perform a
foreskin cut for non-health-related purposes supplying equip-
ment such as spatula scalpel plaster bandage and gauze from
the health facility to men to perform penile cutting at home or
providing penile cutting services to their communities for
contemporary or traditional reasons (Tynan et al 2011) These
findings are supported by another study of 483 PNG men with
a penile foreskin cut for non-health-related reasons who
reported that HWs were the second most likely persons to
have performed the procedure (MacLaren et al 2011b)
Community obligations and other sociocultural responsibil-
ities play an important role in the fabric of many PNG
communities and potentially interface with the health system
(de Renzio 2000 van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Bainton 2008 Reilly and Phillpot
2008) Strong links to community responsibilities have been
shown to outweigh other organizational ties in PNG resulting
in some HWs performing duties outside their role description
(Razee et al 2012 Tynan et al 2013) Further to this the wantok
system in PNGmdashloosely defined as a set of obligations between
individuals of similar geographic origin kinship language
group andor social or religious associationsmdashhas particular
application for engaging in certain practices (de Renzio 2000
Tivinarlik and Wanat 2006 Reilly and Phillpot 2008) In the
public service this clan-based allegiance has been shown to
commonly override the responsibilities of organizational pro-
cesses inadvertently leading to conflict of interest and nepo-
tism within education business and health service networks in
PNG (de Renzio 2000) The wantok system thus serves as a form
of social economy where social capital or resources derived
from specific social structures can be accumulated by actors
(including HWs) within the community and then used to
pursue their own interests (Baker 1990)
MethodsStudy design
This research is part of a multi-disciplinary investigation on the
acceptability and impact of male circumcision for HIV preven-
tion in PNG and used qualitative methods to explore HW
participation in unauthorized penile cutting practices in PNG
Unauthorized practices were defined as those activities that
were not considered a part of a HWrsquos expected role within the
health system or did not conform to standard treating practice
however involved the use of HWrsquos medical skills health system
4 HEALTH POLICY AND PLANNING
supplies or impacted on delivery of other services The quali-
tative research methods included in-depth interviews (IDIs)
with 25 frontline HWs involved in sexual and reproductive
health and data triangulation with findings from an additional
45 focus group discussions (FGDs) and 82 IDIs completed with
community members as part of a wider qualitative study on
community perceptions about masculinity and penile foreskin
cutting and penile modifications in PNG The fieldwork was
completed in five diverse social and geographical locations
around PNG including Central Province (CP) Eastern
Highlands Province (EHP) East Sepik Province (ESP)
Madang Province (MP) and West New Britain Province
(WNB) from 2009 until 2011 (Figure 1) Approval for the
research was obtained from research ethics committees at both
the PNG Institute of Medical Research (PNGIMR) and the
University of Queensland
Sampling and data collection for fieldwork
An iterative purposive sampling technique was used to identify
potential study participants following initial interviews with key
national and local stakeholders at each study location IDIs and
FGDs were completed with a variety of HWs from various
government and non-government health facilities around PNG
men who had undergone penile cutting inserts or associated
practices and other community leaders who had unique
insights and lived experiences in the study area Interview
guides were developed following extensive literature review and
discussions among the research team and followed a number of
themes including types of services provided and knowledge of
penile foreskin cutting in PNG Interviews were completed
by the in-country research team from the PNGIMR and a
researcher from the University of Queensland Interviews were
conducted in either English or PNG pidgin (the most widely
spoken of PNGrsquos three national languages) as per the partici-
pantrsquos preference digitally recorded transcribed verbatim and
translated into English
Data analysis
The framework analysis method appropriate for the analysis of
qualitative data for policy-oriented studies was used to analyse
the data (Braun and Clarke 2006) All IDIs and FGDs were
initially double coded by the in-country research team at the
PNGIMR In cases of discrepancy in coding a third researcher
coded the selected text in question Preliminary analysis of the
HW interviews showed the differing roles that HWs played in
penile cutting in PNG Themes were further updated as the
analysis developed and organized around identification of
whether respondents discussed unauthorized penile cutting
practices or services that operated outside the rules and
regulations of the health system and reasons for their
participation These themes were further triangulated with
IDIs and FGDs completed with community members to assist in
exploring the interconnections of the sociocultural context in
which the HW was participating Final codes were developed by
the first author and adjusted as required following review from
fellow authors
Figure 1 Map of PNG with study provinces highlighted
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 5
Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

(van Lerberghe et al 2002 Ferrinho et al 2004a) These positive
impacts include increased HW motivation mobilization of
additional resources minimizing the budgetary burden on the
public sector to retain skilled staff as HWs and stabilization of
qualified personnel (van Lerberghe et al 2002 Ferrinho et al
2004a Ferrinho et al 2004b Kiwanuka et al 2011) They also
offer an opportunity to address a number of other difficulties
HWs face in developing countries including poor resource
availability lack of trust for the department of health poor
perceived career opportunities inadequate staffing and a range
of other challenges (Table 1) (Garcıa-Prado and Gonzalez 2007
Kiwanuka et al 2011 Ashmore 2013) Coping mechanisms have
also been typically described as motivated by economic advan-
tage but in PNG a country known for health system
difficulties in implementing even basic programmes (Izard
and Dugue 2003 Thomason 2006 Davy and Patrickson 2012
Tynan et al 2012) evidence also exists that the behaviours of
public servants are influenced by social benefits such as capital
derived from relationships or satisfaction of religious cultural
or moral obligations (van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Jayasuriya 2011 Razee et al 2012
Tynan et al 2013)
This article explores how engaging in unauthorized penile
cutting practices in PNG forms a type of coping strategy that is
not primarily motivated by personal financial gains but the
acquisition and exchange of social currency including mutual
obligation social recognition and prestige professional satis-
faction and self-fulfilment (Macq et al 2001 van Lerberghe
et al 2002) Exploration of HW engagement in penile cutting
practices provides particular and unique insights into coping
mechanisms in PNG Understanding how and why
unauthorized practices exist will not only provide an oppor-
tunity to develop strategies to address concerns or deal with
possible consequences but also provide insight into the extent
of adaptation of health systems to the sociocultural environ-
ment in which they operate
Unauthorized penile cutting in PNG
Penile cutting practices have become of significant interest
since large-scale clinical trials in Africa showed that male
circumcision (MC) has a protective efficacy of around 60 in
preventing HIV acquisition in heterosexual men (Auvert et al
2005 Bailey et al 2007 Gray et al 2007 WHOUNAIDS 2007
Siegfried et al 2009) In some communities where MC for HIV
prevention is being considered evidence exists of a considerable
variety of already established penile cutting practices within
communities that have not been shown to be protective against
HIV (Brown et al 2001 Vincent 2008 Hill et al 2012) That is
these penile cutting practices often do not involve full circum-
ferential cut and removal of the foreskin but rather incisions
that do not alter the size of the foreskin or minimize the
exposure of langerhans cells that have been described as
vulnerable to the HIV virus (McCoombe and Short 2006 Pask
et al 2008 Kigozi et al 2009 Doyle et al 2010) PNG is one such
context where a recent study categorizing the various types of
penile cutting demonstrated that these cuts do not conform
with the guidelines for medical circumcision (Hill et al 2012)
Penile cutting in PNG has a complex history embedded in
religion and traditional ritual and more recently has included
contemporary practices that are the outcome of peer influence
and the evolving sociocultural environment (Williamson 1990
Kempf 2002 MacLaren et al 2011a Hill et al 2012 Kelly et al
2012a Kelly et al 2012b) HWs in PNG have been observed to
be engaging in these penile cutting practices justifying their
actions on both medical and non-medical grounds utilizing
health system resources without the formal approval of the
Department of Health (MacLaren et al 2011b Tynan et al 2011
Hill et al 2012) In a recent study almost a quarter of the 33
frontline HWs interviewed reported regularly engaging in penile
cutting services that operated outside the current regulations of
the PNG health system and a number of other HWs reported
that they were aware of colleagues being involved in
unauthorized penile cutting practices (Tynan et al 2011)
Services included providing instructions on how to perform a
foreskin cut for non-health-related purposes supplying equip-
ment such as spatula scalpel plaster bandage and gauze from
the health facility to men to perform penile cutting at home or
providing penile cutting services to their communities for
contemporary or traditional reasons (Tynan et al 2011) These
findings are supported by another study of 483 PNG men with
a penile foreskin cut for non-health-related reasons who
reported that HWs were the second most likely persons to
have performed the procedure (MacLaren et al 2011b)
Community obligations and other sociocultural responsibil-
ities play an important role in the fabric of many PNG
communities and potentially interface with the health system
(de Renzio 2000 van Amstela and van der Geest 2004
Tivinarlik and Wanat 2006 Bainton 2008 Reilly and Phillpot
2008) Strong links to community responsibilities have been
shown to outweigh other organizational ties in PNG resulting
in some HWs performing duties outside their role description
(Razee et al 2012 Tynan et al 2013) Further to this the wantok
system in PNGmdashloosely defined as a set of obligations between
individuals of similar geographic origin kinship language
group andor social or religious associationsmdashhas particular
application for engaging in certain practices (de Renzio 2000
Tivinarlik and Wanat 2006 Reilly and Phillpot 2008) In the
public service this clan-based allegiance has been shown to
commonly override the responsibilities of organizational pro-
cesses inadvertently leading to conflict of interest and nepo-
tism within education business and health service networks in
PNG (de Renzio 2000) The wantok system thus serves as a form
of social economy where social capital or resources derived
from specific social structures can be accumulated by actors
(including HWs) within the community and then used to
pursue their own interests (Baker 1990)
MethodsStudy design
This research is part of a multi-disciplinary investigation on the
acceptability and impact of male circumcision for HIV preven-
tion in PNG and used qualitative methods to explore HW
participation in unauthorized penile cutting practices in PNG
Unauthorized practices were defined as those activities that
were not considered a part of a HWrsquos expected role within the
health system or did not conform to standard treating practice
however involved the use of HWrsquos medical skills health system
4 HEALTH POLICY AND PLANNING
supplies or impacted on delivery of other services The quali-
tative research methods included in-depth interviews (IDIs)
with 25 frontline HWs involved in sexual and reproductive
health and data triangulation with findings from an additional
45 focus group discussions (FGDs) and 82 IDIs completed with
community members as part of a wider qualitative study on
community perceptions about masculinity and penile foreskin
cutting and penile modifications in PNG The fieldwork was
completed in five diverse social and geographical locations
around PNG including Central Province (CP) Eastern
Highlands Province (EHP) East Sepik Province (ESP)
Madang Province (MP) and West New Britain Province
(WNB) from 2009 until 2011 (Figure 1) Approval for the
research was obtained from research ethics committees at both
the PNG Institute of Medical Research (PNGIMR) and the
University of Queensland
Sampling and data collection for fieldwork
An iterative purposive sampling technique was used to identify
potential study participants following initial interviews with key
national and local stakeholders at each study location IDIs and
FGDs were completed with a variety of HWs from various
government and non-government health facilities around PNG
men who had undergone penile cutting inserts or associated
practices and other community leaders who had unique
insights and lived experiences in the study area Interview
guides were developed following extensive literature review and
discussions among the research team and followed a number of
themes including types of services provided and knowledge of
penile foreskin cutting in PNG Interviews were completed
by the in-country research team from the PNGIMR and a
researcher from the University of Queensland Interviews were
conducted in either English or PNG pidgin (the most widely
spoken of PNGrsquos three national languages) as per the partici-
pantrsquos preference digitally recorded transcribed verbatim and
translated into English
Data analysis
The framework analysis method appropriate for the analysis of
qualitative data for policy-oriented studies was used to analyse
the data (Braun and Clarke 2006) All IDIs and FGDs were
initially double coded by the in-country research team at the
PNGIMR In cases of discrepancy in coding a third researcher
coded the selected text in question Preliminary analysis of the
HW interviews showed the differing roles that HWs played in
penile cutting in PNG Themes were further updated as the
analysis developed and organized around identification of
whether respondents discussed unauthorized penile cutting
practices or services that operated outside the rules and
regulations of the health system and reasons for their
participation These themes were further triangulated with
IDIs and FGDs completed with community members to assist in
exploring the interconnections of the sociocultural context in
which the HW was participating Final codes were developed by
the first author and adjusted as required following review from
fellow authors
Figure 1 Map of PNG with study provinces highlighted
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 5
Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

supplies or impacted on delivery of other services The quali-
tative research methods included in-depth interviews (IDIs)
with 25 frontline HWs involved in sexual and reproductive
health and data triangulation with findings from an additional
45 focus group discussions (FGDs) and 82 IDIs completed with
community members as part of a wider qualitative study on
community perceptions about masculinity and penile foreskin
cutting and penile modifications in PNG The fieldwork was
completed in five diverse social and geographical locations
around PNG including Central Province (CP) Eastern
Highlands Province (EHP) East Sepik Province (ESP)
Madang Province (MP) and West New Britain Province
(WNB) from 2009 until 2011 (Figure 1) Approval for the
research was obtained from research ethics committees at both
the PNG Institute of Medical Research (PNGIMR) and the
University of Queensland
Sampling and data collection for fieldwork
An iterative purposive sampling technique was used to identify
potential study participants following initial interviews with key
national and local stakeholders at each study location IDIs and
FGDs were completed with a variety of HWs from various
government and non-government health facilities around PNG
men who had undergone penile cutting inserts or associated
practices and other community leaders who had unique
insights and lived experiences in the study area Interview
guides were developed following extensive literature review and
discussions among the research team and followed a number of
themes including types of services provided and knowledge of
penile foreskin cutting in PNG Interviews were completed
by the in-country research team from the PNGIMR and a
researcher from the University of Queensland Interviews were
conducted in either English or PNG pidgin (the most widely
spoken of PNGrsquos three national languages) as per the partici-
pantrsquos preference digitally recorded transcribed verbatim and
translated into English
Data analysis
The framework analysis method appropriate for the analysis of
qualitative data for policy-oriented studies was used to analyse
the data (Braun and Clarke 2006) All IDIs and FGDs were
initially double coded by the in-country research team at the
PNGIMR In cases of discrepancy in coding a third researcher
coded the selected text in question Preliminary analysis of the
HW interviews showed the differing roles that HWs played in
penile cutting in PNG Themes were further updated as the
analysis developed and organized around identification of
whether respondents discussed unauthorized penile cutting
practices or services that operated outside the rules and
regulations of the health system and reasons for their
participation These themes were further triangulated with
IDIs and FGDs completed with community members to assist in
exploring the interconnections of the sociocultural context in
which the HW was participating Final codes were developed by
the first author and adjusted as required following review from
fellow authors
Figure 1 Map of PNG with study provinces highlighted
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 5
Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

Results and DiscussionAnalysis of the data revealed a number of additional motivators
and obligations other than direct financial gain that prompted
the provision of unauthorized penile cutting These included a
change in social standing meeting of cultural obligations roles
within traditional economies and participating in traditional
roles as a dual practice In the sociocultural context of PNG
these unauthorized practices seem to arise from the need to
cope with the pressures of community expectations within a
failing health system and are not entirely about alleviating the
burden of unsatisfactory living and working conditions The
relationships gained or maintained by the HWs through
participating in unauthorized practices influence the social
standing of the HWs which is further amplified by percep-
tions from the community that HWs are technically safer
practitioners Their response to the social and cultural pressures
on them to engage in penile cutting does generate a lsquocurrencyrsquo
that provides a form of social investment and exchange for the
HW within their local sociocultural environment (Table 1)
How performance of foreskin cuts boosts HWs socialcurrency in PNG
The HW as a cultural lsquobrokerrsquo facilitating access to services
The role HWs played with connecting the community to the
health system was varied According to the respondents it was
quite common that knowing someone working within the
health service provided ease of access to health staff and
facilities for assistance with penile cutting
What they normally do ismdashthey come and see somebody
that they know in the hospital and then that fellow will
come around and inform us that these guys are coming for
or they want to do circumcision [Medical Officer WNB]
HWs suggested that the reasons the community members
approached them was because they were embarrassed or
concerned about the anticipated attitudes of other HWs
However indirect access to the health service also had the
potential to reduce the costs associated with transport and time
off work or even the reported waiting times if they went
through the usual formal channels One HW reported that he
had been waiting for over 6 months to get his son circumcised
at the provincial hospital Therefore accelerated access to
health services via complex kinship networks or wantoks
often free of formal charges has a significant worth
The HW as lsquobig manrsquo social recognition and prestige
The social recognition obtained in being able to assist commu-
nity members with penile cutting forms a source of significant
social capital for the HW in PNG where men can achieve
status fame and authority as lsquobig menrsquo (a title of status or
leader) through their actions (Bainton 2008) Access to unique
skills even where this did not result in higher wages provided
an opportunity to augment existing status within the commu-
nity HWs advised that based on their observation of what was
happening in their community they were aware that their skills
in penile foreskin cutting could be used to build their
reputation Their technical skills could be further developed
with experience and would then respond to a range of differing
requests from the community
Sometimes I do full removal Get rid of the skin and later
when there is only half of the skin I use to sew it suture
So there are two types I do for circumcision One is lsquoopen
cutrsquo (dorsal slit cut only) especially in their community
where it is their custom and the other is the lsquoround cutrsquo
(full circumcision) Because of my health worker training I
am able to apply the skills I know and perform what they
(the community) want [Community Health Worker WNB]
Possession of exclusive knowledge or recognition through skills
or position in a community has important implications for
many communities of PNG (de Renzio 2000 Bainton 2008)
The status of the lsquobig manrsquo in PNG is not gained through
acquisition of leadership roles in the community but rather the
outcome of a series of acts which elevate the person above
others as an acknowledged standing in interpersonal relations
(Sahlins 1963 de Renzio 2000) Individual status may be
distinguished according to professional standing income and
the subsequent capacity for conspicuous consumption resulting
in the power of influence in the community (Bainton 2008)
For the HW providing a special service for a community
member may assist in elevating their own community position
Likewise a HW providing a special service for a lsquobig manrsquo in the
community also involved an exchange of recognition
the big man for example radio announcer or bank
managers they come These big men when they come they
say lsquoyou touched my body (penis) so here is 50 kina for you
have some drinks (beer)rsquo Only those big men help us (give
us money) Not small boys not other men no only big man
like bank managers radio managers They say lsquowhen you
are finish you go and get a 6 pack and wash your handsrsquo
[Community Health Worker ESP]
The opportunity to elevate social standing was also evident in
communities which engaged in traditional penile cutting
activities In these communities there seemed to be a particular
impetus for HWs to perform penile cutting either due to
community expectation or the role the HW perceived they
played in the community In essence HWs in traditional cutting
communities were able to participate in distinct dual practices
in their community one as a HW and the other as a recognized
traditional penile cutting practitioner Dual practice in the
health sector has previously been described as HWs working
concurrently in the public and private sector to mitigate low
salaries and other unsatisfactory conditions (Ferrinho et al
2004b) In PNG dual practice may take the form of engaging in
work that is part of traditional culture with the use of public
system resources and may be seen as a potential opportunity to
elevate social standing or be a part of facilitating customary
practices in the community
The HW as a player benefits from local economies
HWs reported that the penile foreskin cutting services they
provide were typically on a voluntary basis for non-identified
medical reasons and conducted outside of usual work hours for
6 HEALTH POLICY AND PLANNING
no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

no arranged payment However distinction was made between
payment to the hospital or a wage to the HW and payment lsquoin
kindrsquo due to gratitude or for a assisting with a customary or
contemporary practice For customary penile cutting practices
this involved payment to the HW by customary means such as
shell money and lsquokaruka nutsrsquo (an edible nut popular and
widely available particularly in the highlands of PNG) which
have substantial value in traditional economies (Strathern
1993 Bainton 2008 Lederman 2009) or invitations to custom-
ary celebrations In other provinces it was common that offers
of fruit and other foodstuff were provided in appreciation of the
service Therefore although the participants reported that
money rarely changed hands and then only in gratitude for
services or with customary payments there was still an
economic benefit obtained through traditional economies but
this itself could produce unpredictable outcomes
The tradition of compensation in PNG may also extend to HWs
motivation to engage in unauthorized practices Compensation in
PNG is expected following many different kinds of loss
including death during clan fights or other accidents and there
is considerable pressure to pay to ensure further trouble and
bloodshed is prevented (Trompf 1994 Strathern and Stewart
2000) Various factors influence the amount of compensation
that needs to be paid including the nature of the event the
relationship of the parties involved and the economic or social
position of the guilty party (Trompf 1994 Goddard 1996
Strathern and Stewart 2000) HWs have also been implicated
in cultural compensation claims by providing services for a fee
where unexpected complications resulted from the service or
outcomes were considered unsatisfactory by the client (van
Amstela and van der Geest 2004) Obligation to participate in
unauthorized practices however may be driven by fear of
repercussions arising from perceived responsibilities from their
professional roles For example HWs not only feel pressure to
assist with dealing with complications sustained from a penile
cut completed by non-HWs but also risk sharing the blame for
negative outcomes Committing to undertake the procedure
themselves may seem to limit these risks
This fear may also impact on a HWs decision not to engage in
a service For example one HW was concerned about the
possibility of a national MC programme for HIV prevention for
fear that this would raise community expectations of complete
protection from HIV and could result in retribution in the event
of a circumcised man becoming HIV-positive
If our awareness [health promotion] goes wrong the
consequences will come back to us If circumcised men
are infected they will point their fingers to us the health
people and say lsquoYou said I will not get it and I went for
circumcision but now I got it and your words are liesrsquo They
will not believe us and this has its consequences too
[Health Extension Officer EHP]
The HW as ethical practitioner fulfilment of moral obligationand professional satisfaction
Justification for engaging in unauthorized penile cutting
practices according to most respondents was due to the
perceived failings of the health system to respond appropriately
to the potential complications following penile foreskin cutting
undertaken by non-HWs HWs saw their participation as a
necessary part of their responsibility of being a HW in PNG
Reasons for engagement in regular unauthorized practices
centred around a genuine concern that the men from the
community would perform the penile foreskin cut in precarious
ways regardless of whether they had HW support or not In
some cases HWs even reasoned that if they could not provide
the services themselves then supplying the equipment and
instructions for the desired penile foreskin cut would assist in
ensuring safety of the procedure
Many times they come and ask me for equipment And
many times I get cross at them and reject them I tell them
that they should come to me and I will do it But since
many will not come out like I said already they are very
young and are ashamed to come So when I recognize their
problem I now give them equipment and just advise them
how they should do it [Health Extension Officer EHP]
The sense of responsibility to compensate for the failings of the
health system combined with a deep sense of need for service
and religious conviction have been shown to be key motivators
of HWs engagement in health services in PNG (Jayasuriya et al
2011 Razee et al 2012 Tynan et al 2013) Participation in
unauthorized practices assists in satisfaction of moral respon-
sibility as a HW and committed religious practitioner as well as
general professional self-fulfilment
ConclusionsCoping mechanisms create an opportunity to extend the
boundaries of a health system at the discretion of the HW
(van Lerberghe et al 2002) In the case of PNG the emergence
of unauthorized practices as a coping mechanism is compelled
by mutual obligations where HWs are obliged to share
professional skills and access to resources as part of communal
social capital rather than engage in cash economies Likewise
HWs acquire social currency or resources and status which arise
from social networks and communities by providing preferen-
tial treatment and resources amongst these networks (Tynan
et al 2011) This has implications not only for quality control of
services conducted in informal environments and medico-legal
issues around accreditation but also for introduction of new
programmes that may overlap with the sociocultural environ-
ment such as male circumcision for HIV prevention
The introduction of new health programmes requires concerted
efforts from all sections of the health system However in the
case of fragile health systems opportunities are created for
unauthorized practices to become institutionalized pre-empting
appropriate policy development or regulation even before new
programmes are introduced If practices are already informally
established this creates difficulties in measuring the impact of
new intervention programmes because of misreporting or under-
reporting and delivery of services that do not conform to
standards If there is a male circumcision programme introduced
in PNG for HIV prevention the regulation of the dorsal foreskin
slit procedure within the health system will be imperative
Current research to determine whether dorsal slit procedures
offer any protective effect in terms of HIV acquisition will play a
significant role in determining what form of regulation would be
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 7
appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

appropriate There will also be significant tensions across cultural
domains arising from conflicts around preferred ways and
reasons for engaging in particular practices The coping strategies
adopted by the HWs for the provision of unauthorized penile
cutting practices in PNG end up undermining the existing system
because the provider creates their own working conditions and
income in the form of social and economic gains Yet the
relationships and systems that develop even if they have
negative consequences for the health system are the result of
HW desire and obligations to fulfil their full range of social
responsibilities and often are seen by them as consistent with
their professional roles Although some may draw parallels with
HWs continued engagement in female genital cutting in other
countries (Caldwell et al 2000 Shell-Duncan 2001
Christoffersen-Deb 2005) MCmdashand dorsal slit penile cuttingmdash
does not involve the same negative clinical social and cultural
consequences
In order to ensure the success of new programmes which
already have an established informal system it will be
important to acknowledge the existence of such practices and
ensure understandings of potential implications are included
within the programme design (Berman and Cuizon 2004
Jumpa et al 2007 Kiwanuka et al 2011) It has been argued
that even in an adverse socio-economic environment it is
feasible to create conditions that allow individual providersrsquo
strategies to remain compatible with equity and quality while
responding to their aspirations for survival social status and
professional satisfaction (Roenen et al 1997) Improvement of
working conditions in a place such as PNG however is more
than a combination of adequate salary and access to resources
(Segall 2000 van Lerberghe et al 2002) It also means
developing good supervision and support acknowledging the
complex role HWs play in their communities and harnessing
these conditions for positive outcomes Perhaps most import-
antly it requires a social environment that reinforces profes-
sional behaviour and boundaries and acknowledgement that
legislation and regulation are not enough This study used
penile cutting practices as a focus however it is likely that
reasons for engaging in coping mechanisms for other
unauthorized practices are likely to be similar in PNG What
is clear nonetheless is that HW management in PNG extends
beyond the boundaries of health organizations into the complex
sociocultural environment in which they work
AcknowledgementsThis study was supported by an Australian Agency for
International Development (AusAID) Australian Development
Research Award (ADRA) for the Male Circumcision
Acceptability and Impact Study PNG (MCAIS)
Conflict of interest statement None declared
ReferencesAshmore J 2013 lsquoGoing privatersquo a qualitative comparison of medical
specialistsrsquo job satisfaction in the public and private sectors of
South Africa Hum Resour Health 11 1
Auvert B Taljaard D Lagarde E et al 2005 Randomized controlled
intervention trial of male circumcision for reduction of HIV
infection risk the ANRS 1265 Trial PLoS Med 2 e298
Bailey R Moses S Parker C et al 2007 Male circumcision for HIV
prevention in young men in Kisumu Kenya a randomised
controlled trial Lancet 369 643ndash56
Bainton NA 2008 Men of Kastom and the customs of men status
legitimacy and persistent values in Lihir Papua New Guinea Aust J
Anthropol 19 194ndash212
Baker W 1990 Market networks and corporate behavior Am J Sociol 96
589ndash625
Berman P Cuizon D 2004 Multiple Public-private Jobholding of Health Care
Providers in Developing Countries An Exploration of Theory and Evidence
London DFID Health Systems Resource Centre
Braun V Clarke V 2006 Using thematic analysis in psychology Qual Res
Psychol 3 77ndash101
Brown JE Micheni KD Grant EM et al 2001 Varieties of male
circumcision a study from Kenya Sex Transm Dis 28 608ndash12
Caldwell JC Israel OO Caldwell P 2000 Female genital mutilation
conditions of decline Population Res Policy Rev 19 23ndash55
Chaudhury N Hammer J Kremer M Muralidharan K Rogers FH 2005
Missing in action teacher and health worker absence in developing
countries J Econ Persp 20 91ndash116
Chereches RM Ungureanu MI Sandu P Rus IA 2013 Defining
informal payments in healthcare a systematic review Health Policy
110 105ndash14
Christoffersen-Deb A 2005 lsquoTaming Traditionrsquo medicalized female
genital practices in Western Kenya Med Anthropol Quart 19 402ndash18
Conteh L Kingori P 2010 Per diems in Africa a counter-argument
Trop Med Int Health 15 1553ndash55
Dabalen A Wane W 2008 Informal payments and moonlighting in
Tajikistanrsquos health sector Policy Research Working Paper Series
Washington DC World Bank
Davy CP Patrickson M 2012 Implementation of evidence-based
healthcare in Papua New Guinea Int J Evid-Based Healthcare 10
361ndash68
de Renzio P 2000 Bigmen and Wantoks social capital and group
behaviour in Papua New Guinea QEH Working Paper Series -
QEHWPS27 27
Delcheva E Balabanova D Mckee M 1997 Under-the-counter pay-
ments for health care evidence from Bulgaria Health Policy 42
89ndash100
Doyle SM Kahn JG Hosang N Carroll PR 2010 The impact of male
circumcision on HIV transmission J Urol 183 21ndash26
Falkingham J 2004 Poverty out-of-pocket payments and access to
health care evidence from Tajikistan Soc Sci Med 58 247ndash58
Ferrinho P Omar M Fernandes M et al 2004a Pilfering for survival
how health workers use access to drugs as a coping strategy Hum
Resour Health 2 1ndash6
Ferrinho P van Lerberghe W Fronteira I Hipolitp F Biscaia A 2004b
Dual practice in the health sector review of the evidence Hum
Resour Health 2 1ndash17
Garcıa-Prado A Gonzalez P 2007 Policy and regulatory responses to
dual practice in the health sector Health Policy 84 142ndash52
Giedion U Morales LG Acosta OL 2001 The impact of health
reforms on irregularities in Bogota hospitals In Di Tella R
Savedoff WD (eds) Diagnosis Corruption Fraud in Latin Americarsquos
Public Hospitals Washington DC Inter-American Development
Bank pp 163ndash98
Goddard M 1996 The snake bone case law custom and justice in a
Papua New Guinea Village Court Oceania 67 50ndash63
8 HEALTH POLICY AND PLANNING
Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

Gonzalez P Macho-Stadler I 2013 A theoretical approach to dual
practice regulations in the health sector J Health Econ 32 66ndash87
Gray RH Kigozi G Serwadda D et al 2007 Male circumcision for HIV
prevention in men in Rakai Uganda a randomised trial Lancet
369 657ndash66
Hill P Tynan A Law G et al 2012 A typology of penile cutting in Papua
New Guinea results of a modified Delphi study among sexual
health specialists AIDS Care 24 77ndash86
Israr SM Razum O Ndiforchu V Martiny P 2000 Coping strategies of
health personnel during economic crisis A case study from
Cameroon Trop Med Int Health 5 288ndash92
Izard J Dugue M 2003 Moving Toward a Sector-wide Approach Papua New
Guinea the Health Sector Development Program Experience Manila
Asian Development Bank
Jan S Bian Y Jumpa M et al 2005 Dual job holding by public sector
health professionals in highly resource-constrained settings prob-
lem or solution Bull World Health Organ 83 771ndash76
Jayasuriya R Razee H Bretnall L et al 2011 Voices from the Field Factors
Influencing Rural Health Worker Performance in Papua New Guinea
Sydney Australia The University of New South Wales
Jumpa M Jan S Mills A 2007 The role of regulation in influencing
income-generating activities among public sector doctors in Peru
Hum Resour Health 5 5
Kelly A Kupul M Aeno H et al 2012a More than just a cut a
qualitative study of penile practices and their relationship to
masculinity sexuality and contagion and their implications for
HIV prevention in Papua New Guinea BMC Int Health Hum Rights
12 10
Kelly A Kupul M Fitzgerald L et al 2012b lsquoNow we are in a different
time various bad diseases have comersquo Understanding menrsquos
acceptability of male circumcision for HIV prevention in a
moderate prevalence setting BMC Public Health 12 1ndash13
Kempf W 2002 The politics of incorporation masculinity spatiality and
modernity among the Ngaing of Papua New Guinea Oceania 73
56ndash77
Kigozi G Wawer M Ssettuba A et al 2009 Foreskin surface area and
HIV acquisition in Rakai Uganda (size matters) AIDS 23 2209ndash13
Kiwanuka SN Rutebemberwa E Nalwadda C et al 2011 Interventions
to manage dual practice among health workers Cochrane Database
Syst Rev 7 1ndash22
Lederman R 2009 What Gifts Engender Social Relations and Politics in
Mendi Highland Papua New Guinea Cambridge Cambridge
University Press
Lindelow M Serneels P 2006 The performance of health workers
in Ethiopia results from qualitative research Soc Sci Med 62
2225ndash35
Liu T Sun M 2012 Informal payments in developing countriesrsquo public
health sectors Pacific Econ Rev 17 514ndash24
MacLaren D Tombe R Redman-MacLaren M et al 2011a A research
based classification of penile cutting in PNG a synthesis of
research findings from the ADRA and NHMRC studies Joint
National Policy Forum on Male Circumcision for HIV Prevention in Papua
New Guinea Port Morseby Papua New Guinea Institute of Medical
Research and James Cook University
MacLaren D Tombe R Redman-MacLaren M et al 2011 lsquoStronger or
tougherrsquo reasons for penile cutting in Papua New Guinea
Australasian HIVAIDS Conference Canberra Australasian Society
for HIV Medicine p 75
Macq J Ferrinho P De Brouwere V van Lerberghe W 2001 Managing
health services in developing countries between the ethics of the
civil servant and the need for moonlighting Hum Resour Health
Dev J 5 7ndash24
Manzi F Schellenberg J Hutton G et al 2012 Human resources for
health care delivery in Tanzania a multifaceted problem Hum
Resour Health 10 3
McCoombe SG Short RV 2006 Potential HIV-1 target cells in the
human penis AIDS 20 1491ndash5
McCoy D Bennett S Witter S et al 2008 Salaries and incomes of health
workers in sub-Saharan Africa The Lancet 371 675ndash81
McPake B Asiimwe D Mwesigye F et al 1999 Informal economic
activities of public health workers in Uganda implications for
quality and accessibility of care Soc Sci Med 49 849ndash65
McPake B Asiimwe D Mwesigye F Ofumbi M Streefland P Turinde A
2000 Coping strategies of health workers in Uganda Stud Health
Serv Organ Policy 16 157ndash62
Pask AJ McInnes KJ Webb DR Short R 2008 Topical oestrogen
keratinises the human foreskin and may help prevent HIV
infection PLoS ONE 3 1ndash4
Razee H Whittaker M Jayasuriya R Yap L Brentnall L 2012 Listening
to the rural health workers in Papua New Guineamdashthe social
factors that influence their motivation to work Soc Sci Med 75
828ndash35
Reilly B Phillpot R 2008 lsquoMaking democracy workrsquo in Papua New
Guinea social capital and provincial development in an ethnically
fragmented society Asian Survey 42 906ndash27
Roenen C Ferrinho P Van Dormael M Conceicao MC van
Lerberghe W 1997 How African doctors make ends meet an
exploration Trop Med Int Health 2 127ndash35
Sahlins MD 1963 Poor man rich man big-man chief Political types in
Melenesia and Polynesia Comp Stud Soc His 53 285ndash303
Schwalbach J Abdula M Adam Y Khan Z 2000 Good Samaritan or
exploiter of illness coping strategies of Mozambican health care
providers In Ferrinho P van Lerberghe V (eds) Studies in Health
Services Organisation amp Policy 16 117ndash30
Segall M 2000 From cooperation to competition in national health
systemsmdashand back impact on professional ethics and quality of
care Int J Health Plan Manage 15 61ndash79
Shell-Duncan B 2001 The medicalization of female lsquocircumcisionrsquo
harm reduction or promotion of a dangerous practice Soc Sci Med
52 1013ndash28
Siegfried N Muller M Deeks JJ Volmink J 2009 Male circumcision for
prevention of heterosexual acquisition of HIV in men Cochrane
Database Syst Rev 2 CD003362
Smith DJ 2003 Patronage per diems and the lsquoworkshop mentalityrsquo the
practice of family planning programs in Southeastern Nigeria
World Dev 31(4) 703ndash15
Strathern A 1993 Violence and political change in Papua New Guinea
Bijdragen tot de Taal- Land- en Volkenkunde 149 718ndash36
Strathern A Stewart PJ 2000 Accident agency and liability in New
Guinea Highlands compensation practices Bijdragen tot de Taal-
Land- en Volkenkunde 156 275ndash95
Tediosi F 2008 Access to medicines and out of pocket payments for
primary care evidence from family medicine users in rural
Tajikistan BMC Health Serv Res 8 109
Thomason J 2006 Health reform in Papua New Guinea and the Pacific
PNG Medical Journal 49 69ndash75
Tivinarlik A Wanat CL 2006 Leadership styles of New Ireland high
school administrators Anthropol Educ Quart 37 1ndash20
Trompf GW 1994 Payback The Logic of Retribution in Melanedian Societies
Cambridge
Tynan A Vallely A Kelly A et al 2011 Health workers health facilities
and penile cutting in Papua New Guinea implications for male
circumcision as an HIV prevention strategy PNG Med J 54 109ndash22
COPING MECHANISMS OF PAPUA NEW GUINEA HEALTH WORKERS 9
Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING

Tynan A Vallely A Kelly A et al 2012 Vasectomy as a proxy
extrapolating health system lessons to male circumcision as an
HIV prevention strategy in Papua New Guinea BMC Health Serv Res
12 299
Tynan A Vallely A Kelly A et al 2013 Socio-cultural and individual
determinants for motivation of sexual and reproductive health
workers in Papua New Guinea and their implications for male cir-
cumcision as an HIV prevention strategy Hum Resour Health 11 7
van Amstela H van der Geest S 2004 Doctors and retribution the
hospitalisation of compensation claims in the Highlands of Papua
New Guinea Soc Sci Med 59 2087ndash94
van Lerberghe W Conceic C Van Damme W Ferrinho P 2002 When
staff is underpaid dealing with the individual coping strategies of
health personnel Bull World Health Organ 80 581ndash84
Vian T Miller C Themba Z Bukuluki P 2011 Perceptions of per diems
in the health sector evidence and implications Boston University
U4 Anti-Corruption Resource Center 4
Vincent L 2008 lsquoBoys will be boysrsquo traditional Xhosa male circumci-
sion HIV and sexual socialisation in contemporary South Africa
Cult Health Sex 10 431ndash46
WHOUNAIDS 2007 Press Release WHO and UNAIDS announce
Recommendations from Expert Meeting on Male Circumcision for
HIV Prevention 28 March httpwwwwhointhivmediacentre
news68enindexhtml accessed 7 July 2013
Williamson MH 1990 Gender in the cosmos in Kwoma culture Sepik
Heritage Tradition and Change in Papua New Guinea Sydney
Crawford House Press
10 HEALTH POLICY AND PLANNING