AmbiHealth Medical Digest - Weebly
44
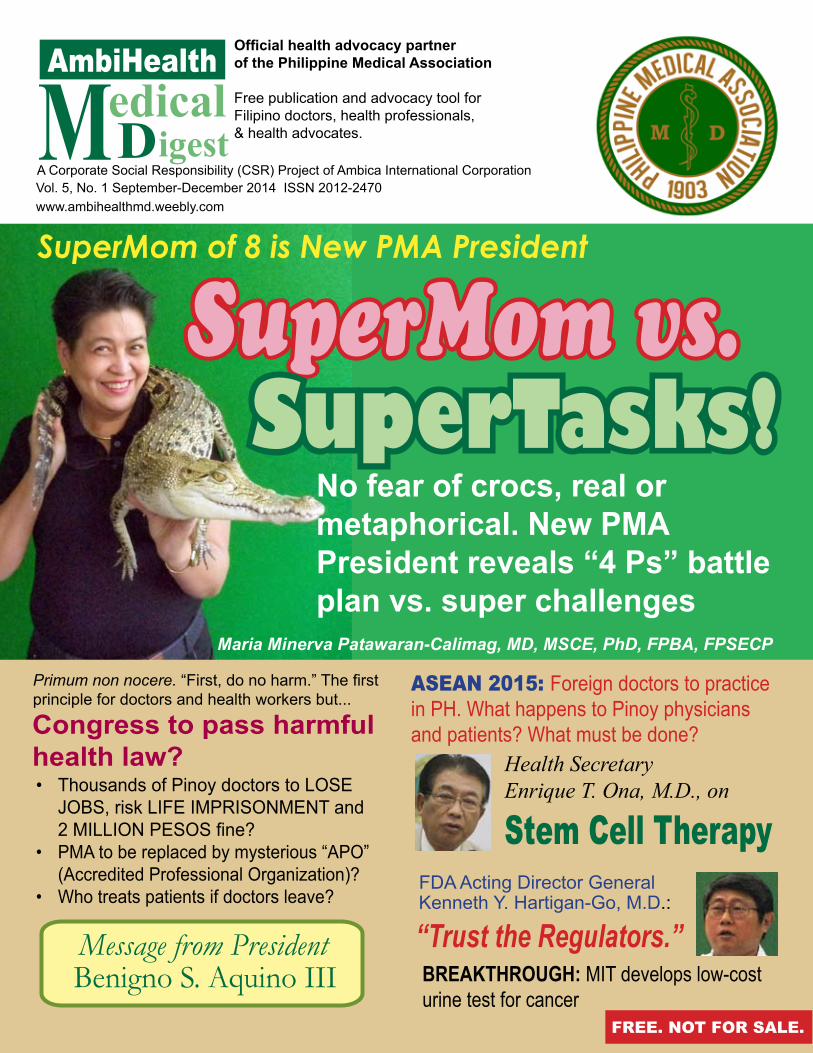
M edical D igest AmbiHealth Vol. 5, No. 1 September-December 2014 ISSN 2012-2470 A Corporate Social Responsibility (CSR) Project of Ambica International Corporation Official health advocacy partner of the Philippine Medical Association Free publication and advocacy tool for Filipino doctors, health professionals, & health advocates. www.ambihealthmd.weebly.com BREAKTHROUGH: MIT develops low-cost urine test for cancer ASEAN 2015: Foreign doctors to practice in PH. What happens to Pinoy physicians and patients? What must be done? Health Secretary Enrique T. Ona, M.D., on Stem Cell Therapy FDA Acting Director General Kenneth Y. Hartigan-Go, M.D.: “Trust the Regulators.” Primum non nocere. “First, do no harm.” The first principle for doctors and health workers but... Congress to pass harmful health law? Thousands of Pinoy doctors to LOSE • JOBS, risk LIFE IMPRISONMENT and 2 MILLION PESOS fine? PMA to be replaced by mysterious “APO” • (Accredited Professional Organization)? Who treats patients if doctors leave? • Message from President Benigno S. Aquino III SuperMom of 8 is New PMA President SuperMom vs. SuperTasks! No fear of crocs, real or metaphorical. New PMA President reveals “4 Ps” battle plan vs. super challenges Maria Minerva Patawaran-Calimag, MD, MSCE, PhD, FPBA, FPSECP FREE. NOT FOR SALE.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of AmbiHealth Medical Digest - Weebly
www.ambicaglobal.com | www.ambicare.net 1
Medical Digest
MedicalDigest
AmbiHealth
Vol. 5, No. 1 September-December 2014 ISSN 2012-2470 A Corporate Social Responsibility (CSR) Project of Ambica International Corporation
Official health advocacy partnerof the Philippine Medical Association
Free publication and advocacy tool forFilipino doctors, health professionals,& health advocates.
www.ambihealthmd.weebly.com
BREAKTHROUGH: MIT develops low-cost urine test for cancer
ASEAN 2015: Foreign doctors to practice in PH. What happens to Pinoy physicians and patients? What must be done?
Health Secretary Enrique T. Ona, M.D., on
Stem Cell TherapyFDA Acting Director GeneralKenneth Y. Hartigan-Go, M.D.:
“Trust the Regulators.”
Primum non nocere. “First, do no harm.” The first principle for doctors and health workers but...
Congress to pass harmful health law?
Thousands of Pinoy doctors to LOSE • JOBS, risk LIFE IMPRISONMENT and 2 MILLION PESOS fine?PMA to be replaced by mysterious “APO” • (Accredited Professional Organization)?Who treats patients if doctors leave?•
Message from President Benigno S. Aquino III
SuperMom of 8 is New PMA President
SuperMom vs.SuperTasks!
No fear of crocs, real or metaphorical. New PMA President reveals “4 Ps” battle plan vs. super challenges
Maria Minerva Patawaran-Calimag, MD, MSCE, PhD, FPBA, FPSECP
FREE. NOT FOR SALE.
www.ambihealthmd.weebly.com2
AmbiHealth M.D.
FOR INQUIRIES, please contact AMBICA INTERNATIONAL CORPORATION, #9 Amsterdam Extension, Merville Park Subdivision, Paranaque City, PHILIPPINES 1700Phones: (632) 828-6617 to 18; 828-6542Fax: (632) 828-6615Mobile: (0917)554-6073; (0917)839-7430e-mail: [email protected]: www.ambicaglobal.com
www.ambicaglobal.com | www.ambicare.net 3
Medical Digest
My warmest greetings to the Ambica In-ternational Corporation as you publish your AmbiHealth Medical Digest.
Our country’s sustained revitalization relies on the dynamic relations between the public and private sectors working towards a healthier, more empowered citizenry. Your organization counts among our steadfast allies in fulfilling this vital undertaking, as you help promote two of our major thrusts: Universal Health Care and Public-Private Partnerships. May the publication of this medical digest further engage your stakehold-ers and inspire them as they secure our people’s welfare through an im-proved health care industry.
Our respective endeavors are integral to our communal agenda of nation-building. Your government trusts that, with your support, and in partner-ship with other sectors, we will foster a culture of inquiry and innovation, rooted in the principles of integrity, accountability, and excellence.
Congratulations, and more power to all of you.
MESSAGE
MALACAÑAN PALACEMANILA
www.ambihealthmd.weebly.com4
AmbiHealth M.D.
AMBICA (pronounced as “am-BIH-kah”) is a Sanskrit name meaning “mother; good, compassionate woman or force that protects humanity against evil.” It is also one of the variant names of the god-dess Parvati.
With the mission to pro-vide affordable, effective, and safe medication for every Fili-pino, AMBICA International
Corporation is a pharmaceuti-cal (generics) company which specializes in Human Health-care.
AMBICA set out as a distribution company in 2000 and has grown steadily to emerge as a respected nationwide pharmaceutical marketing and distribution entity. AMBICA is the partner and representative of many foreign pharmaceu-tical manufacturing corporations that have strong and valued presence in the Philippine pharmaceutical industry.
In line with the company’s mission of cost-effective care to every Filipino, AMBICA has specialized divisions that ca-ter to different markets. AMBICA is focused on promoting results-oriented, researched and developed products. We are also committed in all respects to the highest levels of safety,
environmental awareness, and ethics. For us, the patient’s health always comes first. AMBICA provides not only medi-cines and services, but solutions for life.
The Wise Choice for Affordable Medications
AMBICA is a Filipino company, supplying niche prod-ucts to the entire Philippines. It has been in the pharmaceuti-cal market for more than a decade. It is now classified as one of the leading importers and distributors of world-class pharmaceutical products.
Since its establishment in 2000, AMBICA has commit-ted itself to provide the highest quality medicines to Filipino patients.
AMBICA employs professionals who combine skills and knowledge and work in harmony to achieve its goals. The company has paved the way for Filipinos to avail of world-class affordable medicines either for maintenance therapy or direct therapeutic regimen for diseases such as cancer, diabe-tes, hypertension, allergies, dyslipidemia, and many more.
We have made our mark in the industry through our un-wavering commitment to give only the best products and ser-vices that would benefit the majority. Because of your trust and confidence, AMBICA will continue to provide quality medicines within every Filipino’s reach.
www.ambicaglobal.com | www.ambicare.netAmbica International Corporation, No. 9 Amsterdam Extension, Merville Park Subdivision,
Paranaque City, Metro Manila, PHILIPPINESPhones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615
Mobile: (0917) 554-6073; (0917) 839-7430; e-mail: [email protected]
Dear Readers: AHMD welcomes your comments and suggestions. We also welcome (from doctors, medical societies, other health pro-fessionals, health advocates, and their organizations) health-related press statements / releases, literary pieces (poems and brief essays), photos, greetings, also jokes. Please send e-mail to: [email protected]; [email protected]
ADVERTISERS MOST WELCOME! Influential community leaders with high purchasing power -- such as doctors and other
health professionals -- are ideal target-markets for your products, services, and ideas (advocacies). Through them you can convince many others. Reach this select group nationwide (and worldwide via our website) through AmbiHealth Medical Digest (AHMD)!
RATES (all ads in full color): Back Cover (full page) - P70,000.00; Inside Front or Inside Back Cover (full page) - P60,000.00; INSIDE PAGES: Full Page - P50,000.00; Half Page - P25,000.00; 1/4 page - P13,000.00; 1/8 page - P7,000.00
Please contact AHMD at mobile (0916) 191-1967; telefax (02) 535-1403; phone (02) 425-5877; e-mail: [email protected]; [email protected]
AMBICA

www.ambicaglobal.com | www.ambicare.net 5
Medical Digest
Message from President Aquino ----- 3Cord Blood Banking --------------------- 5
Congress to pass harmful health law? ----------------- 6
SuperMom vs. SuperTasks (Interview with new PMA President Dr. Minerva Calimag) -------------- 10
DOH: Hospital Classification --------- 14List: New PMA officers (2014-15) -- 21MASEAN: Crucial Role in 2015? ---- 22FDA: Trust the Regulators ----------- 24
DOH gives free anti-pneumonia vaccine for children --------------------- 25DOH: TB still major problem ---------- 28 DOH: Malara elimination soon ------- 28
Liver Cancer Biomarker Tests: Best tool for early detection of liver cancer -------------------------- 29
CDO Surgeon-Photographer Victor Francis Orencia shares his art ------------------------ 30
Health Secretary Enrique T. Ona, M.D., speaks on STEM CELL THERAPY -------------- 32
MIT: A paper diagnostic for cancer ------------------------------- 38
Molecular Diagnostic Tests cut risk of wrong diagnosis; best early warning tool against diseases -------- 42
CONTENTS
In the past, the umbilical cord was merely discarded after birth, thus wasting precious life-giving stem cells.
Now, through ReliCord, the cord blood and cord tissue can be saved, frozen and stored for 21 years or more. The col-lection is a non-invasive process that is totally painless and harmless to the mother or the newborn infant.
ReliCord, the first registered cord blood bank and reposi-tory in Southeast Asia, is now available to Filipinos through the partnership of Ambica Biotechnologies and Reliance Life Sciences, one of the world’s largest biopharma corporations.
Using stem cells found in the baby’s cord blood, Cord Blood Banking makes it possible to protect not just the health of the baby but also that of the entire family -- parents, brothers, and sisters. The compatibility of the baby’s stem cells with all members of the immediate family is virtually assured.
Cord blood is the richest source of stem cells. Stem cells from cord blood and cord tissue are among the latest breakthroughs in medical science as protocol against more than EIGHTY (80) deadly diseases like cancer, blood disorders, tissue related disorders (heart, bone, spi-nal cord, liver, etc).
“We hope that in the near fu-ture, more and more expectant Filipino couples will gain access to the benefits of ReliCord Cord Blood/ Cord Tissue Banking Services. It offers immense peace of mind and highly reliable, possible protection against future diseases to the entire family,” says Ambica executive Job Joseph. “We encourage everyone, especially expectant Filipino couples, to learn more about the latest lifesaving technology. For inquiries, they can reach me at mobile 0917-548-3611; e-mail: [email protected]; phones 828-6617 to 18. They can also visit our website (www.ambicaglobal.com).”
Ambica Biotechnology and ReliCord
Cord Blood BankingThe lifesaver “bank saving” for your entire fam-
ily -- and all the deposits come from the young-est member, your newborn baby!
AmbiHealth M.D. Medical Digest www.ambihealthmd.weebly.com
EDITORIAL OFFICE:Mobile (0916) 191-1967Telefax: (02) 535-1403; Phone: (02) 425-5877E-mail: [email protected]@gmail.com PUBLISHER’S OFFICE:AMBICA INTERNATIONAL CORPORATIONNo. 9 Amsterdam Extension, Merville Park
Subdivision, Paranaque City, Metro Manila, PHILIPPINESPhones: (632) 828-6617 to 18; 828-6542 Fax: (632) 828-6615; Mobile: (0917) 554-6073(0917) 839-7430e-mail: [email protected]: www.ambicaglobal.com PUBLISHERKamal Abichandani
EDITORIAL CONSULTANTSDeepu BhatiaJob Joseph
MANAGING EDITORRaymond Lim Toledo
ASSOCIATE EDITORHaydee Parras
LAYOUT EDITORRaymond Lim Toledo
ARTIST: Nestor BacosWRITERS/RESEARCHERSSimon Ortiz, Charito TubianoACCOUNT EXECUTIVECarol Tingson
ADVOCACY CONSULTANTFountainhead Consulting
www.ambihealthmd.weebly.com6
AmbiHealth M.D.
.
The document speaks for itself. In law, documentary evidence is best
because it brooks no alibi. A bounced check is it. A signed contract is so.
Here, the documents are from the cur-rent 16th Congress (2013-2016): House Bill 1775 by Representative Abigail Binay and Senate Bill 1294 by Senator Jinggoy Estrada (interestingly, both legislators have a physician-mother).
Same title: “Physicians Act of 2013” (PA 2013).
Same refiled versions of the “Physi-cians Act of 2012,” filed during the previ-ous 15th Congress.
Both documents/bills speak for them-selves. Same content. Crystal-clear provi-sions which include, among many others, life imprisonment and two million pesos fine for non-specialists who do specialist work.
Well-milledDisturbing that PA 2013 is not new. Not
just the brainchild of its present sponsors. If it were, it could be dismissed as PR ploy by headline-hungry legislators, not to be taken seriously.
Unfortunately, not the case here. Rather, it has already gone through
the legislative mill of several congress-es. PA 2013 is an exact replica of a bill unanimously approved on 3rd Reading by several congresses. In effect, both bills embody the collective “wisdom” and deliberation of Congress. Which makes it all the more disturbing, even frightening.
Will it pass? The signs are ominous.To recall, the House of Representa-
tives (HOR) under the 15th Congress (June 26, 2010 – June 30, 2013) unani-mously passed (not a single objec-tion!) on Third Reading the Physicians Act of 2012 (House Bill 6538), suppos-edly to amend the antiquated Medical Act of 1959 (Republic Act 2382).
At the Senate, the main proponents then of a virtually identical version (Senate Bill 3137) were Senators Franklin Drilon and Antonio Trillanes IV.
Only the interruption caused by the May 2013 elections stopped the bill from becoming a law signed by the President.
Many reelected Considering that many HOR members
of the 15th Congress got reelected to the 16th Congress, observers noted, at the start of the 16th Congress, that there was a great probability that they would refile HB 6538 and, this time, make sure it becomes law. After all, they already approved on 3rd Reading – unanimously and enthusiasti-
Physicians Act of 2013Primum non nocere. “First, do no harm.” The first principle for doctors and health workers but...
Thousands of Pinoy non-specialist doctors to lose jobs, risk life imprisonment and 2 million pesos fine?PMA to be replaced by mysterious “APO” (Accredited Professional Organization)?If non-specialists leave PH or stop practicing, what happens to millions of poor Filipino patients who can’t afford specialists?
Congress to passharmful health law?
by Raymond Lim Toledo
cally – the same bill during the 15th Congress.
Bill refiledAnd they have lost no
time.Last July 24, 2013, just two
days after the 16th Congress opened, Makati Representa-tive Mar-Len Abigail S. Binay filed House Bill 1775 at the House of Representatives.
On August 15, 2013, Senator Jinggoy Ejercito Estrada filed Senate Bill 1294 at the Philippine Senate.
In her EXPLANATORY NOTE (page 1) for HB 1775, Rep. Binay emphasizes: “… this bill was already approved on third and final reading during the 12th, 13th, 14th, and 15th Congresses. However, lack of material time prevented the Senate from approving a counterpart measure, thus pav-ing the way for the necessary bicameral conference committee report and its pro-posed enactment into law. This bill is al-ready a product of extensive debates and vital amendments, both in the committee and plenary levels. Speedy approval of this bill is therefore in order.”
Senate President in favor?Incumbent Senate President Frank-
lin Drilon was the principal author of the Physicians Act of 2012 during the 15th Congress. Most likely, therefore, he will be fully supportive of the 2013 version which is virtually an exact copy of his 2012 bill.
The Senate President is the most pow-erful man in the Senate and the third most powerful official in government, next only to the Vice President. Any bill he supports will most likely pass the Senate. Therefore, unless by a great miracle his opinion has been totally reversed, then most likely the Senate will pass the Physicians Act of 2013 during the 16th Congress.
Faster approvalThis time, most likely the bill will be
processed faster since most members of the 16th Congress finished reviewing and de-bating the bill during the 15th Congress.
Executive branch support?The appointment by President Beni-
gno S. Aquino III of one of the principal authors and most vocal proponents of the Physicians Act of 2012, former Rep. Ja-nette Garin, M.D., to be an Undersecretary of the Department of Health, indicates the
great possibility of strong support from the Executive Branch for the bill’s passage into law.
Health Undersecretary Dr. Garin is said to be quite influential with the President. If she convinces the President to certify the bill as urgent, then the saying “tapos na ang boksing” (the boxing bout is over) could well apply.
It should be noted that Dr. Garin’s hus-band, Engr. Oscar Garin, Jr., now occupies her seat in Congress (HOR), after winning in the May 2013 election. It would not be surprising if he supports the bill champi-oned by his wife during the 15th Congress.
Frightening implicationsWhat are the implications if the 16th
Congress passes the Physicians Act of 2013 – and the President signs it into law – as is, without amendments?
One major implication is that if a non-specialist does specialist work on a patient – and the pa-tient dies -- the non-specialist will be punished with life imprison-ment and two million pesos fine (as per Item 10-b, Section 38 of HB 1775; Item 10-b, Section 39 of SB 1294). Of course, along with said penalties, the non-specialist also loses his medical license.
While the lay public’s knee-jerk reac-tion would likely be “So what? Such a doc-tor deserves life imprisonment anyway… after all, the patient died…” – the consid-erations and consequences in real life are not that simple.
The disturbing – and frightening – im-plications of this scenario can be gleaned from our interview with Dr. Minerva Cal-imag, President of the Philippine Medical Association (PMA) (please see next ar-ticle for interview); as well as from other Filipino doctors who expressed their views
but requested that their names be withheld.
In sum, the various doctors we interviewed make the following points:
Over the decades, because of the absence of any law prohibiting “non-specialists” from doing “specialist” work, as well as the acute short-
age of doctors to serve a hundred-million Filipinos, we now have thousands of gen-eral practitioner / “non-specialist” Filipino doctors doing “specialist” work, serving millions of Filipino patients, most of them poor.
Most of these “non-specialist” doc-tors have undergone specialist training but have not yet taken or passed the certifying exam. While said doctors are not officially certified specialists, years or even decades of actual practice have made them highly competent in the “specialist” work they do.
Our sources in the medical community say that approximately 50% of actively practicing doctors in the Philippines are non-specialists.
Estimates on the total number of ac-tively practicing doctors range from a very optimistic high of 75,000 to the more real-istic low of 27,000 (the latter based on the number of PMA members in “active/good standing,” i.e., members who have paid their P1,200.00 annual membership dues and have completed 300 units of Continu-ing Medical Education (CME) per year).
Since it is more logical and realistic to assume that most actively practicing doc-tors are also active PMA members, then most likely, if allowance is given for a mi-nority of practicing doctors who are not ac-tive in PMA, the total number of practicing doctors is just a little above 27,000; say 40,000.
The World Health Organization (WHO) pegs the ideal ratio at 1 doctor per 600 population. Considering that as of early 2014, the Philippines has a total population of 100 million, having 40,000 practicing doctors implies a doctor-patient ratio of only 1 doctor for every 2,500 Fili-pinos – or more than 300% below the 1:600 ratio prescribed by WHO.
Now imagine a scenario wherein, if the Physicians Act of 2013 becomes law (with-out major amendments), majority or all of the 50% of non-specialists decide to stop

www.ambicaglobal.com | www.ambicare.net 7
Medical Digest
.
The document speaks for itself. In law, documentary evidence is best
because it brooks no alibi. A bounced check is it. A signed contract is so.
Here, the documents are from the cur-rent 16th Congress (2013-2016): House Bill 1775 by Representative Abigail Binay and Senate Bill 1294 by Senator Jinggoy Estrada (interestingly, both legislators have a physician-mother).
Same title: “Physicians Act of 2013” (PA 2013).
Same refiled versions of the “Physi-cians Act of 2012,” filed during the previ-ous 15th Congress.
Both documents/bills speak for them-selves. Same content. Crystal-clear provi-sions which include, among many others, life imprisonment and two million pesos fine for non-specialists who do specialist work.
Well-milledDisturbing that PA 2013 is not new. Not
just the brainchild of its present sponsors. If it were, it could be dismissed as PR ploy by headline-hungry legislators, not to be taken seriously.
Unfortunately, not the case here. Rather, it has already gone through
the legislative mill of several congress-es. PA 2013 is an exact replica of a bill unanimously approved on 3rd Reading by several congresses. In effect, both bills embody the collective “wisdom” and deliberation of Congress. Which makes it all the more disturbing, even frightening.
Will it pass? The signs are ominous.To recall, the House of Representa-
tives (HOR) under the 15th Congress (June 26, 2010 – June 30, 2013) unani-mously passed (not a single objec-tion!) on Third Reading the Physicians Act of 2012 (House Bill 6538), suppos-edly to amend the antiquated Medical Act of 1959 (Republic Act 2382).
At the Senate, the main proponents then of a virtually identical version (Senate Bill 3137) were Senators Franklin Drilon and Antonio Trillanes IV.
Only the interruption caused by the May 2013 elections stopped the bill from becoming a law signed by the President.
Many reelected Considering that many HOR members
of the 15th Congress got reelected to the 16th Congress, observers noted, at the start of the 16th Congress, that there was a great probability that they would refile HB 6538 and, this time, make sure it becomes law. After all, they already approved on 3rd Reading – unanimously and enthusiasti-
Physicians Act of 2013Primum non nocere. “First, do no harm.” The first principle for doctors and health workers but...
Thousands of Pinoy non-specialist doctors to lose jobs, risk life imprisonment and 2 million pesos fine?PMA to be replaced by mysterious “APO” (Accredited Professional Organization)?If non-specialists leave PH or stop practicing, what happens to millions of poor Filipino patients who can’t afford specialists?
Congress to passharmful health law?
by Raymond Lim Toledo
cally – the same bill during the 15th Congress.
Bill refiledAnd they have lost no
time.Last July 24, 2013, just two
days after the 16th Congress opened, Makati Representa-tive Mar-Len Abigail S. Binay filed House Bill 1775 at the House of Representatives.
On August 15, 2013, Senator Jinggoy Ejercito Estrada filed Senate Bill 1294 at the Philippine Senate.
In her EXPLANATORY NOTE (page 1) for HB 1775, Rep. Binay emphasizes: “… this bill was already approved on third and final reading during the 12th, 13th, 14th, and 15th Congresses. However, lack of material time prevented the Senate from approving a counterpart measure, thus pav-ing the way for the necessary bicameral conference committee report and its pro-posed enactment into law. This bill is al-ready a product of extensive debates and vital amendments, both in the committee and plenary levels. Speedy approval of this bill is therefore in order.”
Senate President in favor?Incumbent Senate President Frank-
lin Drilon was the principal author of the Physicians Act of 2012 during the 15th Congress. Most likely, therefore, he will be fully supportive of the 2013 version which is virtually an exact copy of his 2012 bill.
The Senate President is the most pow-erful man in the Senate and the third most powerful official in government, next only to the Vice President. Any bill he supports will most likely pass the Senate. Therefore, unless by a great miracle his opinion has been totally reversed, then most likely the Senate will pass the Physicians Act of 2013 during the 16th Congress.
Faster approvalThis time, most likely the bill will be
processed faster since most members of the 16th Congress finished reviewing and de-bating the bill during the 15th Congress.
Executive branch support?The appointment by President Beni-
gno S. Aquino III of one of the principal authors and most vocal proponents of the Physicians Act of 2012, former Rep. Ja-nette Garin, M.D., to be an Undersecretary of the Department of Health, indicates the
great possibility of strong support from the Executive Branch for the bill’s passage into law.
Health Undersecretary Dr. Garin is said to be quite influential with the President. If she convinces the President to certify the bill as urgent, then the saying “tapos na ang boksing” (the boxing bout is over) could well apply.
It should be noted that Dr. Garin’s hus-band, Engr. Oscar Garin, Jr., now occupies her seat in Congress (HOR), after winning in the May 2013 election. It would not be surprising if he supports the bill champi-oned by his wife during the 15th Congress.
Frightening implicationsWhat are the implications if the 16th
Congress passes the Physicians Act of 2013 – and the President signs it into law – as is, without amendments?
One major implication is that if a non-specialist does specialist work on a patient – and the pa-tient dies -- the non-specialist will be punished with life imprison-ment and two million pesos fine (as per Item 10-b, Section 38 of HB 1775; Item 10-b, Section 39 of SB 1294). Of course, along with said penalties, the non-specialist also loses his medical license.
While the lay public’s knee-jerk reac-tion would likely be “So what? Such a doc-tor deserves life imprisonment anyway… after all, the patient died…” – the consid-erations and consequences in real life are not that simple.
The disturbing – and frightening – im-plications of this scenario can be gleaned from our interview with Dr. Minerva Cal-imag, President of the Philippine Medical Association (PMA) (please see next ar-ticle for interview); as well as from other Filipino doctors who expressed their views
but requested that their names be withheld.
In sum, the various doctors we interviewed make the following points:
Over the decades, because of the absence of any law prohibiting “non-specialists” from doing “specialist” work, as well as the acute short-
age of doctors to serve a hundred-million Filipinos, we now have thousands of gen-eral practitioner / “non-specialist” Filipino doctors doing “specialist” work, serving millions of Filipino patients, most of them poor.
Most of these “non-specialist” doc-tors have undergone specialist training but have not yet taken or passed the certifying exam. While said doctors are not officially certified specialists, years or even decades of actual practice have made them highly competent in the “specialist” work they do.
Our sources in the medical community say that approximately 50% of actively practicing doctors in the Philippines are non-specialists.
Estimates on the total number of ac-tively practicing doctors range from a very optimistic high of 75,000 to the more real-istic low of 27,000 (the latter based on the number of PMA members in “active/good standing,” i.e., members who have paid their P1,200.00 annual membership dues and have completed 300 units of Continu-ing Medical Education (CME) per year).
Since it is more logical and realistic to assume that most actively practicing doc-tors are also active PMA members, then most likely, if allowance is given for a mi-nority of practicing doctors who are not ac-tive in PMA, the total number of practicing doctors is just a little above 27,000; say 40,000.
The World Health Organization (WHO) pegs the ideal ratio at 1 doctor per 600 population. Considering that as of early 2014, the Philippines has a total population of 100 million, having 40,000 practicing doctors implies a doctor-patient ratio of only 1 doctor for every 2,500 Fili-pinos – or more than 300% below the 1:600 ratio prescribed by WHO.
Now imagine a scenario wherein, if the Physicians Act of 2013 becomes law (with-out major amendments), majority or all of the 50% of non-specialists decide to stop

www.ambihealthmd.weebly.com8
AmbiHealth M.D.
accepting any patient who might require a specialist for fear of life imprisonment and a P2 million fine. After all, no doctor, not even specialists, can give 100% assurance that the patient will not die while undergo-ing treatment.
This means that the acute shortage of doctors will become even more acute: there will be only 1 doctor for every 5,000 Filipi-nos (instead of 1:2,500).
What happens to the millions of poor, pregnant, Filipino wom-en who can’t find or can’t afford a certified specialist (obstetrician/ gynecologist) when it’s time to de-liver their babies?
Assuming there’s a doctor/general prac-titioner available who is more than capable of delivering the baby safely, can we blame him if he refuses to do so because, after all, in case the mother or her baby dies due to numerous possible complications while giving birth, he will be punished with life imprisonment and a P2 million fine, plus loss of medical license?
What happens to children whose poor parents can’t find or can’t afford certified specialists (pediatricians) to check and treat their children?
What happens to patients in urgent need of a simple surgical procedure when only doctors with diplomates in surgery will be legally allowed to operate?
What happens to burn victims from a
fire who can’t find or can’t afford certified specialists (dermatologists) to treat their burnt skins?
And so on and so forth, millions of sim-ilar situations in the lives of 100 million Filipinos, most of whom are poor and can-not find or cannot afford a specialist when they most need one.
And, by the way, what hap-pens to the 50% non-specialist Filipino doctors (around 20,000) who will inevitably soon find themselves with no medical field to safely practice in? What hap-pens to their families when they stop earning?
After all, if you think about it, every medical case can be easily interpreted to require a specialist (even a sub-specialist, who is more specialized than the special-ist!), especially if something goes terribly wrong during treatment and the patient’s relatives look for someone to blame and sue.
For example, one of the simplest pro-cedures for any doctor is delivering ba-bies. But if something goes wrong during delivery, if the mother or baby dies, then it would be so easy to blame and sue the general practitioner/non-specialist for do-ing “specialist” (obstetrician/gynecologist) work.
How can a general practitioner do his
work calmly and confidently if he/she is al-ways afraid that if something goes wrong, he could easily be charged with wrongfully doing “specialist” work and thus suffer life imprisonment and P2 million fine?
Another by-the-way: Who will now want to become a doctor?
Who will now want to go through TEN YEARS of mind-breaking, budget-busting study – not to mention passing the Medi-cal Board Exam -- to become a “Doctor of Medicine,” only to be subjected to such a frightening and irrational law?
And what happens to the Philippine health system when it becomes very dif-ficult to attract young Filipinos to become doctors?
What happens to the much-publicized “Universal Health Care” Vision / Program of the Aquino Administration when we run out of enough doctors for 100 million Filipinos?
Another critical implication – if the Physicians Act of 2013 gets passed into law without amendments – is that the 110 years old Philippine Medical Association (PMA) (older than DOH or PRC), for some “mysterious” reason, faces the very real risk of being abolished / replaced by another (still unidentified) “Accredited Professional Organization.”
PMA objects strongly to this vague APO provision. It wants Congress to amend this provision and make PMA the automatic APO -- similar to the prevail-ing (albeit largely outdated) Medical Act of 1959, Republic Act 2382, wherein PMA is explicity mentioned as member of the Board of Medical Education.
So will Congress pass the the Physi-cians Act of 2013 without the needed amendments?
Truth is it depends on us, the Fipino voters. If we allow apathy to rule us, if Fili-pino doctors, health workers, and patients fail to unite and lobby soon enough for a sane and HEALTHY health law, chances are one morning we will all wake up to PA 2013 passed by both House and Senate, ap-proved and signed into law by the Presi-dent. We will have no one left to blame then but ourselves.
Anxious patients (mostly charity cases) lining up for consultation at a clinic in Cagayan de Oro City. PHOTO BY DR. VICTOR FRANCIS ORENCIA
FOR INQUIRIES, please contact AMBICA INTERNATIONAL CORPORATION, #9 Amsterdam Extension, Merville Park Subdivision, Paranaque City, PHILIPPINES 1700; Phones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615; Mobile: (0917)554-6073; (0917)839-7430; e-mail: [email protected]: www.ambicaglobal.com
www.ambicaglobal.com | www.ambicare.net 9
Medical Digest
accepting any patient who might require a specialist for fear of life imprisonment and a P2 million fine. After all, no doctor, not even specialists, can give 100% assurance that the patient will not die while undergo-ing treatment.
This means that the acute shortage of doctors will become even more acute: there will be only 1 doctor for every 5,000 Filipi-nos (instead of 1:2,500).
What happens to the millions of poor, pregnant, Filipino wom-en who can’t find or can’t afford a certified specialist (obstetrician/ gynecologist) when it’s time to de-liver their babies?
Assuming there’s a doctor/general prac-titioner available who is more than capable of delivering the baby safely, can we blame him if he refuses to do so because, after all, in case the mother or her baby dies due to numerous possible complications while giving birth, he will be punished with life imprisonment and a P2 million fine, plus loss of medical license?
What happens to children whose poor parents can’t find or can’t afford certified specialists (pediatricians) to check and treat their children?
What happens to patients in urgent need of a simple surgical procedure when only doctors with diplomates in surgery will be legally allowed to operate?
What happens to burn victims from a
fire who can’t find or can’t afford certified specialists (dermatologists) to treat their burnt skins?
And so on and so forth, millions of sim-ilar situations in the lives of 100 million Filipinos, most of whom are poor and can-not find or cannot afford a specialist when they most need one.
And, by the way, what hap-pens to the 50% non-specialist Filipino doctors (around 20,000) who will inevitably soon find themselves with no medical field to safely practice in? What hap-pens to their families when they stop earning?
After all, if you think about it, every medical case can be easily interpreted to require a specialist (even a sub-specialist, who is more specialized than the special-ist!), especially if something goes terribly wrong during treatment and the patient’s relatives look for someone to blame and sue.
For example, one of the simplest pro-cedures for any doctor is delivering ba-bies. But if something goes wrong during delivery, if the mother or baby dies, then it would be so easy to blame and sue the general practitioner/non-specialist for do-ing “specialist” (obstetrician/gynecologist) work.
How can a general practitioner do his
work calmly and confidently if he/she is al-ways afraid that if something goes wrong, he could easily be charged with wrongfully doing “specialist” work and thus suffer life imprisonment and P2 million fine?
Another by-the-way: Who will now want to become a doctor?
Who will now want to go through TEN YEARS of mind-breaking, budget-busting study – not to mention passing the Medi-cal Board Exam -- to become a “Doctor of Medicine,” only to be subjected to such a frightening and irrational law?
And what happens to the Philippine health system when it becomes very dif-ficult to attract young Filipinos to become doctors?
What happens to the much-publicized “Universal Health Care” Vision / Program of the Aquino Administration when we run out of enough doctors for 100 million Filipinos?
Another critical implication – if the Physicians Act of 2013 gets passed into law without amendments – is that the 110 years old Philippine Medical Association (PMA) (older than DOH or PRC), for some “mysterious” reason, faces the very real risk of being abolished / replaced by another (still unidentified) “Accredited Professional Organization.”
PMA objects strongly to this vague APO provision. It wants Congress to amend this provision and make PMA the automatic APO -- similar to the prevail-ing (albeit largely outdated) Medical Act of 1959, Republic Act 2382, wherein PMA is explicity mentioned as member of the Board of Medical Education.
So will Congress pass the the Physi-cians Act of 2013 without the needed amendments?
Truth is it depends on us, the Fipino voters. If we allow apathy to rule us, if Fili-pino doctors, health workers, and patients fail to unite and lobby soon enough for a sane and HEALTHY health law, chances are one morning we will all wake up to PA 2013 passed by both House and Senate, ap-proved and signed into law by the Presi-dent. We will have no one left to blame then but ourselves.
Anxious patients (mostly charity cases) lining up for consultation at a clinic in Cagayan de Oro City. PHOTO BY DR. VICTOR FRANCIS ORENCIA
FOR INQUIRIES, please contact AMBICA INTERNATIONAL CORPORATION, #9 Amsterdam Extension, Merville Park Subdivision, Paranaque City, PHILIPPINES 1700; Phones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615; Mobile: (0917)554-6073; (0917)839-7430; e-mail: [email protected]: www.ambicaglobal.com

www.ambihealthmd.weebly.com10
AmbiHealth M.D.
by Raymond Lim Toledo
New PMA President Maria Minerva Patawaran-Calimag, MD, MSCE, PhD, FPBA, FPSECP
SuperMom vs.SuperTasks!
She’s a Doctor of Medicine (Anesthesiologist) and a Doctor of Education with a long string of credentials and awards -- and a mother of EIGHT children, four of whom are already doctors of medicine, and another four who will soon be (the youngest is a high school senior).
Not only is she a mother. She was widowed in 2009 and, since then, has been both mother and father to her brood of eight. Her late husband was Dr. Placido “Jun” Calimag, Jr., a plastic reconstructive surgeon.
So, yes, especially for those who have actually expe-rienced what it means to be a father or mother, the mind-blowing daily challenges (financial, physical, mental, emo-tional, spiritual) one must surmount to sucessfully raise and educate even just one child (let alone eight!), it is but fit-ting to bestow the “SuperMom/SuperWoman” tag on Ma-ria Minerva Patawaran-Calimag, MD, MSCE, PhD, FPBA, FPSECP, new President of the Philippine Medical Associa-tion (PMA) (June 2014 – May 2015).
However, it looks like she will need every bit of her Su-perMom powers as she leads PMA against formidable Su-perTasks, such as:
u ASEAN 2015. The challenge: Considering that 2015 is just a few months away, how to deal with two related prob-lems: First, the likely deluge of thousands of foreign doc-tors from other ASEAN countries who will try to expand their practice to the Philippines; Second, the possible “brain drain” as Filipino doctors leave the Philippines to take advantage of more lucrative opportunities in other ASEAN nations.
This will happen because as signatory to the “ASEAN Community 2015” agreement, the Philippine government will have to lift restrictions on the flow of people, products, and services from and to its fellow ASEAN countries.
NOTE: The Association of Southeast Asian Nations
www.ambicaglobal.com | www.ambicare.net 11
Medical Digest
(ASEAN) is composed of 10 nations: Philippines, Indonesia, Malaysia, Singapore, Thailand, Brunei, Burma (Myanmar), Cambodia, Laos, and Vietnam.
According to en.wikipedia.org, “ASEAN covers a land area of 4.46 million km², which is 3% of the total land area of Earth, and has a population of approximately 600 million people, which is 8.8% of the world’s population. The sea area of ASEAN is about three times larger than its land counterpart. In 2012, its combined nominal GDP had grown to more than US$ 2.3 trillion. If ASEAN were a single entity, it would rank as the eighth largest economy in the world.”
u Physicians Act of 2013. The challenge: How to inject sense into an allegedly deadly health law Congress wants to pass.
For some mysterious reason, Congress has been doggedly trying, for more than 12 years (since the 12th Congress up to the present 16th Con-gress), to foist this law on the medical profession.
There are well-founded worries that this time, Congress could succeed.
If the bill gets passed into law without the right amendments, it could threaten thousands of Filipino doctors with unemployment, life imprisonment, P2 million fine, plus many other penalties – and greatly worsen the acute shortage of doctors for millions of poor Filipino patients. (Please see article on p. 6)
u Integration of PMA. According to Dr. Calimag herself, out of 72,000 Filipino doctors practicing in the Philippines, only 27,000 are active PMA mem-bers, i.e., members who have paid their P1,200.00 annual membership dues and have completed 300 units of Continuing Medical Education (CME) per year. The challenge: How to successfully push for the passage of a law for an Integrated PMA, simi-lar to the Integrated Bar of the Philippines (IBP), which makes it mandatory for any lawyer to be an IBP member of good standing before he can prac-tice law. Likewise, an Integrated PMA will pave the way for the unification of all Filipino doctors practicing in the Philippines, as PMA member-ship becomes mandatory instead of optional.
In the following interview conducted shortly before her official inauguration as PMA President for 2014-2015, she tells us a bit about herself and provides a comprehensive overview of her “battle plan” to win over the awesome challenges her new administration must face.
PROFILEMaria Minerva P. Calimag, M.D., M.S.C.E.,
Ph.D., F.P.B.A., F.P.S.E.C.P.
I• n 2012, the Professional Regulation Commission (PRC) awarded Dr. Calimag with the MOST OUT-STANDING PROFESSIONAL FOR MEDICINE and the FIRST ERIC NUBLA AWARD AS MOST OUT-STANDING PROFESSIONAL for 2012 wherein she bested 39 other outstanding professionals (from vari-ous PRC-licensed fields) in a three tiered selection pro-cess that had three Justices of the Court of Appeals as members of the Board of Judges. FULL PROFESSOR of Pharmacology, Anesthesiol-• ogy and Clinical Epidemiology at the UST Faculty of Medicine and Surgery PROFESSORIAL LECTURER, Epidemiology and • Medical Informatics at the UST Graduate SchoolPRESIDENT, Philippine Medical Association, 2014-• 20152-term GOVERNOR FOR MANILA of the Philippine • Medical Association (2004 and 2013)2-term PRESIDENT, Manila Medical Society (MMS) • 2002-20042-term PRESIDENT, Society for Obstetric Anesthesia • of the Philippines (SOAP) 2000-20022-term PRESIDENT, International College of Sur-• geons Alliance (ICSA) 2001-2003FELLOW and VICE-CHAIR, Board of Examiners, • Philippine Board of Anesthesiology (PBA) 2002-2007COMMISSIONER, Commission on Accreditation, • Philippine Board of Anesthesiology (PBA) 2014-20162-term PRESIDENT, Philippine Society of Anesthesi-• ologists, Inc. (PSA), 2010-2011SECRETARY of the Confederation of the ASEAN • Societies of Anesthesiologists 2008-2010PRESIDENT-ELECT of the Asian and Oceanic • Society for Regional Anesthesia and Pain Medicine 2013-2015.Born and reared in Manila, Dr. Calimag graduated • with honors during her primary education from the Dominican School (1969) and her secondary educa-tion from the UST High School (1973); the UST Col-lege of Science with a B.S. (Pre-Med) Magna Cum Laude (1977); the UST Faculty of Medicine and Sur-gery Benemeritus (1981); the University of the Philip-pines College of Medicine with a Masters of Science in Clinical Epidemiology (2003) under a scholarship grant from the Philippine Council for Health Research and Development. A firm believer in life-long learning and as further testimony of her passion for her craft, she successfully defended her dissertation (Meritis-simus) toward a Doctorate of Philosophy in Education major in Educational Management degree Summa Cum Laude (2011) at the UST Graduate School.
www.ambihealthmd.weebly.com12
AmbiHealth M.D.
AmbiHealth Medical Digest (AHMD): Before talking about the urgent issues your new PMA adminis-tration must face, please tell us about yourself... you are married, with chil-dren?...
Dr. Minerva Patawaran-Calimag (DMPC): I’m a widow. My husband, a plastic reconstructive surgeon, actually a trained microsurgeon, died in 2009, during Typhoon Ondoy (September 24-26, 2009)... he had a heart attack... he was the one in charge of medical mis-sions at the PMA... so Ondoy was re-ally painful for me because I lost my husband... yes, he died in the line of duty ... maybe he got too stressed... the medical missions then were national in scope because of the magnitude of On-doy’s devastation... he died a week af-ter Ondoy... on the day he died, he had just come back from teaching...that was the first school day after Ondoy...
AHMD: How many children do you have?
DMPC: We have eight children... barkada ko sila (they’re my buddies)... the oldest is 29 years old... I have four physicians na actually...
AHMD: Wow, ma’am, you are like a superwoman...
DMPC: I’m really a supermom... I am... I’m the supermom of PMA (laughs)...
AHMD: How many girls, how many boys?
DMPC: Three girls and five boys. Four of them are now physicians. I have a 3rd year surgical resident, one 1st year plastic, two interns... one in-coming 3rd year medical student, and the youngest is incoming 4th year high school...
AHMD: And then you’re going to be President of PMA...
DMPC: That’s where they grew up (in PMA). Can you imagine, this child was campaigning for me when she was still small, “Vote for my Mom!”
AHMD: How do you juggle all these things?
DMPC: You know, you don’t need to teach the children. They emulate their parents. They look up to you... oh, Daddy’s like this, Mommy’s like this... they just follow your footsteps... it’s all
a matter of time management. Many say, ah, doctora, you’re
busy? I’m not busy -- I am very busy! (laughs)
As I often say, there’s no fixed or absolute reality (everything is percep-tion and relative). My reality is I am able to do all of these things. Prioritiza-tion is part of everything. When I know I can do it, I can do it.
You see, the important thing in a person’s life is self-mastery. You do not become stressed because you know you can do it.
The first deterrent is when you say you can’t do it. When your mind says you can’t do it, then there’s noth-ing you can do. But when you have self-mastery, when you know what’s needed and you know how to do it, then you can do it.
And one thing I have set for my-self which my children emulate is that when you start something, you should finish it. You shouldn’t start one thing here and later start another thing there without finishing anything...
AHMD: Now to the urgent issues facing the medical profession... What
is PMA’s position regarding the Physicians Act of 2013 (PA 2013)?
DMPC: The provision on criminalization of medi-cal malpractice should be re-moved. PMA totally opposes criminalization because if it’s proven that a doctor has com-mitted malpractice, or he did not follow guidelines -- which can be easily seen -- he is already li-able under the penal code.
That’s just like our opposi-tion to a similar medical mal-practice bill in the past...
The important thing, I think, that we should look into, is cre-dentialling to define scope of practice.
Also, our stand is to put PMA as APO (Accredited Professional Organization) in the law (PA 2013). It should be written in the law... we are aware of the view of the other
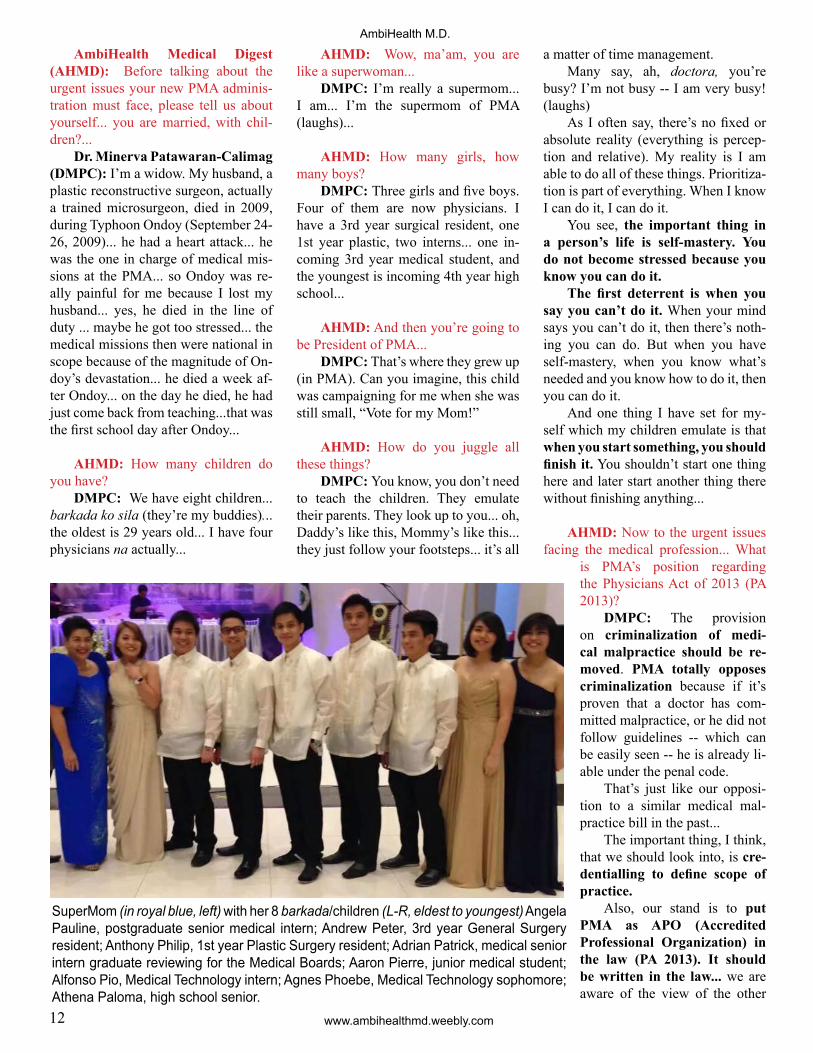
SuperMom (in royal blue, left) with her 8 barkada/children (L-R, eldest to youngest) Angela Pauline, postgraduate senior medical intern; Andrew Peter, 3rd year General Surgery resident; Anthony Philip, 1st year Plastic Surgery resident; Adrian Patrick, medical senior intern graduate reviewing for the Medical Boards; Aaron Pierre, junior medical student; Alfonso Pio, Medical Technology intern; Agnes Phoebe, Medical Technology sophomore; Athena Paloma, high school senior.
www.ambicaglobal.com | www.ambicare.net 13
Medical Digestside that the law should be generic (i.e., no mention of particular organization)... but what we are saying is that since the PMA has been there for one-hundred-eleven years, older even than DOH (Department of Health), PMA should be recognized as the APO.
AHMD: PA 2013 penalizes non-specialists who do specialist work with life imprisonment and P2 million fine. If implemented, what will be the impli-cations, especially on the poor?
DMC: They will be deprived (of health services). For example, appen-dectomies... and I’m just a poor per-son... I could say I want to have my operation here at this Level 2 hospital... anyway, this is good enough for me, I’m just here in the province, and my surgeon might have been trained, might not have the necessary board certifica-tion, and yet he has been doing it for a long time -- and so he should not be penalized for doing that...
The prevailing definition of a spe-cialist is someone who has passed board certification -- fellow or diplo-mate... Most doctors have completed their residency training but are unable to pass the specialty board exams... so we have to rethink or we have to look back at our specialty board exams as well... are we being too strict?
So we have included in our plans credentialling to define scope of prac-tice... this means even if you’re not a specialist, if you are able to do certain procedures, you can do those proce-dures but limited let’s say to a Level 2 hospital (EDITOR’S NOTE: Please see sidebar article on page 14 re hospital classification).
The point is those who have cre-dentialling for up to Level 2 will not be allowed to work at Level 3. But those with credentialling for up to Level 3 hospitals can also work at Level 2 or Level 1... however, one problem is there are specialists who work at Level 2 hospitals who don’t get reimbursed (by PhilHealth) because the procedures they do supposedly should get done only in Level 3 hospitals. But then pa-tients go to Level 2 because they can’t afford Level 3...
So it’s a matter really of harmoniz-ing the patients’ needs with the services that the doctors can offer...
AHMD: Do you agree with those who raise the scenario that if the PA 2013 bill gets passed into law without amendments, many non-specialists will stop working, out of fear that they will be penalized for doing “specialist work” even for simple procedures like delivering babies or appendectomies?
DMC: That’s why it (PA 2013) shouldn’t be passed into law. It won’t work because it’s not reality.
We should look at the practice of medicine in the context of the Phil-ippine scenario... that’s why we are pushing for credentialling to define the scope of practice... all doctors and other health workers should know when it’s time to refer.
Many problems are due to fail-ure to refer cases at the proper time... for example, a midwife who insists on handling the delivery of a baby even though, because of certain complica-tions, a specialist (obstetrician) is al-ready needed...
AHMD: Isn’t that difficult to ex-ecute? How do you implement that na-tionwide?
DMPC: It really needs widespread information dissemination... that’s why we need to do strategic planning, be-cause strategic planning will reveal the need for Continuing Medical Educa-tion (CME), not only for doctors, but also for peripherals like midwives who are doing care for the underprivi-leged in underserved areas.
AHMD: What will be your major programs? How will PMA members benefit?
DMPC: The main reason I ran (for PMA President) was to promote sincer-ity, integrity, transparency, and account-ability as things we should put a PMA leader to task.
I think these are questions we should really ask of our leaders -- like how do you manage our conflicts of in-terests in ethical issues that we are often faced with especially in the practice of
our profession... I’ve been with the PMA for the past
30 years. I started with PMA as soon as I took my oath in 1982...
What we want is for PMA to be more relevant. Many doctors have shied away from PMA because they don’t feel it’s relevant to their practice. Why? Because we have the specialty societies which are already addressing issues relevant to the practice of that profession. So if you are an anesthesi-ologist, you have the Philippine Soci-ety of Anesthesiologists (PSA). That’s where we discuss all the knowledge we need for the practice of anaesthesia. So where does that leave PMA? It’s sup-posed to be the umbrella organization and as such it ought to look into the problems of the physicians. Not only of the specialists but of the non-specialists as well. So what then should be the rel-evant stance of the PMA President and the PMA Board of Governors?... What should be the primary focus of PMA?
The problem is we have no strate-gic planning... we have no direction... Special events move PMA... so the board meeting is regular... every second Sunday of the month... and then comes the Medicine Week in September... and then last day of payment... and so on and so forth... it seems events are always the trigger for activities... and most of the time we are reactive... when BIR issues a statement, we react...
We are proactive, though, in the sense that we do lobby for laws... We have been lobbying for the Medical Act since 2003... at that time there was a move to have a medical malpractice bill; we opposed it because we feel there’s nothing intentional if something untoward happens to a patient; it’s not just the doctor’s fault.
There are instances as well when patients withhold information because they want to be operated on... And we must be very vigilant about those things... sometimes, for example, the patient already knows she has a thyroid condition... she will hide it from us, she will transfer to another hospital if you refuse to operate on her... so it’s dan-gerous if you don’t detect that she’s just shopping for a hospital that will operate

www.ambihealthmd.weebly.com14
AmbiHealth M.D.on her despite her thyroid condition...
AHMD: What is the logic there? Why does the patient want to be operated on and why does the doctor refuse?
DMC: In some cases, the doctor does not want to operate because the pa-tient does not need the operation... there are irrational patients like that who insist on unnecessary operations...
AHMD: What can PMA members expect from your new administration? What will be your major programs?
DMPC: We want to look at advoca-cies to drive changes at the PMA because otherwise, it will become events-driven again... just doing things repetitive-ly... everybody looking forward to the Medicine Week so we can take photos (laughs)... I call it advocacy for the “4 Ps” -- Profession, Physician-Peers, Pa-tients, and Planet...
On advocacy for Physician-Peers, we want to have something about good citizenship... such as the promise made by BIR to us when we met with them to develop an accounting software, for doctors, for tax payments... we will make the website of the PMA truly in-teractive, where we will deliver many of the things we need, such as BIR’s requirements from doctors or from self-employed. At the moment, when you visit the BIR website, there’s a lot of data not directly relevant of doctors... so we want to distill only the information that’s necessary for doctors... hopefully, tax payments and filing of tax returns can also be done online... in my view, if we minimize the people in between, the hu-man interface, we will be able to lessen corruption...
AHMD: How about the matter of making the charity work (free medical service to poor patients) of doctors tax-deductible?
DMPC: We raised that with BIR Commissioner Kim Henares but she asked us, where will BIR get the money to give you tax rebate when, in the first place, you have not paid any taxes for the free services you rendered?
AHMD: Well, one possibility is to
DOH: Hospital Classification
Under the Department of Health’s (DOH) Administrative Order 2012-0012, signed last July 18, 2012, a health facility must have, among others, an operating room to be considered a Level 1 hospital. The AO conforms to the mandate of Republic Act No. 4226, the Hospital Licensure Act, which requires a hospital to have surgical and ancillary services for its operation to be permitted.
The previous DOH guidelines did not require Level 1 hospitals to have an operating room and those health facilities with functioning operating rooms were considered Level 2 hospitals. Health facilities previously classified as Level 1
hospitals without operating rooms will now be considered as primary care facilities.
As of 2011, there were 733 government and 1,088 private hospitals, with 372 government and 399 private Level 1 hospi-tals under the old classification.
According to Health Sec-retary Enrique Ona, M.D., “With the new classification of hospi-tals and other health facilities, we are ensuring that all our hos-pitals have the minimum capac-ity to render emergency surgical care, such as cesarean sections and appendectomies.”
AO 2012-0012 classifies hospitals in the Philippines based on ownership (govern-ment or private), scope of ser-vices (general or specialized), and functional capacity (level 1, 2 or 3).
Among others, a Level 1 hospital must have an operat-ing room to be able to provide surgical services. A Level 2 hos-pital has all of Level 1 capacity and must be departmentalized, equipped to be able to provide services in the specialties of medicine, surgery, pediatrics and obstetrics-gynecology and has an intensive care unit. A Level 3 hospital has all of Level 2 capacity plus a residency or
teaching program. Ona also said that the DOH’s Health Facilities Enhancement Program will
upgrade government district hospitals without operating rooms for these facilities to be able to comply with the new guidelines. As of March 2012, an estimated 137 out of 283 district hospitals classified as Level 1 hospitals in the previous system have no operating rooms. For 2013, P 2.3 billion will be used to upgrade these district hospitals.
“Patients needing surgical care who are brought to some of our district hos-pitals often have to be referred to provincial or regional hospitals. With our new guidelines and with the upgrading of our district hospitals under the health fa-cilities enhancement program, our patients are assured of timely surgical care,” Ona concluded.
Source: www.doh.gov.ph
Photo courtesy of Dr. Betha Fe Castillo, President, Pangasinan Medical Society (PMS); Dr. Ma. Julita Parras-De Venecia, Secretary, PMS

www.ambicaglobal.com | www.ambicare.net 15
Medical Digest
monetize (give a peso value) char-ity work, ask the patient to sign an ac-knowledgment receipt for free medical services received, and then have the option to deduct the peso value of said charity service from the doctor’s tax li-abilities...
DMPC: That’s a possibility we can explore... I myself would like that since I do so many free medical missions... for example, we had one medical mis-sion wherein we did 80 operations per day, so in four days we did 320 opera-tions, all for free... imagine that, all in the name of service... however, on the other hand, I think what we earn from charity work is God’s grace... when you get money in exchange for charity work, you will lose the blessings... you say you are helping the poor but then you ask for tax credit -- you will lose your blessings (laughs)... but really, the truth is when we doctors go on medical missions, we really have at the back of our minds that we are doing it because we need to serve the less fortunate, not because we want to earn tax credits... but of course, a tax credit will not hurt (laughs)...
TelemedicineI also have a Ph.D. in Education,
major in Educational Management. My main focus in Education is Ed-
ucational Media and Technology... so that is what I want to bring to PMA... increase the use of technology for edu-cation among doctors... podcast (files which can be downloaded from web-sites and can be used offline), webcast (online Internet streaming), things like that... for example, not all doctors get to attend conventions... some are left to take care of the workplace. We want to address that situation.
We also want to harness telemedi-cine... if I have a physician in the prov-ince and we have a telemedicine facility there... it’s so easy now... just go online -- “Doctor, what should I do with this patient?” -- even if you’re working pro bono here in Manila... “Oh, don’t do that, that’s anesthesia, that’s dan-gerous...”... It’s not just the telephone now... you can ask for the X-ray to be sent to you online so you can review
it...
AHMD: Please tell us more about your plans to elevate the status of PMA…
DMPC: Our Vision is for Filipino physicians to be globally competitive but locally relevant.
We need to elevate the status of the PMA to a level of professional-ism beyond politics. Politics muddle all our issues at the PMA...we should all rise above politics and discuss the things that really matter to us as phy-sicians.
The leader must be respected and in turn be respectful of others...one with the wisdom and the ability to synthesize all inputs to a solution that will be beneficial for all. The medical profession is beset by many issues and challenges that it cannot tackle alone.
An integrated PMAThere is strength in numbers and
the PMA will work for the passage of a de-criminalized Medical Act that will push the integration of the PMA and promote inclusiveness of all physi-cians. PMA has to show the community at large that it is large enough to lobby and negotiate fairly on all issues that affect the medical community.
Credentialing to define scope of practice
Many of the legal issues brought to the attention of the PMA involve physicians who perform procedures beyond their credentialed status and levels of competency. There is a need therefore to define the scope of practice of the physician based on one’s level of training, board certification and board accreditation. A referral system for ser-vice upgrades shall be implemented and a tiered reimbursement scheme will be proposed considering that some physi-cians are dependent only on third-party payors and insurance reimbursements for their income.
A physician in every city, municipality and town
For our country, the PMA will as-sist medically (neglected) areas by im-proving the manpower distribution of physicians across the country and de-velop policy towards better health care access for patients and better working environments for physicians.
Every physician empowered to lead
We value creativity, responsible risk-taking, and enthusiastic pursuit of new ideas through creative governance. There are many changes that need to be
Mother with sick child in a municipal hospital.

www.ambihealthmd.weebly.com16
AmbiHealth M.D.
done at the PMA and the stra-tegic solutions shall be accom-plished at the appropriate time. Every physician will be engaged and every voice will be heard in meaningful conversations that affect our profession.
Strong collaborative partnerships
Strong collaborative part-nerships need to be forged to make sustainable change hap-pen. We value partnerships with business, industry, government, educational systems, and our Component Society communi-ties. Soon, the problems of the PMA will not just be local and we need to address global chal-lenges as well. The PMA needs a leader who will be the voice of the Filipino physicians. The PMA needs a leader who can talk and speak sensibly about all the issues that beleaguer our Profes-sion.
A globally-relevant PMAThe ASEAN Harmonization is
looming in the horizon. It is time to en-gage the global medical community on issues pertaining to the establishment of the global medical information high-way on issues of cross-country creden-tialing, pharmacovigilance issues on ground and across our borders, medical professionalism and many more. There is palpable yearning among us Filipino physicians for a leader who can stand head to head with otherleaders in the medical field and in government.
Uplift PMA imageWe will seek to uplift the image of
PMA through creative governance.This means applying “Transforma-
tive Servant Leadership” at PMA guid-ed by the principle of Filipino physi-cians valuing responsible, accountable, ethical behavior in an atmosphere of honest, open communication, and mu-tual respect.
There can be no substitute for prin-cipled leadership at the PMA.Under our PMA Constitution, the By-Laws is the law and not just guidelines.
So it is all the more important that the Officers and the PMA Board of Governors, through its appropriat-ing power, and the General Assem-bly, through its ratifying power, reject agreements whose long-range effects and impact on the PMAis unclear or potentially detrimental.
Leadership DevelopmentThe PMA will equip members to
become more influential in motivating and inspiring other physicians to be leaders in their communities. There is a need to enhance physicians’ lifelong learning and core aptitudes to excel as leaders within organized medicine, hospitals, health care systems, medi-cal staffs, group practices, and in the public policy arena. Leadership skills that need to be improved on includes, among others: self-awareness and self-assertiveness in leadership positions; building professional relationships among and between physician-hospital, physician-physician, and physician-pa-tient; conflict resolution during intense situations; advocacy to drive change; and effective collaboration in teams.
National and Component Society Officers must undergo the PMA Lead-ership Seminar and conduct their stra-tegic planning before assuming office in June.
System Process Improvement at all levels in the PMA
For the PMA as an orga-nization, we must systematize processes and protect what-ever resources we have. We will operationalize information management through data min-ing and processing of relevant digital information; dissemi-nate credible and truthful infor-mation at all levels within the PMA; systematically manage processes and improve work-flows at the PMA; and institute tighter internal and external control and management of our fiscal resources and transform our accounts receivables to positive cash flows.
Advocacy to drive changes at PMA
We aim to balance Change with Stability at PMA.
Our Mission is for Filipino physi-cians to work together to make a dif-ference in the lives of others through creative strategies enabled by wisdom and purpose.
The PMA is our Mother Organiza-tion since 1903 built upon the age-old ideals of our predecessors. It is the Accredited Professional Organization (APO) of physicians in the country for the longest time. It has weathered many challenges through the years. Advocacy will drive changes at the PMA. Mem-bers and patients count on the PMA to be the informed, authoritative and in-dependent voice in the art and science of medicine. Public confidence in our objectivity is critical to carrying out our mission. The public relies on the PMA to minimize actual and perceived conflicts of interest and ensure that all its interactions meet high ethical stan-dards. In all of these interactions, the PMA must be committed to acting with integrity and transparency.
Advocacy for the Profession
Legislative advocacyIncrease PMA participation on na-
tional issues that affect physicians and increase PMA physician involvement in the crafting of health policies.
Nurse explains doctor’s prescription to a farmer-patient in a rural hospital.

www.ambicaglobal.com | www.ambicare.net 17
Medical DigestThe top priorities involve legisla-
tive advocacy on behalf of physicians to receive respected, effective repre-sentation before national and local government on issues that directly af-fect physician practices and create a position of strength for physicians as decisions are made.
Provide weekly status updates during legislative sessions and on pro-posed bills including the Medical Act, the uninsured and managed care issues with PHILHEALTH and AHMOPI, and DOH, FDA, DDB and PDEA mandates affecting member practice.
The PMA will maintain a careful watch of all regulatory bodies including the Professional Regulation Commis-sion and challenge any efforts that would negatively affect the Filipino physicians, their practice and their patients.
Advocacy for Physician-PeersImprove the relevance of the PMA
to the individual members. Advocacy on behalf of physicians
is the principal task of the PMA and to advance the interests of physicians and their patients, to lobby for legisla-tion favorable to physicians and patients should be given priority.
The PMA shall continuously im-prove its membership benefit packages and make them responsive to every phy-sician’s needs, and the PMA shall sup-port member rights at all times.
The PMA will be the resource for general legal issues, policy, medical eth-ics and legislative updates
Member ParticipationEvery member shall take part in the
democratic forum of the PMA through the General Assembly wherein physi-cians raise and debate issues, formulate policy, and influence changes to im-prove patient care and the medical pro-fession. Increase member involvement and participation in the electoral process to help elect candidates who fairly rep-resent issues important to our medical community.
Membership FeedbackIt is vital to ensure that the PMA
continues to serve physician members
effectively. There is a need to assess PMA
members’ satisfaction with services of-fered by the Association: to ascertain members’ perceptions of the most im-portant issues for the PMA to address; obtain members’ assessments of the PMA performance in these areas and its responsiveness to their concerns; and assess overall levels of satisfaction with membership at the PMA and their likeli-hood of membership renewal.
Physician Mentoring The PMA is the lead organization in
providing physician education. For our individual members, the
PMA will increase opportunities for improving the credentialed status of physicians through alternative and tech-nology-enabled modes of Continuing Medical Education.
A Mentoring Program will also be instituted to provide knowledge and skill support prior to taking the creden-tialing/Specialty Board Exam.
Access to InformationThe PMA website will be the PMA’s
window and link to the global communi-ty and will feature the latest health care news and extensive information that is vital to medical practices relevant to the Filipino physician, such as develop-ments in new models of care especially for disease prevalent in the Philippines, and many more.
Monthly newsletters will be emailed directly to members to keep them in-formed of important breaking medical news, and legislative and compliance issues.
Evidence-based answers to practice questions can be availed through a PMA CME Resource Center.
Advocacy for PatientsEmphasis on health, wellness and
disease preventionPMA should also strive to help pa-
tients live longer and healthier lives through improved access to reliable medical information; increase the amount of physician time invested in wellness and prevention, and lobby for legislation that promote health, well-
ness and disease prevention. Start them young and teach children health promo-tion while still in elementary.
Patient safety initiativesPatient safety initiatives will be en-
hanced through inter-professional edu-cation and collaborative practice. Partner programs will be carried with alliances, organizations, specialties and profes-sions with similar advocacies on patient safety and quality care of patients.
Advocacy for Our PlanetWe will promote environmental ad-
vocacies. I have been an environmental health
advocate since my early leadership days at the Manila Medical Society, at the In-ternational College of Surgeons Alliance and the Philippine Society of Anesthesi-ologists...promoting tree planting, gar-bage segregation and recycling, energy saving techniques and reduction in the use of paper in many transactions. The advocacies shall continue at the PMA.
AHMD: What reforms do you in-tend to do to promote greater transpar-ency and accountability in PMA?
DMPC: There are many calls to strengthen the ethics of the profession... there are many instances when the Doc-tor’s Code of Ethics is not being fol-lowed... managing conflicts of inter-est...
AHMD: Quite a number of doctors say they don’t know what the PMA na-tional leadership / office is doing...
DMPC: Correct, correct. Detached sila. But when there’s a problem, they ask what is PMA doing? So our next ques-

www.ambihealthmd.weebly.com18
AmbiHealth M.D.tion is, did you vote in the PMA election? Have you paid your membership dues? You were not able to vote because you haven’t paid... good citizenship first! So it’s a matter of the chicken and the egg... so first, we need to instill in them love for PMA. How do we instill that? We have to restore their trust in the PMA leadership. Once we restore their trust, we will be able to address all the professional problems of doctors.
AHMD: How do you re-store their trust?
DMC: What’s needed are open lines of communica-tions with all areas -- Congress, the lawmaking body; PRC, the credentialling body; BIR, PhilHealth...
AHMD: Can extremely underpaid government doctors (also members of PMA), espe-cially those in rural areas who earn as low as P20,000.00 per month, expect your incoming administration to strongly lobby for an increase of their salaries?
DMPC: We will push for the full implementation of the Magna Carta for Health Workers... Since health de-livery has been devolved, we need to talk to provincial governors
AHMD: There is growing clamor for public health care to be restored to control by the National Government, particularly the Department of Health, instead of the present setup wherein health care is devolved to Local Govern-ment Units (LGUs). The clamor is based on the view that LGUs do not have the competence to handle health care. Will PMA under your administration sup-port this move to restore health care to DOH?
DMPC: It’s because LGUs have dif-ferent agendas. So if your LGU does not include or prioritize health in its agenda, then health will be at the bottom. There are certain areas where this is really the case...
My position is that for as long as DOH can handle all these health needs, then restore health care to DOH... the problem is the politics behind... are the LGUs willing to give up control of health delivery?
This is a political issue. We need to change the law. We need to change the Local Government Code... I think DOH is already moving towards amending the law to restore health delivery to the na-tional government. Yes, of course, PMA will support this move...
AHMD: How true are reports that certain unscrupulous LGU officials are pocketing the PhilHealth fees of LGU physicians?
DMPC: I prefer to approach this problem by establishing lines of com-munication with LGU officials... As a teacher, I inform minds and I form minds... I prefer a more positive ap-proach instead of making accusations... once we establish lines of communica-
tion and ask the LGU officials how to address problems re-garding the PhilHealth fees of LGU doctors, we might get bet-ter results.
AHMD: What are the oth-er urgent problems of the Phil-ippine health system?
DMPC: We need to make some changes in the curricu-lum of Philippine medical education. As I have stated in various fora, our curriculum is too focused on the science of medicine, there is no uniform implementation of the medical curriculum all over the coun-try; there are some medical curriculum which strongly ad-dress public health -- which is correct, especially in the prov-inces... the expectation there is their graduates will practice in the province.
AHMD: So what are these changes you want to see?
DMPC: There should be socio-anthropology... this re-fers to the cultural aspects of medicine... the people’s health
beliefs... we need to teach this to medi-cal students, not just medicine... be-cause it explains why some patients refuse to take the medicines their doc-tors prescribe.... And the reason is be-cause of their culture, their beliefs... then there are the realities of technology, e-health is coming, such as telemedicine, electronic records... and especially, the ethics of practice...
Doctors should also expect that we will be engaging all members of the medical profession, the push is for in-tegration of the medical profession... similar to IBP (Integrated Bar of the Philippines) for lawyers... ideally, when you take you take your oath as physician before the PRC, you’re al-ready a member of the PMA...
AHMD: You cannot practice medi-cine if you’re not a member of PMA?
DMPC: Yes, something like that... and one by one, we hope to solve the
HIGH STAKES. The future of millions of poor Filipino children in remote villages depends largely on how their elders shape the nation’s health program.
www.ambicaglobal.com | www.ambicare.net 19
Medical Digest
gargantuan problems of the medical pro-fession...
AHMD: By the way, what is the status of efforts to recover money lost by the PMA in the bank where it depos-ited...?
DMPC: The principal amount de-posited in the Export & Industry Bank is P5 million... the P6 million, which made the total P11 million, is unrealized income, meaning it would have earned that amount as interest had the bank not gone bankrupt... so far, we have recov-ered only the five-hundred-thousand pe-sos insured by PDIC (Philippine Deposit Insurance Corporation)... the only way we can gain back the rest of the money is if the bank gets rehabilitated... PMA was just one of the many unfortunate depositors of that bank... the problem is it’s being made into a political issue... it shouldn’t be made a political issue... the only thing we can do now is to make sure we deposit PMA funds in very sta-ble banks, and not get involved in high-risk investments...
AHMD: One of PMA’s major proj-ects is the planned PMA-Filinvest build-ing. What is its present status?
DMPC: With regards to the PMA-Filinvest building... We have to cut our potential losses...tearing down the Ad-ministration Building versus tearing down the Doctor’s Inn.
Transferring the PMA building to the back of the PMA Auditorium would mean that we lose the potential income for renting the spaces facing North Av-enue.
Keeping the PMA Auditorium is probably okay if we can have it declared as a national heritage site by the Nation-al Historical Commission but we have to make it an integral part of the PMA Building so our access will still be at North EDSA.
Given that...we have to shift the bur-den of refurbishing the PMA Auditori-um to Fil-invest. The contract also states that we get only Php500,000 monthly or a percentage of the earnings, whichever is higher...but we have to consider the cost of money now, the monetary infla-tion and the depreciation of the building
after 25 years. We have to cut our losses and maximize our gains.
AHMD: Bottom line, what can PMA members expect from your admin-istration?
DMPC: PMA members can expect a more vibrant PMA ... the new dispen-sation also expects more involvement from PMA members, including spe-cialty societies, in PMA activities... they seem to have awakened because in the last PMA election, around 20 to 25% of votes came from those who had never voted before...
AHMD: What’s the total number of Filipino doctors now?
DMPC: There are 72,000 doctors actually practicing in the Philippines... only 27,000 are active PMA members... that’s just around 1/3...
ASEAN 2015
AHMD: When ASEAN 2015 comes around, you will have the distinct honor of being the first PMA President to lead Filipino physicians as the nation enters this historic milestone.
Since ASEAN 2015 allows the free flow of people, services, and products in the ASEAN region, this will most likely bring a “deluge” of foreign doctors who want to practice in the Philippines.
At the same time, of course, this will open up new opportunities for Fili-pino doctors to practice in other ASEAN countries.
It should also be pointed out that most likely, other health professions (nursing, pharmacy, midwifery, med tech, etc.) will experience the same in-crease in competition and opportunities.
What are the major POSITIVE and NEGATIVE implications of ASEAN 2015 that you/PMA foresee, relative to Filipino doctors, patients, and other health professionals, as well as the en-tire Philippine health system?
DMPC: What needs to be carefully monitored is the Implementing Rules and Regulations (IRR).
It is being drafted now. PMA is involved in the drafting of the IRR, to-gether with PRC.
We do not want unbridled (unregu-lated) influx of foreign doctors... the hardliners say we don’t want that be-cause, while we want Filipino doctors to also practice and be exposed to other ASEAN countries, the fact is there will be much more of them (foreign doctors) coming here than Filipino doctors going out.
AHMD: So you see a lot of possible problems?
DMPC: You will see the problems when they’re there. If we can’t even rein in (properly regulate) our own doctors, what more doctors from oth-er countries? But since we are signato-ry to that, we just have to ensure that we have good rules regarding the practice of medicine...
AHMD: Is PMA part of an ASEAN medical organization?
DMPC: Yes, it’s part of MASEAN (Medical Association of South East Asian Nations).
AHMD: Do we envision MASE-AN becoming more a more felt and liv-ing reality by 2015?
DMPC: The current Chairman of the MASEAN Council is a Filipino, Dr. Jose Asa Sabili, past PMA President... (EDITOR’S NOTE: Other senior PMA/Filipino officials of the MASEAN Coun-cil are Dr. Marian Dobles, Deputy Sec-retary General, and Dr. Oscar Tinio, Vice Treasurer)
Let me share some basic facts about ASEAN’s Mutual Recognition Arrange-ment (MRA) on Medical Doctors for 2015.
During the Bali Concord II, it was decided to adopt at the Ninth ASEAN Summit held in 2003 the call for the completion of Mutual Recognition Ar-rangements (MRA) for qualifications in major professional services by 2008.
The intent is to facilitate free move-ment of professionals/skilled labour/tal-ents in ASEAN. The Healthcare sector is one of the twelve priority sectors that the ASEAN leaders have identified for integration and creation of the ASEAN Economic Community (AEC).
www.ambihealthmd.weebly.com20
AmbiHealth M.D.
Providing an MRA for Medical Practitioners was expected to strengthen professional capabilities by promoting the flow of relevant information and exchange of expertise, experiences and best practices suited to the specific needs of ASEAN Member States.
The objectives of this MRA are to: 1. Facilitate mobility of medical
practitioners within ASEAN; 2. Exchange information and en-
hance cooperation in respect of mutual recognition of medical practitioners;
3. Promote adoption of best practic-es on standards and qualifications; and
4. Provide opportunities for capacity building and training of medical practi-tioners.
To be recognized as a foreign medi-cal professional and be eligible to prac-tice medicine in another ASEAN state, they must have the following qualifica-tions:
1. Recognition by Professional Medical Regulatory Authority (PMRA) of country of origin Professional Regu-lation Commission, Board of Medicine and Philippine Medical Association (in the case of the Philippines) and host country;
2. Possess a valid professional reg-istration and license to practice issued by PMRA of country of origin (Profes-sional Regulation Commission, Board of Medicine, in the case of the Philip-pines);
3. Has been in active practice for five years (for physicians) (Article III of the MRA);
4. Comply with all Continuing Professional Development require-ments;
5. Certified as not having violated any professional or ethical standards, both local and international;
6. Declare that there is no inves-tigation or legal proceeding pending against him/her in the country of origin or another country;
7. Comply with any other assess-ment or requirement as may be imposed by the host country.
To the question regarding the major
POSITIVE and NEGATIVE implica-tions of ASEAN 2015 on the Philip-pine health system, we must understand that all ASEAN member states may not be able to undertake full integration by 2015 given that each member state has its own standards, procedures, and reg-ulations which makes the creation of a single market and production base more complex.
Assuming that the implementation of the MRA is to begin in the Philippines in 2015, it has both its POSITIVE and NEGATIVE implications to the country.
On the positive side, the MRA will be able to expand the Philippine market. Filipino doctors will be able to move and practice all over the ASEAN mem-ber states.
With the infusion of health technol-ogy from our ASEAN neighbors, specifi-cally Singapore and Thailand, our coun-try’s health care systems will improve.
On the negative side, the country can lose Filipino doctors through migra-tion, although such impact is still unclear since we haven’t explored the possibility of having other ASEAN medical doctors come in the country.
Presently, Medical Exchange Pro-grams between the Philippines with other ASEAN countries are already happening. Actually, there is a need for cooperation with other member states even prior to the full implementation of the MRA to gain trust and friendship of ASEAN member states.
AHMD: Are the government and medical profession fully prepared to ad-equately handle the challenges posed by ASEAN 2015? Why yes or why not?
DMPC: The impact of the MRA on medical doctors really depends on the terms and conditions that are to be written within the concessions made un-der the ASEAN Framework Agreement on Services of the MRA. It is therefore even more important now that there be mutual recognition of professional stan-dards and that our medical curriculum be in consonance with ASEAN-wide re-quirements.
AHMD: How can the Philippines
protect itself from possible medical mal-practice by doctors from other ASEAN countries? Are our present laws adequate to protect us?
DMPC: We ought to be vigilant and report all unscrupulous activities by foreign nationals. The MRA on Medi-cal Practitioners provides that “… MRA shall not reduce, eliminate, or modify the rights, power and authority of each ASEAN Member State, its PMRA and other relevant authorities to regulate and control medical practitioners and the practice of medicine.” Presently, the ASEAN is still in the process of looking at the equivalences of medical doctors with other ASEANcountries.
AHMD: How can Filipino doc-tors take full advantage of opportunities to practice in other ASEAN countries? How will this benefit our doctors?
DMPC: We are actually better off than our ASEAN counterparts because we must remember that the PMRA’s Do-mestic Regulations of the host country still need to evaluate the medical doc-tors’ qualifications, training, and expe-riences while imposing further require-ment or assessment.
Language skills and technical com-petence are still to be considered before the actual employment occurs.
In the end, the freedom to move by medical doctors does not immediately translate into employment opportuni-ties.
However, our facility with the Eng-lish language and high technical com-petence stand our medical graduates in good stead and allow them to land em-ployment opportunities not only in ASE-AN member states but in the US, Cana-da and the UK. In fact the Philippines is one of the main exporters of medical doctors in the ASEAN region.
AHMD: What are the basic pro-tective / regulatory mechanisms that government should put in place to pro-tect the Philippine health system before ASEAN 2015 comes around?
DMPC: Again, the MRA on Medi-cal Practitioners provides that “… MRA

www.ambicaglobal.com | www.ambicare.net 21
Medical Digest
EXECUTIVE OFFICERS
Maria Minerva P. Calimag, M.D.PresidentBenito P. Atienza, M.D.National TreasurerMarianne O. Dobles, M.D.Secretary GeneralJose C. Montemayor, M.D.Assistant Secretary General
BOARD OF GOVERNORS
Harry G. Soller, M.D.Northeastern LuzonFrancisco B. Ranada III, M.D.Northwestern Luzon
Raul E. Echipare, M.D.Central LuzonSalvador G. Silverio, M.D.ManilaMa. Realiza G. Henson, M.D.Quezon CityEvangeline F. Fabian, M.D.RizalRebecca W. Deduyo, M.D.Central TagalogEduardo F. Chua, M.D.Southern TagalogRufino A. Bartolabac, M.D.BicolMa. Cristina C. Danac-Delfin, M.D.Western Visayas
Ethel A. Lagria, M.D.Eastern VisayasMa. Gay M. Gonzales, M.D.Western MindanaoRuben O. Go, M.D.Northern MindanaoMaria Lourdes G. Monteverde, M.D.Southeastern MindanaoKaren Conol-Salomon, M.D.Northcentral MindanaoAngelo L. Dimaano, M.D.Caraga
New PMA Officers (2014-2015)
shall not reduce, eliminate, or modify the rights, power and authority of each ASEAN Member State, its PMRA and other relevant authorities to regulate and control medical practitioners and the practice of medicine.”
Another problem for us here in the Philippines is the restricted capacity for employment because of our decentral-ized or devolved health services, thus we experience shortages at the sub-national level. Urban areas become the areas of migration and outmigration of medical doctors.
The question of preparedness of each member country is being raised given that the bottom line of allow-ing medical doctors to work in another country can further worsen the unequal distribution of health workers causing the rural areas of the country to experi-ence understaffing.
We have a lot of medical schools and we produce something like four doctors per 100,000 population but the challenge is to make our graduates serve in our shores first before seeking em-ployment elsewhere.
Production capacity does not always translate to the availability of health pro-fessionals where we need them.
We lack specialists in many far-flung and conflict-stricken areas and
another challenge is to provide medi-cal graduates from these far-flung areas with training opportunities in accredited training programs funded with salaries coming from the local government.
We have to push for the full imple-mentation of the Magna Carta for the Healthcare Workers in order to incen-tivise practice in our rural areas.
AHMD: What has PMA done and will do to maximize benefits and mini-mize disadvantages posed by ASEAN 2015 to Filipino doctors, other health professionals, and patients?
DMPC: Considering that the PMA is part of the PMRA of the Philippines, the PMA has to push for integration of the profession so that all medical grad-uates will be under the wings of the PMA.
We have to strengthen and build ca-pacities for future leaders of the PMA not only at the national but at the local level as well.
The PMA must look at its strategic goals at national and local levels so that everyone marches in cadence.
2014 is the 111th year of the PMA and we must improve its image and its relevance among members and also among non-members so we can entice
them to join us, while we await the leg-islation that mandates the integration.
At present, the PMA is doing a na-tionwide manpower study of all medical practitioners in the country so we will know the cross-section of medical doc-tors practicing in the Philippines.
We also need to address the creden-tialing issues and program accreditation of existing training programs so that all who graduate from these training pro-grams attain credentialed status.
We will also look at the imple-mentation of eHealth initiatives (e.g., telemedicine) in rural areas that will be manned by MHU and RHU in partner-ship with private and public health in-stitutions with specialists/subspecialists to address the issue of maldistribution of physicians in the country.
We must be proactive and let advo-cacy instead of events drive all our ac-tivities at the PMA.
Transparency devoid of self-inter-ests and truthful information dissemina-tion is important so that all physicians will know all the national and interna-tional issues that will impact on their practice come the ASEAN 2015.
All initiatives are expected to re-dound towards patient safety.

www.ambihealthmd.weebly.com22
AmbiHealth M.D.
In a few months, ASEAN 2015 will become reality: The official start of Regional Integration of national econ-omies in the ASEAN Region.
Among many other implications, Regional Integration means ASEAN doctors will be allowed to practice in all ASEAN countries, subject to cer-tain rules.
Suddenly, we will all be compelled to think REGIONAL -- ASEAN -- not just NATIONAL. A truly profound para-digm shift for all ASEAN citizens.
When it happens, chances are for all doctors in the ASEAN Region, one organization will suddenly take center stage: MASEAN, or the Medical Asso-ciation of South East Asian Nations.
Logically, it will be at the forefront of efforts to find ways to smoothly in-tegrate the practice of medicine within ASEAN. Not an easy task at all, con-sidering the immense hurdles that lie ahead, such as harmonizing inevita-ble conflicts of interests and cultures between medical professionals from different ASEAN countries.
High time, then, to start getting to know a bit more about this organiza-tion which will most likely have a major impact on the lives of Filipino doctors, as well as on their counterparts in oth-er ASEAN nations.
From its website, http://masean.wordpress.com/masean-council/, we get the following basic information:
About MASEANThe preparatory meeting of the
medical associations of the member states of the Association of South East Asian Nations (ASEAN) was held in Jakarta, Indonesia, from 29 February to 1 March 1980 to consider the estab-lishment of the Medical Association of South East Asian Nations (MASEAN).
This was held in response to the recognition of the importance of mu-tual cooperation and collective effort among the national medical associa-tions in attaining the highest possible level of healthcare for people in the re-gion and in upholding the image and
dignity of the medical pro-fession.
D e l -egates from I ndones ia , M a l a y s i a , Philippines, S i n g a p o r e and Thailand met to study the feasibil-
ity of establishing a cooperative as-sociation in order to pool talents and resources, to formulate programmes for studies and research as well as to improve the services in healthcare de-livery to the people of our nations.
It was envisaged that the frame-work of the proposed organisation would allow for the exchanges of views, information and resources for projects and programmes.
The preparatory meeting culmi-nated in the formation of MASEAN, which was inaugurated on 10 April 1980 in Penang, Malaysia. OBJECTIVES
The main objectives of MASEAN are:
• To promote close ties among the national medical associations and physicians in ASEAN;
• To foster the study and dissemi-nation of all aspects of medical knowl-edge;
• To study and report on the prob-lems which confront the profession in the region; and
• To establish common policies in attaining the highest possible level of healthcare for the people.
Past MASEAN Meetings
The 1st MASEAN Council Meeting was held immediately after the Inau-gural Ceremony and Dr M. K. Rajaku-mar, the then President of the Malay-sian Medical Association was elected Chairman of MASEAN for a two-year term. On 30 January 1981, MASEAN was accepted by ASEAN as an affili-
ate with non-government status.
MEMBER ASSOCIATIONSMASEAN is composed of the fol-
lowing associations:• Brunei Medical Association• Cambodia Medical Association• Indonesian Medical Association• Medical Association of Lao PDR• Malaysian Medical Association• Myanmar Medical Association• Philippine Medical Association• Singapore Medical Association• Medical Association of Thailand• Vietnam Medical Association
MASEAN CouncilChairman: Dr Jose Asa Sabili (Philippine Medical Association)Vice Chairman: Dr Tran Huu Thang (Vietnam Medical Association)Secretary General: Dr Lee Yik Voon (Singapore Medical Association)Deputy Secretary General: Dr Marian Dobles (Philippine Medical Association)Treasurer: Dr Tammy Chan (Singapore Medical Association)Vice Treasurer: Dr Oscar Tinio (Philippine Medical Association)
MASEAN Secretariat Contact address: Dr LEE Yik VoonSecretary GeneralAddress: MASEAN c/o Singapore Medical Association, 2 College Road, Level 2 , Alumni Medical CentreSingapore 169850Tel: +65 6223 1264Fax:+65 6224 7827Website:http://masean.wordpress.comEmail: [email protected]
For queries in relation to each country, please email that country’s medical association directly.
by AHMD Research Group
Crucial Role in 2015?masean: masean members
Brunei Medical Association
Cambodia Medical Association
(No logo)
Malaysian Medical Association
Myanmar Medical Association
Indonesian Medical Association
Medical Association of Lao PDR
Philippine Medical Association
Singapore Medical Association
Medical Association of Thailand
Vietnam Medical Association
(No logo)

www.ambicaglobal.com | www.ambicare.net 23
Medical Digest
In a few months, ASEAN 2015 will become reality: The official start of Regional Integration of national econ-omies in the ASEAN Region.
Among many other implications, Regional Integration means ASEAN doctors will be allowed to practice in all ASEAN countries, subject to cer-tain rules.
Suddenly, we will all be compelled to think REGIONAL -- ASEAN -- not just NATIONAL. A truly profound para-digm shift for all ASEAN citizens.
When it happens, chances are for all doctors in the ASEAN Region, one organization will suddenly take center stage: MASEAN, or the Medical Asso-ciation of South East Asian Nations.
Logically, it will be at the forefront of efforts to find ways to smoothly in-tegrate the practice of medicine within ASEAN. Not an easy task at all, con-sidering the immense hurdles that lie ahead, such as harmonizing inevita-ble conflicts of interests and cultures between medical professionals from different ASEAN countries.
High time, then, to start getting to know a bit more about this organiza-tion which will most likely have a major impact on the lives of Filipino doctors, as well as on their counterparts in oth-er ASEAN nations.
From its website, http://masean.wordpress.com/masean-council/, we get the following basic information:
About MASEANThe preparatory meeting of the
medical associations of the member states of the Association of South East Asian Nations (ASEAN) was held in Jakarta, Indonesia, from 29 February to 1 March 1980 to consider the estab-lishment of the Medical Association of South East Asian Nations (MASEAN).
This was held in response to the recognition of the importance of mu-tual cooperation and collective effort among the national medical associa-tions in attaining the highest possible level of healthcare for people in the re-gion and in upholding the image and
dignity of the medical pro-fession.
D e l -egates from I ndones ia , M a l a y s i a , Philippines, S i n g a p o r e and Thailand met to study the feasibil-
ity of establishing a cooperative as-sociation in order to pool talents and resources, to formulate programmes for studies and research as well as to improve the services in healthcare de-livery to the people of our nations.
It was envisaged that the frame-work of the proposed organisation would allow for the exchanges of views, information and resources for projects and programmes.
The preparatory meeting culmi-nated in the formation of MASEAN, which was inaugurated on 10 April 1980 in Penang, Malaysia. OBJECTIVES
The main objectives of MASEAN are:
• To promote close ties among the national medical associations and physicians in ASEAN;
• To foster the study and dissemi-nation of all aspects of medical knowl-edge;
• To study and report on the prob-lems which confront the profession in the region; and
• To establish common policies in attaining the highest possible level of healthcare for the people.
Past MASEAN Meetings
The 1st MASEAN Council Meeting was held immediately after the Inau-gural Ceremony and Dr M. K. Rajaku-mar, the then President of the Malay-sian Medical Association was elected Chairman of MASEAN for a two-year term. On 30 January 1981, MASEAN was accepted by ASEAN as an affili-
ate with non-government status.
MEMBER ASSOCIATIONSMASEAN is composed of the fol-
lowing associations:• Brunei Medical Association• Cambodia Medical Association• Indonesian Medical Association• Medical Association of Lao PDR• Malaysian Medical Association• Myanmar Medical Association• Philippine Medical Association• Singapore Medical Association• Medical Association of Thailand• Vietnam Medical Association
MASEAN CouncilChairman: Dr Jose Asa Sabili (Philippine Medical Association)Vice Chairman: Dr Tran Huu Thang (Vietnam Medical Association)Secretary General: Dr Lee Yik Voon (Singapore Medical Association)Deputy Secretary General: Dr Marian Dobles (Philippine Medical Association)Treasurer: Dr Tammy Chan (Singapore Medical Association)Vice Treasurer: Dr Oscar Tinio (Philippine Medical Association)
MASEAN Secretariat Contact address: Dr LEE Yik VoonSecretary GeneralAddress: MASEAN c/o Singapore Medical Association, 2 College Road, Level 2 , Alumni Medical CentreSingapore 169850Tel: +65 6223 1264Fax:+65 6224 7827Website:http://masean.wordpress.comEmail: [email protected]
For queries in relation to each country, please email that country’s medical association directly.
by AHMD Research Group
Crucial Role in 2015?masean: masean members
Brunei Medical Association
Cambodia Medical Association
(No logo)
Malaysian Medical Association
Myanmar Medical Association
Indonesian Medical Association
Medical Association of Lao PDR
Philippine Medical Association
Singapore Medical Association
Medical Association of Thailand
Vietnam Medical Association
(No logo)

www.ambihealthmd.weebly.com24
AmbiHealth M.D.
Food and Drug Administration (FDA) Acting Director General Dr. Kenneth Y. Hartigan-Go stressed the important role of regulators in achieving Kalusugan Pangkala-hatan (universal health care) and access to medicines guaranteeing the quality, efficacy and safety of medicines which entails monitor-ing the whole life cycle of drugs starting from manufacturing up to consumption.
He said this during a recent Pol-icy Dialogue on Universal Health Care and Access to Medicines.
He emphasized the key func-tions of FDA which include: the creation of regulatory standards; inspection and licensing of drug establishment; levying penalties for violators; conducting laboratory tests for health products; and post-marketing surveillance.
Borrowing the World Health Organization’s concept of health
system strengthening, Go empha-sized that Kalusugan Pangkala-hatan cannot be dissociated with
strengthening health systems – human re-source health, logistics, good governance, in-formation and c o m m u n i c a -tion technology, health products, and healthcare financing – and challenges can be best ad-dressed with a holistic commu-nity approach
which encour-ages the engagement of every stakeholder from other govern-ment agencies to the industry as well as health professionals and consumers.
First, compliance to good man-ufacturing practice (GMP) needs to be strictly enforced in order to ensure the quality, efficacy, and safety of drugs. The FDA is now more than ever vigilant in meeting this obligation to safeguard public health. However, the FDA would want to be more proactive by con-ducting on-site GMP inspections of drug manufacturers abroad in order to guarantee the quality, safety, and efficacy of imported medicines.
On changing irrational and improper prescribing behavior of medical practitioners, the FDA is fully aware of the need to address the unethical marketing promo-
tions. Accurate information on drugs is very essential as these pieces of information influence the choice of medicines. Likewise, prescriptions also have a great in-fluence in the choice of medicines. The FDA takes full responsibility of monitoring the unethical marketing practices. In the coming months, the FDA will implement the Asia-Pacific Economic Cooperation (APEC) Declaration of Ethical Mar-keting Practices in the country to address this issue.
The prescription of generic drugs is also an issue. Recent data show that the Philippines is still a branded market when it comes to drugs. This is alarming given that the Generics Law of the Philip-pines, marks its 25th anniversary this year. However, a more press-ing issue is the question on the quality of generic drugs. To date, the FDA cannot guarantee the quality, safety, and efficacy of ge-neric drugs due to lack of resourc-es to test the drugs, but the FDA is not stopping there. The FDA is now working on requiring bioavail-ability and bioequivalence (BA/BE) analyses for generic drugs.
To continuously monitor the quality of drugs available in the market, the FDA is strengthening its post-marketing surveillance. The FDA has already established its Regulatory Enforcement Unit which now requires companies to provide risk management plans, including the voluntary recall of products if proven unsafe, sub-standard and ineffective.
The FDA has already estab-lished an e-reporting system for
by Abram Joseph Magnaye DOH Research Fellow
Reprinted from HealthBeat Magazine; www.doh.gov.ph
Trust the Regulators
www.ambicaglobal.com | www.ambicare.net 25
Medical Digestadverse drug reactions (ADR) providing an avenue for consum-ers to lodge their complaints on the safety, quality, and efficacy of medicines. It is also complement-ed with the continuous advocacy on pharmacovigilance and the ongoing education and promotion efforts to increase awareness on ADR.
Moreover, the FDA is also lay-ing down other innovations in reg-ulatory reform, like a Micro, Small and Medium Enterprises unit that will be closely working with the Department of Trade and Industry to help address the compliance and investment issues of the phar-maceutical sector. In addition, the FDA is challenging the Pharmacy Law with regard the deregulation of the requirement for pharma-cists in drugstores. The significant mismatch between the number of drugstores and licensed pharma-cists poses a challenge to access
to medicines with drugstores fac-ing closure with this stringent re-quirement and potentially reduc-ing the accessibility of medicines especially in remote areas.
However, it must be noted that FDA’s role in Kalusugan Pangka-lahatan spans many other health product categories under its re-mit such as food, cosmetics, and medical devices. This amounts to about Php 2.2 trillion of household expenditures on the products di-rectly monitored by the agency, and may even reach Php 3.3 tril-lion of household expenditures if other sectors that are indirectly monitored by the FDA are in-cluded. Thus, the FDA is actually in the frontline and bottleneck of access to medicines, inclusive growth and sustainable develop-ment.
Go said that the FDA dutifully accepts its mandate, but without the support and the resources to
fulfill its duties, it may turn into a ‘white elephant.’ Amidst the fi-nancial constraints of the agency, he believes that the agency is not being a very effective regu-lator. There is still so much to be done. The regulator needs to be equipped, but there is no school for regulators to equip them with the science of regulation. Also, the regulator needs to be protected from any political and economic agenda that can compromise its regulatory obligation to the public. Finally, the FDA must be strength-ened with improved science, equipment, and facilities in order to register better products, in turn, gaining credibility as a regulator.
Finally, Go called on stake-holders to trust the regulators. Amidst all the financial challeng-es the FDA faces, it has been showing resiliency and is making a statement that it will not back down in doing its mandate.
Since July 2013, the Department of Health’s (DOH) im-munization program has included free immunization against pneumonia in children in the country’s health centers.
“We (have introduced) the Pneumococcal Conjugate Vaccine (PCV) to the Philippine vaccination program for infants,” Secretary of Health Enrique Ona revealed, adding that this is another historical milestone to the DOH Expand-ed Program on Immunization (EPI).
According to the Philippines Health Statistics of 2010, pneumonia ranks as the second leading cause of infant mor-tality in 2010, which accounts for 2,628 deaths.
“Pneumonia can cost up to P23,500 for hospitalization, including professional fee, consultation, laboratory tests and medication,” the health chief said. The vaccine costs P2,050 per full vaccination (three doses of the PCV) per child.
Integration of PCV started with two regions, Autono-mous Regions in Muslim Mindanao (ARMM) and Caraga, as the first recipients of the PCV. Additional regions will be included every year for administration of pneumococcal vaccines until 100% of the regions are covered.
Caraga was chosen for initial PCV implementation to complement the Rotavirus vaccination that started in July 2012. Same region was selected as the site for the impact study on the rotavirus vaccination, which will end on 2014.
Regions ARMM and Caraga, ranked number 13 among the regions with high number of pneumonia cases.
The vaccine was given to 333,000 infants aged between six months to 11 months old residing in the provinces and cities of Caraga and the ARMM. These infants represent the 14% of the 2.4 million target infants nationwide.
“This is part of our goal to achieve better health outcomes and meet our health-related Millennium Development Goals by strengthening existing public health programs, such as expanding immunization interventions,” Ona concluded.
The DOH Expanded Program on Immunization provides FREE vaccines that protect infants and children from the common vaccine preventable diseases. Vaccines include BCG for childhood tuberculosis, rotavirus vaccine, measles-mumps-rubella vaccines (MMR), polio vaccine, and pen-tavalent vaccine, which is a combination of Diphtheria-Per-tusis-Tetanus-Hepatitis B-Haemophilus influenza vaccines.
Data Source: Official Gazette online, managed and maintained by the Presidential Communications Development and Strategic Planning Office and PREGINET (http://www.gov.ph/2013/07/17/doh-vaccine-vs-pneumonia-in-children-now-part-of-government-immunization-program/)
DOH gives free anti-pneumonia vaccine for children
www.ambihealthmd.weebly.com26
AmbiHealth M.D.
Services OfferedImportation & Warehousing
Ambica can handle the importation of client’s quality medicines at an affordable price.
Importation of medicines takes place as soon as the purchase order is released by the client.
Upon arrival of the products, the cli-ent can take delivery of the stock in partial monthly batches, if so desired. This will solve client’s storage concerns.
Under this arrangement, client can ar-range for partial deliveries even on short notice, while remaining inventories are se-curely stored in Ambica’s warehouse, to be released as per requirements of client with-out extra charge.
Ambica can store 3 to 4 months inven-tory for the client.
Example: If there are 2,000 boxes to be consumed in 4 months, then we will deliver 500 boxes every 1st week of the month until the fourth month.
Marketing SurveysAmbica can provide client with accu-
rate, timely, and relevant information about the feasibility of a product’s success in the market using in-depth research, IMS data, drugstore chain surveys, and many more.
Information such as who are the leading competitors in the market for a given therapy or product. This will give a competitive edge for those who want to launch new therapies or products to the market.
Information SystemAmbica can offer client in-depth infor-
mation on sales, performance, statistics seg-
regated per region or area of a given prod-uct through survey, research, interviews and corporate connections.
Sales & MarketingAmbica has the national marketing net-
work, experience, and expertise to help place client’s product in a viable market po-sition within a reasonable time frame.
Product Launch & ExhibitionAmbica can give client’s product a boost
in the market through Product Launch & Ex-hibition, with appropriate advertising and PR support.
RegulatoryClient can tap Ambica to get their Prod-
uct Dossier/Samples evaluated and regis-tered at FDA-Philippines to receive the Certif-icate of Product Registration in due course.
Ambica can also handle monitoring and research of drug effects as deemed neces-sary for a given product.
OthersAmbica can perform assay testing for
products which can be assayed in Philip-pines.For inquiries, please contact:
AMBICA INTERNATIONAL CORPORATIONNo. 9 Amsterdam Extension, Merville Park Subdivision, Paranaque City), Metro Manila, PHILIPPINESPhones: (632) 828-6617 to 18; 828-6542Fax: (632) 828-6615Mobile: (0917)554-6073; (0917)839-7430E-mail: [email protected]: www.ambicaglobal.com
AMBICA
www.ambicaglobal.com | www.ambicare.net 27
Medical Digest
Queens: Exotic Culinary Nirvana!
Queens Taj Mahal Indian Restaurant146 Jupiter StreetMakati, Philippines
Reservation and Delivery: +63 922 870 8482Dine-in and Delivery: +63 (02) 895 1316
e-mail: [email protected]
www.queenstajbollywood.com
Queens at Bollywood3/F Greenbelt 3 Ayala Center
Makati, PhilippinesReservation: +63 (02) 757 3536, +63 (02) 903 0710
Dine-in: +63 922 870 8483Quick Delivery: +63 2121212
e-mail: [email protected]
QUEENS is primarily an Indian restaurant which also serves Indonesian and Indo-Asian Fusion cuisines. We serve a highly select variety of 200 non-vegetarian dishes, 80 vegetarian dishes and sweet desserts. We offer chicken, lamb, eggs, and seafood which includes crabs, fish, prawns and shrimp. Our dishes are all authentic, fresh and high quality to ensure unforgettable, excellent meals for our guests. QUEENS TAJ MAHAL at 146-B Jupiter Street, BelAir 2, Makati Avenue is open 12 noon to 4 PM; 6 PM to 11 PM, Sunday to Thursday; and from Friday to Saturday, 12 noon to 4 PM; 6 PM to 12 midnight; delivery hotline 02-8951316/+639228708482. QUEENS AT BOLLYWOOD at Greenbelt 3, 3rd level, Ayala Mall, Makati City, is open 12 noon to 12 midnight Sunday to Thursday; and from Friday to Saturday, 12 noon to 2 AM. For delivery: Call 212-1212.
SPICY ROAST LAMB. Also known as Raan in lamb leg marinated in spices and roasted.
BIRYANI. Aromatic rice cooked fresh with your choice of chicken, fish, mutton, or vegetables and garnished with fresh herbs.
CHICKEN TANDOORI. Chicken marinat-ed overnight in yogurt and freshly ground-ed spices and grilled to perfection in the tandoor.
ALOO GOBI MUTTER. Potatoes, cauli-flower and green peas. Nicely tossed with tomato, fresh coriander and Indian spices.
NAAN ON THE RAAN. Spicy roasted lamb pieces rolled on a naan, served with masala fries and chutney salad.
We cater and deliver!
KULFI. Indian flavored refreshing ice cream in three choices: Mango, Almond, Pistachio.

www.ambihealthmd.weebly.com28
AmbiHealth M.D.
DOH: TB Still Major ProblemIt is the sixth leading cause of death and
illness in PH. It is estimated that 260,000 Filipinos have active TB and the country is among the 22 “high-burden” countries for TB epidemic. Along with China, Cambodia, and Vietnam, it accounted for 93 per cent of TB cases in Western PacificRegion.
But despite the high TB incidence, significant progress has been made in in-creasing case detection and treatment in the country. The World Health Organization (WHO) Global Tuberculosis Report 2012 showed the number of Filipinos afflicted with TB decreased by 52 percent and TB casualties by 49 percent. TB prevalence is high among the high risk groups such as the elderly, urban poor, smokers and those with compromised immune systems such as people living with HIV, malnutrition and diabetes. It is estimated that 10,600 pa-tients have MDR-TB in 2011. This situation leads to substantial socio-economic losses to the country.
TB is an infectious bacterial disease that most commonly affects the lungs. It is transmitted from person-to-person via drop-lets from the throat and lungs of people with the active TB. Signs and symptoms can occur in the first few weeks after infection with the bacteria, or it can occur a few years later. In healthy individuals, infection often causes no symptoms, since the person’s immune system acts to wall off the bacte-ria. The symptoms of active TB of the lungs are coughing, sometimes with sputum or blood, chest pains, weakness, weight loss, fever and night sweats. TB can also affect other organs of the body, such as the kid-neys, spine or brain. Symptoms depend on the organ affected. It is important that TB should be checked and treated as early as
possible. Filipinos need not suffer from
TB nor hide from the stigma that has been attached to the disease for decades that prevent them from receiving proper treatment. The DOH-NTP aims to detect 85% of active TB cases and cure at least 90% of these cases. It has adopted the Directly Observed Treatment Short-course (DOTS) program, recommended by the WHO.
Persons with TB can ac-cess free diagnostic test using sputum microscopy and anti-TB drugs from different DOTS facili-ties such as the rural health units, health centers, private clinics, some hospitals, prison clinics, and other facilities. Under DOTS, a relative or a health worker di-rectly observes the patient taking anti-TB medicines daily. The Phil-
ippines’ DOTS treatment success is placed at 90 per cent, higher than the WHO target of 85 per cent.
A major challenge in treating the dis-ease is MDR-TB. This occurs because TB patients do not adhere to the drug regimen, meaning they do not take their medicines every day for the usual six months period. Because of this, the TB bacteria develop a resistance to isoniazid and rifampicin, the two most powerful TB drugs. MDR-TB is more difficult and expensive to treat. An-other challenge is the estimated 65,000 TB cases that remain undetected and un-treated. These are called the “missing TB cases,” and each of them can spread the disease to 10 other Filipinos each year.
Thus, the fight against TB and the dis-semination of right information on its pre-vention, treatment and control must con-tinue.
DOH: Malaria Elimination Soon
“The Philippines is on course of elimi-nating malaria by 2020,” reported the De-partment of Health (DOH) during the 6th Meeting of the Asia Pacific Malaria Elimi-nation Network (APMEN) in Makati City on March 11-13, 2014.
APMEN is a network of 14 Asia-Pacific countries working towards the elimination of malaria as a public health threat.
Health Secretary Enrique T. Ona, in his speech during the welcome dinner for the delegates, said that this past decade showed significant progress in the reduc-tion of malaria cases and deaths in the country due to improved diagnostic modali-ties, the use of artemisinin-based combina-tion therapies for malaria treatment, and im-provement in vector control interventions.
He also emphasized the concerted efforts of the national and local governments, the private sector, the scientific community and international donors in their technical and financial support to the implementation of interventions.
Ona said that malaria belongs to a group of diseases with an elimination initia-tive – along with rabies, schistosomiasis, leprosy and filariasis – and forms part of the thrust of the government to achieve better health outcomes for the Filipinos, through elimination of illnesses and deaths from diseases which are entirely preventable. He added that for malaria, the government bud-get has increased from US$67,000 in 2002 to US$7.2 million in 2014, a 99% increase in 13 years. Political commitment from the local government units has also increased.
But as domestic resources increased, Ona said that these are not enough to fully achieve malaria elimination. The need for external funding persists, especially in the assurance of universal and equitable coverage of malaria interventions and the strengthening of an elimination-oriented surveillance systems.
Malaria cases declined since the mid-2000s, and have resulted in an 83% reduc-tion from 2005 to 2013, while there was a 92% reduction in the number of deaths within the same period.
Of the 53 known provinces endemic for the disease, 27 have already been de-clared malaria-free. These are Cavite, Ba-tangas, Marinduque, Catanduanes, Albay, Masbate, Sorsogon, Camarines Sur, Iloilo, Aklan, Capiz, Guimaras, Bohol, Cebu, Siquijor, Western Samar, Eastern Samar, Northern Samar, Northern Leyte, Southern Leyte, Biliran, Camiguin, Surigao Del Norte, Benguet, Romblon, Batanes and Dinagat Islands.
Malaria is a disease caused by para-site called plasmodium. It is transmitted by the bite of a mosquito vector, anopheles. The disease usually thrives in the rural and hard-to-reach areas such as in the hills, mountains and coastal areas. Disease transmission is perennial and generally higher during the rainy season. High-risk groups consist of upland subsistence farm-ers, forest workers, indigenous people and settlers in frontier areas, including migrant agricultural workers. Children under-five are also considered to be at high risk, in-cluding pregnant women.
Malaria elimination entails reducing to zero the incidence of locally acquired malaria infection in a specific geographic area as a result of deliberate efforts, with continued measures in place to prevent re-establishment of transmission(Reprinted with permission from HEALTH-beat magazine of the Department of Health; Issue No. 81 / March-April 2014)
“Flying Kiss”: New anti-TB advocacy movie. Help educate Filipinos on how to prevent and treat tuberculosis by sponsoring group or community screenings of this film, a joint proj-ect of DOH and PBSP. For inquiries send e-mail to [email protected]. Shown in photo are the movie’s lead players (L-R) Carl Guevara, Andrea Tatad, Wyn Mar-quez and Fabio Ide.
www.ambicaglobal.com | www.ambicare.net 29
Medical Digest
Liver cancer is one of the deadliest diseases because it is very difficult to detect. Often, there are no early symptoms.
Usually, by the time it is detected, it is already in a very advanced stage (tumour size already at least 10 cm) and, therefore, virtually 100% fatal.
Patients who are diagnosed too late have, at best, less than 5% chance of survival. Most die within one year af-ter diagnosis.
Early Detection: Only OptionFor liver cancer victims, the best
survival strategy is early detection. The earlier the disease is detected and aggressively treated, the greater the chances of survival. But how can early detection be done?
Good news: Now in PHThe good news for Filipino pa-
tients -- the world’s most accurate and modern tool for early detection of liver cancer is now available in the Philippines: Liver Cancer Biomarker Tests offered by the partnership of Ambica Biotechnology and Reliance Life Sciences, one of the world’s larg-est biopharma corporations, fully cer-tified by the Philippine Department of Health (DOH) as a specimen collec-tion/holding facility for referral to a special clinical laboratory.
Biomarkers“Biomarkers” or “biological / tu-
mour markers” are substances that can be found in the body when cancer is present. They can be products of can-cer cells themselves or of the body in response to cancer or other conditions. Most tumour markers are protein.
To test for the presence of tumour markers, the doctor sends a sample of the patient’s tissue to a fully qualified laboratory, such as the world-class laboratory facilities and services of the Ambica / Reliance partnership, which has the world’s largest collec-tion of cancer tissue biomarkers in one centre. It has a total of 149 bio-markers for various cancers (Breast, Cervical, Ovarian, Lung, Colon, Gas-tric, Oesophageal, Bladder, Prostate, Thyroid, Testicular, Liver, Oral and Lymphoma). For liver cancer alone, Ambica / Reliance has eight biomark-ers.
CAP AccreditationOf vital importance: All of its 149
cancer biomarkers are accredited by the College of American Pathology (CAP), thus ensuring high credibility and reliability.
Biomarkers have various uses, such as: Screening and early detec-tion of cancer, diagnosing cancer, de-termining the prognosis (outlook) for certain cancer types, determining the effectiveness of cancer treatment, and
detecting recurrent cancer.
Very affordableThe cost of biomarker testing is
very reasonable and affordable, con-sidering its lifesaving and peace-of-mind benefits. Prices range from P4,900.00 to P9,400.00 only, depend-ing on the specific type of biomarker that will be done. Speed is also a ma-jor benefit: Within five (5) days, the patient (through his/her doctor) will get the laboratory results, under strict confidentiality.
The Philippine situation regarding liver cancer is much worse than the global average. Based on data from DOH and the Philippine Cancer So-ciety, while liver cancer is the eighth most common cancer type worldwide, in the Philippines it is the third most common form of cancer among men and sixth among women.
80% of all liver cancer cases are preceded by cirrhosis. In turn, the usual causes of cirrhosis are chronic hepatitis B, hepatitis C infection, and alcoholism.
“We hope that in the near future, more and more Filipinos, especially those at high risk of having cancer – any type of cancer – will realize the extremely vital importance of EARLY DETECTION to save their lives. They should consult their respective doc-tors regarding the benefits of Cancer Biomarker Tests,” says Ambica exec-utive Job Joseph. “We encourages ev-eryone to learn more about this latest lifesaving technology: For inquiries, they can reach me at mobile 0917-548-3611; e-mail: [email protected]; landline (02) 828-6617 to 18. They can also visit our website at www.ambicaglobal.com.”
BIOMARKER TESTSby AHMD Research Staff
Best tool for early detection of liver cancer
Liver Cancer

www.ambihealthmd.weebly.com30
AmbiHealth M.D.Cagayan de Oro’s Surgeon-Photographer,Victor Francis Orencia, shares his art.
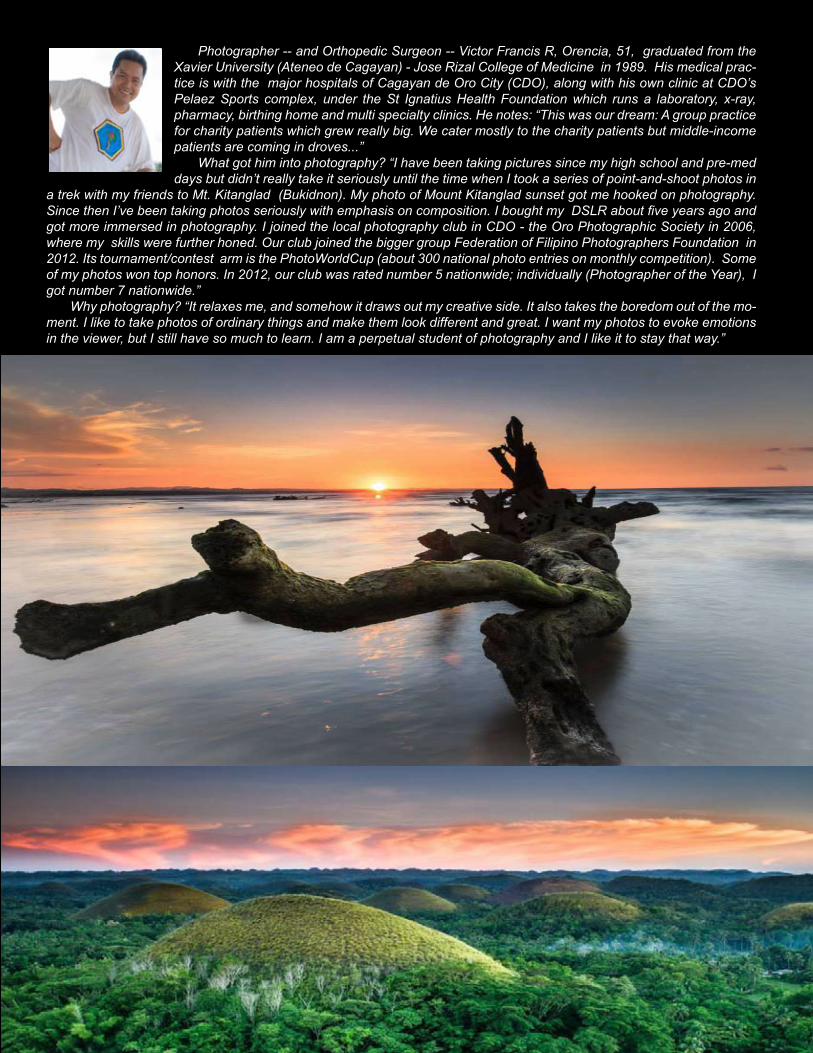
www.ambicaglobal.com | www.ambicare.net 31
Medical DigestPhotographer -- and Orthopedic Surgeon -- Victor Francis R, Orencia, 51, graduated from the
Xavier University (Ateneo de Cagayan) - Jose Rizal College of Medicine in 1989. His medical prac-tice is with the major hospitals of Cagayan de Oro City (CDO), along with his own clinic at CDO’s Pelaez Sports complex, under the St Ignatius Health Foundation which runs a laboratory, x-ray, pharmacy, birthing home and multi specialty clinics. He notes: “This was our dream: A group practice for charity patients which grew really big. We cater mostly to the charity patients but middle-income patients are coming in droves...”
What got him into photography? “I have been taking pictures since my high school and pre-med days but didn’t really take it seriously until the time when I took a series of point-and-shoot photos in
a trek with my friends to Mt. Kitanglad (Bukidnon). My photo of Mount Kitanglad sunset got me hooked on photography. Since then I’ve been taking photos seriously with emphasis on composition. I bought my DSLR about five years ago and got more immersed in photography. I joined the local photography club in CDO - the Oro Photographic Society in 2006, where my skills were further honed. Our club joined the bigger group Federation of Filipino Photographers Foundation in 2012. Its tournament/contest arm is the PhotoWorldCup (about 300 national photo entries on monthly competition). Some of my photos won top honors. In 2012, our club was rated number 5 nationwide; individually (Photographer of the Year), I got number 7 nationwide.”
Why photography? “It relaxes me, and somehow it draws out my creative side. It also takes the boredom out of the mo-ment. I like to take photos of ordinary things and make them look different and great. I want my photos to evoke emotions in the viewer, but I still have so much to learn. I am a perpetual student of photography and I like it to stay that way.”
www.ambihealthmd.weebly.com32
AmbiHealth M.D.
EDITOR’S NOTE: For easier reading, we have pro-vided subheads for the key sec-tions of this Keynote Message of Health Secretary Enrique T. Ona at the 1st Mid-Year Convention of the Philippine Society for Stem Cell Medicine, August 12, 2013, Manila Hotel. We have also set in bold type certain vital points.
Thank you for this invitation to speak on an issue that seems to be di-viding the medical community and pits the supposed medical scientists, the freewheeling practitioners and the regulatory arm of government.
Balance innovation and regulation
Stem cell therapy has been consid-ered as the future of medicine as it has been proven to be effective in several medical conditions. However, stem cell therapy is not a cure-all medical treatment. Patients have to be pre-sented first with standard of treat-ment, and in many cases, stem cell treatments have to be done in con-junction with other standard modali-ties of treatment.
Today, there is an increasing de-mand for the use of stem cells as thera-py in oncology, end-organ diseases and regenerative medicine. We see around the proliferation of “centers” offering
stem cell therapies for medical and aes-thetic purposes.
Let me start by quoting what our Food and Drug Administration, headed by Dr. Kenneth Hartigan-Go, promi-nently inscribes in its letterhead: “Find-ing the balance between innovation and sound regulation.”
Please read AO firstTwo days ago, 17 medical societies
and sub specialty societies published a one page announcement of its posi-tion on stem cell treatments, intended to warn the public of its danger of un-regulated use and urging the govern-ment, presumably the DOH and the FDA to be more vigilant in controlling the proliferation of these blatantly un-supported claims and advertisements in TV and print media on its supposed magical effects in restoring youth and vigor to aging men and women.
Lately, some of our prominent citi-zens have made personal endorsements of stem cells therapies as their “foun-tain of youth”.
I welcome all of these concerns coming from our specialty societies, especially from the sector I greatly ad-mire and respect.
However, obviously, most, if not all of them have not read the DOH administrative order published in our newspapers, numbered 2013-0012 entitled “The Rules and Regula-
tions Governing the Accreditation of Health Facilities Engaging in Human Stem Cell and Cell-Based or Cellular Therapies in the Philippines”, which was signed last March 18, 2013. They could have checked their facts first with the DOH and the FDA before releasing their statement.
The guidelines in the administrative order seek to, among others, ensure a minimum quality of service rendered by hospitals and other health facilities capable of utilizing human stem cell preparations and cell-based therapies; and guarantee that human stem cell preparations and cell-based therapies in the Philippines are safe and effective for their intended use.
TrickyIndeed, the implementation of this
administrative order is not an easy mat-ter, as we have to contend with a public so hungry to hear more of the wonders of stem cell technology, especially the “well-to-do” looking for the wellspring of beauty and eternal youth.
Defining the “accepted” from the downright “bogus claims” in stem cell use today can be tricky.
The issue is how one differentiates the “research aspect” and possible effective use from the frank claim as though it is a “standard practice.”
As a matter of fact, who decides when this thin line is breached, espe-
Official Statement by Health Secretary Enrique T. Ona, M.D., on
Stem Cell TherapySource: Philippine Department of Health
www.doh.gov.ph
Health Secretary Enrique T. Ona, M.D.
www.ambicaglobal.com | www.ambicare.net 33
Medical Digest
PROFILE: HEALTH SECRETARYOur Secretary of Health, Dr. Enrique T. Ona, is recognized as one of the top surgeons of the country specializing in the field of vascular and transplant surgery. A graduate of the Uni-versity of the Philippines, he underwent surgi-cal training in the United States and the United Kingdom. He is certified by both the Philippine and American Board of Surgery.
Upon his return to the country, he joined the faculty of the University of the Philippines and the Philippine General Hospital. He was a pro-fessor and Vice-Chair of the Department of Surgery when he was tapped to become the Executive Director of the National Kidney and Transplant Institute (NKTI), transforming the said institution into the first ISO-certified gov-ernment hospital in the Philippines. Under his leadership, NKTI is now recognized as a world class center in kidney transplantation, current-ly performing the second largest transplant program as a single institution in the world. He performed the first multi-organ transplants in Southeast Asia: liver and kidney transplant and kidney and pancreas transplant at the NKTI.
He is the recipient of numerous national and international awards, such as the Ten Out-standing Young Men (TOYM) Award in Medi-cine in 1979, The Most Outstanding Alumnus of the College of Medicine and most distin-guished alumnus of the University of the Philip-pines. He is also the first and only Filipino Sur-geon to be awarded the Honorary Fellowship of the American College of Surgeons in 2012, a singular honor for one who is already a Fel-low of the College of Surgeons.
As Secretary of Health, he has devoted re-lentlessly to the mission of attaining Kalusug-an Pangkalahatan or Universal Health Care for Filipinos, responding to the challenge of His Excellency President Benigno “Noynoy” Aquino III. In his first year, 5.3 million families or about 25 million Filipinos have been enrolled in PhilHealth. Under his administration, two land-mark health reforms have been passed, name-ly the Tobacco and Alcohol Excise Tax Reform Act of 2012 and the Responsible Parenthood and Reproductive Health Act of 2012.Source: www.doh.gov.ph
cially today when medical research from other countries often overwhelm the scientif-ic literature with various suc-cesses in one or two attempts on a few patients?
Let me answer some of these and try to revisit our AO.
Prohibitions and restrictions
Administrative Order No. 2013-0012 prohibits and restricts the creation, im-portation, promotion, mar-keting and use of stem cell therapies from embryonic, aborted fetal, and geneti-cally altered, animal and plant stem cells, as they have been proven to cause some fatal complications or tumor formations.
Permitted preparationsStem cell preparations
that are permitted for pa-tient’s use are autologous adult human stem cells, al-logeneic human stem cells, human umbilical cord stem cells and human organ-spe-cific cells.
Other key provisionsOnly DOH accredited
health facilities are allowed to use these permitted stem cell preparations.
Health facilities utilizing stem cell preparations and cell-based or cellular thera-pies are mandated to com-ply with the guidelines set by the Bioethics Advisory Board which has been estab-lished by the DOH.
This Board ensures that ethical standards are upheld and that contentious scien-tific, ethical and legal issues are addressed.
Meanwhile, an Institu-
tional Review Board re-views and approves stem cell therapies, based on the guidelines set by the Bioeth-ics Advisory Board.
Standards have been defined regarding person-nel qualifications, physical facilities, equipment and supplies, work environ-ment, quality improvement activities, records keeping and reporting of results.
Furthermore, non-hospi-tal based facilities such as free standing clinics should be affiliated with an accred-ited hospital before being al-lowed to engage in stem cell therapy.
Needed: Public vigilance and cooperation
The DOH has started strictly monitoring the com-pliance of these guidelines.
Essential to ensuring that this AO is effective is the cooperation of you, the medical practitioners and the general public.
I ask the same physicians and the various medical so-cieties to report to the DOH and FDA possible viola-tions of these guidelines, as they are in a better position to discern which among the therapies being offered are phony and which ones have sound scientific basis.
Payment issuesThe payment of services
for certain unproven applica-tions in stem cell therapies can be defined without nec-essarily measuring it only in pesos or dollars.
Crucial in determining the cost of an innovative service is differentiating the cost of supplies from that of out-right personal service.

www.ambihealthmd.weebly.com34
AmbiHealth M.D.We cannot completely adopt West-
ern practices of offering these inves-tigational therapies completely free to clinical trial participants.
This approach will not only be unaf-fordable for our institutions but very ex-pensive and will forever relegate us to be a “marketing testing ground” after others have developed a technique in their country.
Fees for translational research work must be well defined and this is where government and the private sector can work together.
ExampleLet me cite an example in my field of
interest. When we started vascular and organ transplant surgery of the kidneys, liver and pancreas in the late sixties and seventies, none of these operations were considered the standard of care.
It took several years for Medicare in the United States and other countries to consider these operations as standard of care and for government to pay for it, but research continued and fees were being paid by other parties like foundations or “out of pocket” payments.
Are we in a similar period with stem cell research and stem cell therapy to-day?
Innovative therapyFor now, most stem cells therapies fall
under what we term “innovative therapy.”Let me share with you what Professor
Patrick Taylor, Assistant Clinical Professor of Harvard Medical School and Co-Chair of the Standards Committee of the Interna-tional Society for Stem Cell Research, has to say regarding innovative therapy: “In-novative therapy develops in diverse ways. Some fields, like oncology, have pro-gressed through a close alliance between innovative therapy and research.
“With this model, innovative therapies are suggested by understanding where current therapies fail, and combining that knowledge with hypotheses about how changes in somewhat-known compounds might affect their action on other diseases.
“In clinical trials, toxic compounds of uncertain risks are offered to large cohorts, and the results, if positive, are incorporated in medical practice.
“However, other fields, like surgery, take a very different tack: innovative therapy to address an unexpected anom-aly intraoperatively can be suddenly re-
quired, and predetermined adherence to a protocol might be a fatal rigidity. Only later, after multiple experiences — and per-haps never — may a surgeon test the novel procedure through clinical research, and on many patients.
“Even then it may be difficult to ‘re-duce’ a patient to a randomized research subject if the surgeon is convinced that the novel procedure is better, or that choosing the best care option requires patient-specif-ic judgment.”
Basic questionsProfessor Insoon Hyun of the Case
Western Reserve University School of Medicine, in his article in the Journal of Law, Medicine and Ethics, raised the fol-lowing questions as regards the regulatory approach towards stem cell therapies:
Under what circumstances should • stem cell-based innovative therapies be allowed outside the context of a clinical trial? And • how should attempts at new stem cell-based therapies be regu-lated?
Concerns on regulation of stem cell therapies comes at a time when the inter-est of patients in stem cell medical travel is increasing in our country.
The 2008 guidelines of the Interna-tional Society for Stem Cell Research (ISSCR) recommends — even while condemning fraud and generally urging research — that some limited innovative administration of unproven stem cell therapies be permissible outside a re-search setting.
Ethical usesThe World Medical Association’s
Declaration of Helsinki which was last updated in October 2008, Article 35 out-lines the ethical uses of Innovative Treatment:[1] “In the treatment of a pa-tient, where proven interventions do not
exist or have been ineffective, the phy-sician, after seeking expert advice, with informed consent from the patient or a legally authorized representative, may use an unproven intervention if in the physician’s judgement it offers hope of saving life, re-establishing health or alleviating suffering.”
Article 35 then continues that when-ever possible, the innovative treat-ment should also be made the object of research, designed to evaluate its safety and efficacy. However, unlike formal clinical trials which are based
on gathering data rather than benefiting an individual patient,[2] the principle of innovative therapy is not solely aimed at producing generalizable knowledge but rather to improve an individual patient’s condition.[3]
The challenge, I believe among us, seemingly competing forces, is to sit down and craft a path of consensus, taking in consideration the most fundamental tenet why our profession exists: to save life, to alleviate pain, to do no harm.
Academic pretensions?In closing, let me pose this question
to this aggrupation: Is there a need now to organize a separate society with aca-demic pretensions akin to specialization or only an organization of physicians with interest in this developing field?
I’m afraid of a situation where title might precede competence.
I therefore ask the organizers to fur-ther review the initiatives of starting the granting of fellowships to our colleagues with particular interest in this field but only with minimal exposure to training in this complex field.
I look forward to more discussion and a happy resolution of these issues on stem cell therapy. I hope this summit brings us closer to that goal.
[1] World Medical Association (WMA) Decla-ration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects, 59th WMA Gen-eral Assembly, Seoul, Korea, October 2008
[2] Patrick L. Taylor, “Overseeing Innovative Therapy Without Mistaking it for Research: A Func-tion-Based Model Based on Old Truths, New Capaci-ties, and Lessons From Stem Cells”, Journal of Law Medicine and Ethics 2010, p.287.
[3] Insoo Hyun, “Allowing Innovative Stem Cell-Based Therapies Outside of Clinical Trials: Ethical and Policy Challenges,” Journal of Law, Medicine and Ethics, Symposium on Law, Science and Innova-tion, Summer 2010, p. 279.
Stem cell. Image courtesy of dream designs at FreeDigitalPhotos.net

www.ambicaglobal.com | www.ambicare.net 35
Medical Digest
A SUBSIDIARY OF AIC GROUP OF COMPANIESFor details on Molecular Medicine Services, please call Ambica BiotechnologiesTel. No. 828-6617 to 18, visit our website www.ambicaglobal.come-mail us at [email protected]
A SUBSIDIARY OF AIC GROUP OF COMPANIES

www.ambihealthmd.weebly.com36
AmbiHealth M.D.
Our Global Network of Principals
AMBICA

www.ambicaglobal.com | www.ambicare.net 37
Medical Digest
A SUBSIDIARY OF THE AIC GROUP OF COMPANIES

www.ambihealthmd.weebly.com38
AmbiHealth M.D.
A paper diagnostic for cancerLow-cost urine test developed by Massachusetts Institute of Technology
(MIT) engineers amplifies signals from growing tumors to detect disease.by Anne Trafton, MIT News Office, January 6, 2014BREAKTHROUGH
Cancer rates in developing nations have climbed sharply in recent years, and now account for 70 percent of cancer mortality worldwide. Early detection has been proven to improve out-comes, but screening approaches such as mam-mograms and colonoscopy, used in the devel-oped world, are too costly to be implemented in settings with little medical infrastructure.
To address this gap, MIT engineers have de-veloped a simple, cheap, paper test that could improve diagnosis rates and help people get treated earlier. The diagnostic, which works much like a pregnancy test, could reveal within minutes, based on a urine sample, whether a per-son has cancer. This approach has helped detect infectious diseases, and the new technology al-lows non-communicable diseases to be detected using the same strategy.
The technology, developed by MIT profes-sor and Howard Hughes Medical Institute inves-tigator Sangeeta Bhatia, relies on nanoparticles that interact with tumor proteins called proteas-es, each of which can trigger release of hundreds of biomarkers that are then easily detectable in a patient’s urine.
“When we invented this new class of syn-thetic biomarker, we used a highly specialized instrument to do the analysis,” says Bhatia, the John and Dorothy Wilson Professor of Health Sciences and Technology and Electrical Engi-neering and Computer Science. “For the devel-oping world, we thought it would be exciting to adapt it instead to a paper test that could be performed on unprocessed samples in a rural setting, without the need for any specialized equipment. The simple readout could even be transmitted to a remote caregiver by a picture on a mobile phone.”
Bhatia, who is also a member of MIT’s Koch Institute for Integrative Cancer Research and In-stitute for Medical Engineering and Science, is the senior author of a paper describing the par-ticles in the Proceedings of the National Acad-emy of Sciences the week of Feb. 24. The pa-per’s lead authors are graduate student Andrew Warren, postdoc Gabriel Kwong, and former postdoc David Wood.
Amplifying cancer signalsIn 2012, Bhatia and colleagues introduced
the concept of a synthetic biomarker technol-ogy to amplify signals from tumor proteins that would be hard to detect on their own. These proteins, known as matrix metalloproteinases (MMPs), help cancer cells escape their original locations by cutting through proteins of the ex-tracellular matrix, which normally holds cells in
place.The MIT nanopar-
ticles are coated with peptides (short protein fragments) targeted by different MMPs. These particles con-gregate at tumor sites, where MMPs cleave hundreds of peptides, which accumulate in the kidneys and are ex-creted in the urine.
In the original ver-sion of the technology, these peptides were detected using an in-strument called a mass spectrometer, which analyzes the molecular makeup of a sample. However, these instru-ments are not readily available in the devel-oping world, so the re-searchers adapted the particles so they could be analyzed on paper, using an approach known as a lateral flow assay — the same technology used in pregnancy tests.
To create the test strips, the researchers first coated nitrocellulose paper with antibodies that can capture the peptides. Once the peptides are captured, they flow along the strip and are ex-posed to several invisible test lines made of oth-er antibodies specific to different tags attached to the peptides. If one of these lines becomes visible, it means the target peptide is present in the sample. The technology can also easily be modified to detect multiple types of peptides re-leased by different types or stages of disease.
“This is a clever and inspired technology to develop new exogenous compounds that can detect clinical conditions with aberrantly high protease concentrations,” says Samuel Sia, an associate professor of biological engineering at Columbia University who was not involved in the research. “Extending this technology to detection by strip tests is a big leap forward in bringing its use to outpatient clinics and decen-tralized health settings.”
In tests in mice, the researchers were able to accurately identify colon tumors, as well as blood clots. Bhatia says these tests represent the first step toward a diagnostic device that could someday be useful in human patients.
“This is a new idea — to create an excreted biomarker instead of relying on what the body
gives you,” she says. “To prove this approach is really going to be a use-ful diagnostic, the next step is to test it in patient populations.”
Developing diagnostics To help make that happen, the
research team recently won a grant from MIT’s Deshpande Center for Technological Innovation to devel-op a business plan for a startup that could work on commercializing the technology and performing clinical trials.
Bhatia says the technology would likely first be applied to high-risk populations, such as peo-ple who have had cancer previous-ly, or had a family member with the disease. Eventually, she would like to see it used for early detection throughout developing nations.
Such technology might also prove useful in the United States, and other countries where more
advanced diagnostics are available, as a simple and inexpensive alternative to imaging. “I think it would be great to bring it back to this setting, where point-of-care, image-free cancer detec-tion, whether it’s in your home or in a pharmacy clinic, could really be transformative,” Bhatia says.
With the current version of the technology, patients would first receive an injection of the nanoparticles, then urinate onto the paper test strip. To make the process more convenient, the researchers are now working on a nanoparticle formulation that could be implanted under the skin for longer-term monitoring.
The team is also working to identify signa-tures of MMPs that could be exploited as bio-markers for other types of cancer, as well as for tumors that have metastasized.
The research was funded by a National Sci-ence Foundation Graduate Research Fellow-ship, a Mazumdar-Shaw International Oncology Fellowship, the Ruth L. Kirschstein National Research Service Award from the National Insti-tutes of Health, the Burroughs Wellcome Fund, the National Cancer Institute, and the Howard Hughes Medical Institute.
Reprinted with permission of MIT News (http://web.mit.edu/newsoffice/)http://web.mit.edu/newsoffice/2014/a-pa-per-diagnostic-for-cancer-0224.html
The paper test strips, which work similar to a pregnancy test, reveal the presence of proteins associated with cancer. They can also be designed to detect other dis-eases. PHOTO: BRYCE VICKMARK

www.ambicaglobal.com | www.ambicare.net 39
Medical Digest
A paper diagnostic for cancerLow-cost urine test developed by Massachusetts Institute of Technology
(MIT) engineers amplifies signals from growing tumors to detect disease.by Anne Trafton, MIT News Office, January 6, 2014BREAKTHROUGH
Cancer rates in developing nations have climbed sharply in recent years, and now account for 70 percent of cancer mortality worldwide. Early detection has been proven to improve out-comes, but screening approaches such as mam-mograms and colonoscopy, used in the devel-oped world, are too costly to be implemented in settings with little medical infrastructure.
To address this gap, MIT engineers have de-veloped a simple, cheap, paper test that could improve diagnosis rates and help people get treated earlier. The diagnostic, which works much like a pregnancy test, could reveal within minutes, based on a urine sample, whether a per-son has cancer. This approach has helped detect infectious diseases, and the new technology al-lows non-communicable diseases to be detected using the same strategy.
The technology, developed by MIT profes-sor and Howard Hughes Medical Institute inves-tigator Sangeeta Bhatia, relies on nanoparticles that interact with tumor proteins called proteas-es, each of which can trigger release of hundreds of biomarkers that are then easily detectable in a patient’s urine.
“When we invented this new class of syn-thetic biomarker, we used a highly specialized instrument to do the analysis,” says Bhatia, the John and Dorothy Wilson Professor of Health Sciences and Technology and Electrical Engi-neering and Computer Science. “For the devel-oping world, we thought it would be exciting to adapt it instead to a paper test that could be performed on unprocessed samples in a rural setting, without the need for any specialized equipment. The simple readout could even be transmitted to a remote caregiver by a picture on a mobile phone.”
Bhatia, who is also a member of MIT’s Koch Institute for Integrative Cancer Research and In-stitute for Medical Engineering and Science, is the senior author of a paper describing the par-ticles in the Proceedings of the National Acad-emy of Sciences the week of Feb. 24. The pa-per’s lead authors are graduate student Andrew Warren, postdoc Gabriel Kwong, and former postdoc David Wood.
Amplifying cancer signalsIn 2012, Bhatia and colleagues introduced
the concept of a synthetic biomarker technol-ogy to amplify signals from tumor proteins that would be hard to detect on their own. These proteins, known as matrix metalloproteinases (MMPs), help cancer cells escape their original locations by cutting through proteins of the ex-tracellular matrix, which normally holds cells in
place.The MIT nanopar-
ticles are coated with peptides (short protein fragments) targeted by different MMPs. These particles con-gregate at tumor sites, where MMPs cleave hundreds of peptides, which accumulate in the kidneys and are ex-creted in the urine.
In the original ver-sion of the technology, these peptides were detected using an in-strument called a mass spectrometer, which analyzes the molecular makeup of a sample. However, these instru-ments are not readily available in the devel-oping world, so the re-searchers adapted the particles so they could be analyzed on paper, using an approach known as a lateral flow assay — the same technology used in pregnancy tests.
To create the test strips, the researchers first coated nitrocellulose paper with antibodies that can capture the peptides. Once the peptides are captured, they flow along the strip and are ex-posed to several invisible test lines made of oth-er antibodies specific to different tags attached to the peptides. If one of these lines becomes visible, it means the target peptide is present in the sample. The technology can also easily be modified to detect multiple types of peptides re-leased by different types or stages of disease.
“This is a clever and inspired technology to develop new exogenous compounds that can detect clinical conditions with aberrantly high protease concentrations,” says Samuel Sia, an associate professor of biological engineering at Columbia University who was not involved in the research. “Extending this technology to detection by strip tests is a big leap forward in bringing its use to outpatient clinics and decen-tralized health settings.”
In tests in mice, the researchers were able to accurately identify colon tumors, as well as blood clots. Bhatia says these tests represent the first step toward a diagnostic device that could someday be useful in human patients.
“This is a new idea — to create an excreted biomarker instead of relying on what the body
gives you,” she says. “To prove this approach is really going to be a use-ful diagnostic, the next step is to test it in patient populations.”
Developing diagnostics To help make that happen, the
research team recently won a grant from MIT’s Deshpande Center for Technological Innovation to devel-op a business plan for a startup that could work on commercializing the technology and performing clinical trials.
Bhatia says the technology would likely first be applied to high-risk populations, such as peo-ple who have had cancer previous-ly, or had a family member with the disease. Eventually, she would like to see it used for early detection throughout developing nations.
Such technology might also prove useful in the United States, and other countries where more
advanced diagnostics are available, as a simple and inexpensive alternative to imaging. “I think it would be great to bring it back to this setting, where point-of-care, image-free cancer detec-tion, whether it’s in your home or in a pharmacy clinic, could really be transformative,” Bhatia says.
With the current version of the technology, patients would first receive an injection of the nanoparticles, then urinate onto the paper test strip. To make the process more convenient, the researchers are now working on a nanoparticle formulation that could be implanted under the skin for longer-term monitoring.
The team is also working to identify signa-tures of MMPs that could be exploited as bio-markers for other types of cancer, as well as for tumors that have metastasized.
The research was funded by a National Sci-ence Foundation Graduate Research Fellow-ship, a Mazumdar-Shaw International Oncology Fellowship, the Ruth L. Kirschstein National Research Service Award from the National Insti-tutes of Health, the Burroughs Wellcome Fund, the National Cancer Institute, and the Howard Hughes Medical Institute.
Reprinted with permission of MIT News (http://web.mit.edu/newsoffice/)http://web.mit.edu/newsoffice/2014/a-pa-per-diagnostic-for-cancer-0224.html
The paper test strips, which work similar to a pregnancy test, reveal the presence of proteins associated with cancer. They can also be designed to detect other dis-eases. PHOTO: BRYCE VICKMARK
www.ambihealthmd.weebly.com40
AmbiHealth M.D.
www.ambicaglobal.com | www.ambicare.net 41
Medical Digest

www.ambihealthmd.weebly.com42
AmbiHealth M.D.
“Despite numerous check-ups and diagnostic tests, his cancer was not detected until it was too late . . .” For thousands of Filipino families, this is a familiar statement regarding the nightmare of losing a loved one because of inaccurate and too late medical diagnosis.
Fortunately, a high-tech (yet af-fordable) solution is now available in the Philippines: “Molecular Diag-nostic” (MD) tests, a service offered by the partnership of Ambica Bio-technologies (www.ambicaphilippines.com) and the multi-billion-dollar global pharma giant, Reliance Life Sciences India (www.rellife.com).
MD tests are the most advanced and superior alternative to traditional serologic and pathologic laboratory tests which are not sensitive and spe-cific enough to detect the targeted anomalies.
The United States government’s National Cancer Institute provides a simplified explanation:
“Before molecular diagnostics, cli-nicians categorized cancer cells ac-cording to their pathology, that is, ac-cording to their appearance under a microscope.
“Borrowing from two new disci-plines, genomics and proteomics, mo-lecular diagnostics categorizes cancer using technology such as mass spec-trometry and gene chips. Genomics is the study of all the genes in a cell or organism, while proteomics is the study of all the proteins. Molecular di-agnostics determines how these genes and proteins are interacting in a cell. It focuses upon patterns--gene and pro-tein activity patterns--in different types of cancerous or precancerous cells. Molecular diagnostics uncovers these sets of changes and captures this in-formation as expression patterns. Also called ‘molecular signatures,’ these expression patterns are improving the clinicians’ ability to diagnose cancer. Soon all cancers may be diagnosed this way.”
Thus, while traditional lab tests rely
more on general diagnostic methods and modalities, MD tests analyze the specific and target-sensitive molecular structures. Examples would include genes, chromosomes and proteins of the blood and tissue samples. Conse-quently, MD test results are more spe-cific, more sensitive, and more accu-rate than traditional lab tests.
Not just cancerMore good news: MD tests are not
limited to diagnosing cancer conditions. It is an equally effective diagnostic tool against dengue, HIV/AIDS, hepatitis, tuberculosis, malaria, and many other diseases.
For couples, MD tests are even ca-pable, to a certain extent, of predicting and diagnosing infertility problems.
For pregnant women, through pre-natal diagnosis, MD tests can predict the probability that the fetus will be afflicted with Patau, Edward, Down or other congenital syndromes which have serious or even fatal conse-quences for the baby.
MD tests do not only provide early detection of cancer; they can also give highly reliable projections on the prob-ability that a presently healthy patient will develop cancer, thus providing these patients and their doctors with additional tools for preventive mea-sures to be undertaken.
Cord blood/tissue/stem cell bankingA related service to the MD test ser-vices is “cord blood banking,” “cord tis-sue banking,” and “stem cell banking,”
wherein blood and tissue from the baby’s umbilical cord are gathered at birth and cryopreserved (for many years) under strictly controlled labo-ratory conditions, for the purpose of having a ready and reliable source of stem cells which the baby – or an im-mediate nuclear relative – might need in the future to cure all kinds of diseas-es, such as different types of cancers, diabetes, arthritis, neurodegenerative disorders (Alzheimer’s, etc.).
Other benefitsOther key benefits of MD tests are:• Fast Turn-Around-Time (TAT) -- as
quick as four days from the receipt of the specimen sample by the lab -- un-like traditional lab tests which take sev-eral weeks for results to be available.
• Lab results fully verified and rec-ognized by all hospitals worldwide be-cause of accreditation by the College of American Pathologists (CAP), the highest and most rigorous international accreditation for medical laboratories.
• Maximum confidentiality (only the doctor and patient will know the re-sults).
• Affordable, As low as a few thou-sand pesos for some of the tests.
How to avail of MD testsFor patients who want to avail of
MD tests, all they have to do is request their attending physicians to facilitate the process. The patients, through their doctors, will then provide the blood or tissue samples needed by the specific tests requested, and their doctors will then coordinate with Ambica Biotech-nologies. As early as four days from the test date, the patients can then visit their doctors to know the results of their tests.
For doctors who want to avail of MD tests for their patients, they can contact Ambica International Cor-poration, Phones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615 Mobile: (0917) 554-6073; e-mail: [email protected]; Website: www.ambicaglo-bal.com | www.ambicare.net
by AmbiHealth Medical Digest Research Group
Molecular Diagnostic Tests cut risk of misdiagnosis;
Image courtesy of Photokanok at FreeDigitalPhotos.net
best early warning tool against diseases

www.ambicaglobal.com | www.ambicare.net 43
Medical Digest
FOR INQUIRIES, please contact AMBICA INTERNATIONAL CORPORATION, #9 Amsterdam Extension, Merville Park Subdivision, Paranaque City, PHILIPPINES 1700Phones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615; Mobile: (0917)554-6073; (0917)839-7430E-mail: [email protected]; Website: www.ambicaglobal.com
www.ambihealthmd.weebly.com44
AmbiHealth M.D.
FOR INQUIRIES, please contact AMBICA INTERNATIONAL CORPORATION, #9 Amsterdam Extension, Merville Park Subdivision, Paranaque City, PHILIPPINES 1700Phones: (632) 828-6617 to 18; 828-6542; Fax: (632) 828-6615Mobile: (0917)554-6073; (0917)839-7430E-mail: [email protected]; Website: www.ambicaglobal.com