
Acceptance and Commitment Therapy: Altering the Verbal Support for Experiential Avoidance
15
The Behavior Analyst 1994, 17, 289-303 No. 2 (Fall) Acceptance and Commitment Therapy: Altering the Verbal Support for Experiential Avoidance Steven C. Hayes and Kelly G. Wilson University of Nevada Acceptance and Commitment Therapy (ACT) is a behavior-analytically-based psychotherapy approach that attempts to undermine emotional avoidance and increase the capacity for behavior change. An overview of this approach is given, followed by several specific examples of the techniques used within ACT. In each instance the behavioral rationale of these techniques is described. A contemporary view of verbal relations provides the basis for new approaches to adult outpatient psychotherapy. Key words: rule-governed behavior, emotions, psychotherapy, Acceptance and Commitment Therapy, cognition In our previous article in this series (Hayes & Wilson, 1993), we described a relational frame conception of verbal events, and related this theory to an anal- ysis of rule-governed behavior. We de- veloped the implications of this view for several clinical topics, including mean- inglessness and existential angst, suicide, insight and self-knowledge, and the hu- man tendency toward emotional avoid- ance. Together, these lines of thinking create the outlines of a theory of psycho- pathology, in which many common forms of psychopathology are interpreted as be- ing the natural result of human verbal behavior. Over the last 15 years we have devel- oped a set of techniques designed to alter the way verbal relations function, based on this analysis. Taken together, these techniques form a behavior analytically derived psychotherapy approach: Accep- tance and Commitment Therapy or ACT (pronounced "act" not "A-C-T"). (As this approach was being developed, it was known as comprehensive distancing, but the therapy was renamed to avoid the undesirable and inaccurate dissociative connotations of that term.) ACT is one of a very few comprehensive verbal psy- Preparation of this manuscript was supported in part by Grant DA08634 from the National Institute on Drug Abuse. Correspondence concerning this article should be addressed to Steven C. Hayes, Department of Psy- chology, University of Nevada, Reno, NV 89557- 0062. chotherapies that have consciously been based on behavior-analytic thinking (R. Kohlenberg, Hayes, & Tsai, 1993; R. Kohlenberg, Tsai, & Dougher, 1993). In this article we will briefly summa- rize our approach. We will then explore two issues in greater detail, showing the kinds of things we do and providing a behavioral rationale. ACCEPTANCE AND COMMITMENT THERAPY The essential goal of ACT is to treat emotional avoidance, excessive literal re- sponse to cognitive content, and the in- ability to make and keep commitments to behavior change (Hayes, 1987; Hayes, Kohlenberg, & Melancon, 1989; Hayes & Melancon, 1989; Zettle & Hayes, 1986). Conventional Support for a Causal Role of Private Events Most psychotherapies deal, implicitly or explicitly, with the effect of client thoughts and feelings on overt behavior. In the usual view, certain undesirable emotions or thoughts are believed to cause undesirable patterns of living. On that basis these thoughts or emotions are targeted for change, control, or elimina- tion. Avoidance of a variety of private events can be understood as both a so- cially encouraged outcome and as a nat- ural outcome for verbal organisms as re- sult of bidirectional transformation of stimulus functions through equivalence and other derived relational responses 289
Transcript of Acceptance and Commitment Therapy: Altering the Verbal Support for Experiential Avoidance

The Behavior Analyst 1994, 17, 289-303 No. 2 (Fall)
Acceptance and Commitment Therapy:Altering the Verbal Support for Experiential Avoidance
Steven C. Hayes and Kelly G. WilsonUniversity of Nevada
Acceptance and Commitment Therapy (ACT) is a behavior-analytically-based psychotherapy approachthat attempts to undermine emotional avoidance and increase the capacity for behavior change. Anoverview of this approach is given, followed by several specific examples of the techniques used withinACT. In each instance the behavioral rationale of these techniques is described. A contemporary viewof verbal relations provides the basis for new approaches to adult outpatient psychotherapy.Key words: rule-governed behavior, emotions, psychotherapy, Acceptance and Commitment Therapy,
cognition
In our previous article in this series(Hayes & Wilson, 1993), we described arelational frame conception of verbalevents, and related this theory to an anal-ysis of rule-governed behavior. We de-veloped the implications of this view forseveral clinical topics, including mean-inglessness and existential angst, suicide,insight and self-knowledge, and the hu-man tendency toward emotional avoid-ance. Together, these lines of thinkingcreate the outlines ofa theory of psycho-pathology, in which many common formsofpsychopathology are interpreted as be-ing the natural result of human verbalbehavior.Over the last 15 years we have devel-
oped a set oftechniques designed to alterthe way verbal relations function, basedon this analysis. Taken together, thesetechniques form a behavior analyticallyderived psychotherapy approach: Accep-tance and Commitment Therapy orACT(pronounced "act" not "A-C-T"). (As thisapproach was being developed, it wasknown as comprehensive distancing, butthe therapy was renamed to avoid theundesirable and inaccurate dissociativeconnotations of that term.) ACT is oneof a very few comprehensive verbal psy-
Preparation of this manuscript was supported inpart by Grant DA08634 from the National Instituteon Drug Abuse.
Correspondence concerning this article should beaddressed to Steven C. Hayes, Department of Psy-chology, University of Nevada, Reno, NV 89557-0062.
chotherapies that have consciously beenbased on behavior-analytic thinking (R.Kohlenberg, Hayes, & Tsai, 1993; R.Kohlenberg, Tsai, & Dougher, 1993).
In this article we will briefly summa-rize our approach. We will then exploretwo issues in greater detail, showing thekinds of things we do and providing abehavioral rationale.
ACCEPTANCE ANDCOMMITMENT THERAPY
The essential goal of ACT is to treatemotional avoidance, excessive literal re-sponse to cognitive content, and the in-ability to make and keep commitmentsto behavior change (Hayes, 1987; Hayes,Kohlenberg, & Melancon, 1989; Hayes& Melancon, 1989; Zettle& Hayes, 1986).
Conventional Support for a CausalRole ofPrivate EventsMost psychotherapies deal, implicitly
or explicitly, with the effect of clientthoughts and feelings on overt behavior.In the usual view, certain undesirableemotions or thoughts are believed tocause undesirable patterns of living. Onthat basis these thoughts or emotions aretargeted for change, control, or elimina-tion. Avoidance of a variety of privateevents can be understood as both a so-cially encouraged outcome and as a nat-ural outcome for verbal organisms as re-sult of bidirectional transformation ofstimulus functions through equivalenceand other derived relational responses
289
290 STEVEN C. HAYES & KELLY G. WILSON
(see Hayes & Wilson, 1993, for a morecomplete discussion). Rather than tryingto change the form or frequency of pri-vate events, ACT attempts to alter theirpsychological functions by altering thesocial/verbal context in which privateevents occur.According to an ACT perspective, the
controlling effects of private events overovert behavior are supported by the so-cial/verbal context that supports the lit-erality oflanguage, and the resultant needto alter the form of private events. Sup-pose a panic-disordered person thinks "IfI get too anxious I will go crazy." Givena context (both historical and situational)that supports the domination of derivedstimulus functions based on such rela-tional responses over other sources ofbe-havior, the private event called "anxi-ety" may occasion a variety ofdisruptivebehavior, such as running out of the sit-uation "in order to reduce the anxiety"and thus avoid going crazy. From an ACTperspective, however, the behavior reg-ulatory function of anxiety and thoughtsabout anxiety is not mechanical or direct.When the context supporting excessiveliterality is changed, the link between pri-vate events and overt action can be re-duced, even in the presence of suchthoughts, and attention can then shiftfrom emotional or cognitive manipula-tion to the more direct consequences ofovert action. In short, the issue becomesdoing what works, particularly in the longterm, rather than feeling, thinking, re-membering, or sensing only certain thingsin order to do what works.At least three aspects of the normal
social/verbal context for human actionare thought to contribute to the estab-lishment of undesirable control by pri-vate behavior: (a) the impact of literalmeaning and evaluation, (b) the accep-tance of verbal reason giving as a validexplanation for individual behavior, and(c) social training that cognitive and emo-tional control can, and should, beachieved as a means to successful living.
Literality. Words enter into stimulusequivalence and other derived relations(Hayes& Hayes, 1989; Sidman & Tailby,1982) with verbal and nonverbal events.
Functions given to one member of a re-lational network will transfer to others interms ofthe underlying relation. Such ef-fects have been repeatedly documentedin the equivalence literature (Hayes,Brownstein, Devany, Kohlenberg, &Shelby, 1987; Hayes, Kohlenberg, &Hayes, 1991; B. Kohlenberg, Hayes, &Hayes, 1991; Wulfert & Hayes, 1988). Incommon language, words mean the thingsto which they relate, and many functionsthat would adhere to the situation be-come present with regard to the words.The verbal community arbitrarily es-
tablishes the specific relation betweenwords and other events. These conven-tions are what we mean by "the contextof literality." In many situations, thisability to respond to verbal formulationsin some ways as if one were respondingto the actual contingencies described isextremely adaptive. "Don't drink that-it's poison," for example, can establish abehavioral topography that would be dif-ficult to acquire through direct contactwith the contingencies described. Otherdescriptions are less clearly adaptive and,in some instances, may be psychologi-cally destructive, such as "Don't feel X,"or "Don't remember X." The problemis that in some contexts derived stimulusfunctions can dominate over other, moredirect forms ofbehavioral influence. ACTseeks to undermine literality, such thatliteral meaning is no longer the necessarybasis for responding-rather, it is thepsychological context for responding onlyon the basis of experienced workability.In other words, we seek to limit rationalresponding to situations in which ratio-nality is helpful as a basis for responding.To do this, however, derived stimulusfunctions must come more into balancewith those acquired directly. To give aslightly simplified analysis of the exam-ple ofthe panic-disordered person we de-scribed earlier, the impact of "if I get tooanxious I will go crazy" is based on atleast three kinds of verbal relations: (a)a strong equivalence relation betweenvarious bodily sensations and behavioralpredispositions and the term anxiety, (b)a similarly tight equivalence class be-tween highly undesirable and socially
ACCEPTANCE AND COMMITMENT THERAPY 291
condemned behavior in others and "go-ing crazy," and (c) the ability to apply an"if... then" relation as an operant classbased on cues to do so rather than ondirect experience with the sequential re-lation. The panic-disordered person's di-rect history is almost never that anxietyitself leads to going crazy. Indeed, thedirect history is usually more that at-tempting to avoid anxiety creates anxiety(in part, because such avoidance para-doxically supports the if... then relationbetween anxiety and aversive ends, andanxiety is a natural response to imminentaversive stimulation). The dominationofderived over direct stimulus functionsis based, we argue, on the domination ofcontextual support for literal (i.e., highlyrelational) responding.Reason giving. A second source of the
relation between private events and overtbehavior is reason giving. Thoughts andfeelings are commonly pointed to as val-id and sensible causes of overt behav-ior-an explanation for behavior that iswell supported by the culture. A personsaying "I was too anxious to stay at themall" will certainly be thought to havesaid something reasonable and under-standable. He or she may even gamersympathy or reassurance for this for-mulation. "I have no idea why I left" willprobably receive a much less positive re-sponse. In this way, the verbal commu-nity establishes discriminative and mo-tivational functions for a variety ofprivate events that are conventionallypart of reasons and explanations. Theverbal community that reinforces (or doesnot punish) behavior because a reasonpoints to a private event as a cause forthat behavior, is also reinforcing two dis-tinct things. First, it reinforces the be-havior regulatory function of the privateevent itself. Second, it reinforces the oc-currence of the private event that is ac-tually related to the behavior that thisevent supposedly controls. For example,if one can successfully avoid a difficultjob interview "because I am just too de-pressed to go," then (a) feeling depressedis more likely to lead to the avoidance ofdifficult tasks, and (b) depressed feelingsare more likely when such tasks occur.
Most of these functions are conven-tional, however, rather than necessary.Depressed feelings need not necessarilylead to behavior change, and under otherconditions they may not. One such con-dition may be the weakening of supportby the verbal community for emotionalor other experiential reasons. The social/verbal community oftherapist and clientcreated in an ACT session gives little orno support for reason giving ofthis kind.
Training in experiential control. Theprocess of emotional and cognitive reg-ulation as a means of behavior controlbegins quite early. Even babies are oftenevaluated according to how little they ex-press negative affective states (e.g., "She'ssuch a good baby, she never cries"). Chil-dren are told, regularly and often, thatthey can and ought to control negativeaffective states. Punishment and rein-forcement are frequently doled out ac-cording to the ability to control and sup-press at least the outward signs ofaversiveemotional states ("Stop crying or I'll giveyou something to cry about"). Siblingsand schoolmates support the ongoingpurposeful control of emotion. State-ments such as "Don't be a baby" or "Justforget about X" will be backed up by avariety of socially mediated conse-quences (e.g., being hit, being shamed,etc.). Clients often arrive in therapy fo-cused on this agenda: "I can't control mydepression" or "I'm too anxious." Evenin the therapeutic milieu, the therapistmay overtly tell the client to emote, ex-press, and report negative emotions, butin subtle ways may punish the client'snegatively evaluated affect, thoughts, ormemories. Furthermore, the therapeuticagenda itselfmay imply as much, becauseit is common to accept as a goal of ther-apy the reduction or alteration of emo-tional and cognitive events. Given thesecontingencies, private events gain morebehavior regulatory power, because theyoccasion such determined efforts to altertheir form or frequency of occurrence.
SYNOPSIS OF ACTClients naturally come into therapy
with the intent to control what they view
292 STEVEN C. HAYES & KELLY G. WILSON
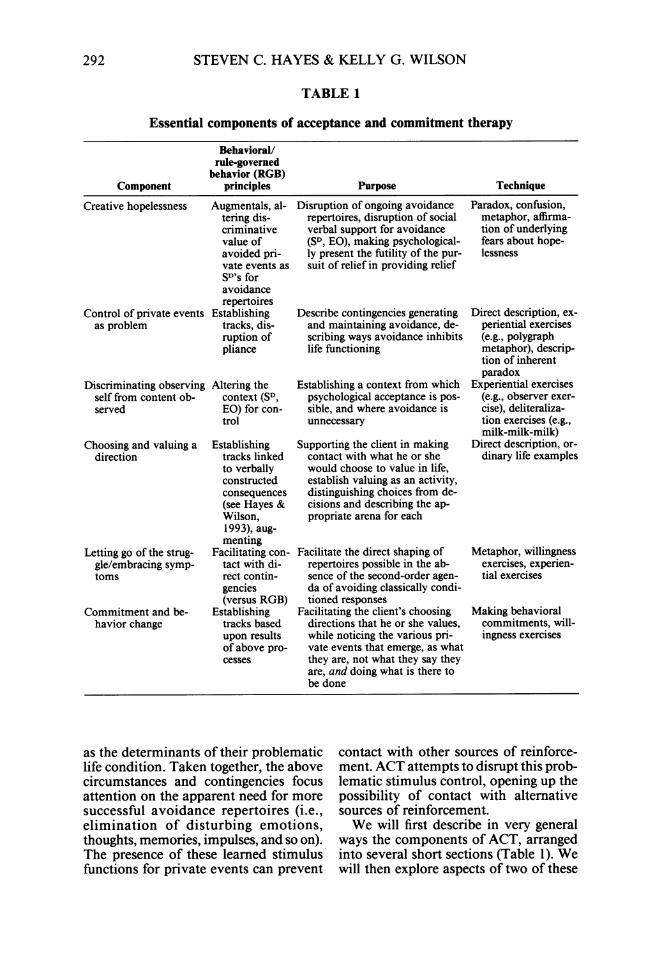
TABLE 1
Essential components of acceptance and commitment therapy
Behavioral/rule-governed
behavior (RGB)Component principles Purpose Technique
Creative hopelessness Augmentals, al- Disruption of ongoing avoidance Paradox, confusion,tering dis- repertoires, disruption of social metaphor, affirma-criminative verbal support for avoidance tion of underlyingvalue of (SD, EO), making psychological- fears about hope-avoided pri- ly present the futility of the pur- lessnessvate events as suit of relief in providing reliefSD's foravoidancerepertoires
Control of private events Establishing Describe contingencies generating Direct description, ex-as problem tracks, dis- and maintaining avoidance, de- periential exercises
ruption of scribing ways avoidance inhibits (e.g., polygraphpliance life functioning metaphor), descrip-
tion of inherentparadox
Discriminating observing Altering the Establishing a context from which Experiential exercisesself from content ob- context (SD, psychological acceptance is pos- (e.g., observer exer-served EO) for con- sible, and where avoidance is cise), deliteraliza-
trol unnecessary tion exercises (e.g.,milk-milk-milk)
Choosing and valuing a Establishing Supporting the client in making Direct description, or-direction tracks linked contact with what he or she dinary life examples
to verbally would choose to value in life,constructed establish valuing as an activity,consequences distinguishing choices from de-(see Hayes & cisions and describing the ap-Wilson, propriate arena for each1993), aug-menting
Letting go of the strug- Facilitating con- Facilitate the direct shaping of Metaphor, willingnessgle/embracing symp- tact with di- repertoires possible in the ab- exercises, experien-toms rect contin- sence of the second-order agen- tial exercises
gencies da of avoiding classically condi-(versus RGB) tioned responses
Commitment and be- Establishing Facilitating the client's choosing Making behavioralhavior change tracks based directions that he or she values, commitments, will-
upon results while noticing the various pri- ingness exercisesof above pro- vate events that emerge, as whatcesses they are, not what they say they
are, and doing what is there tobe done
as the determinants of their problematiclife condition. Taken together, the abovecircumstances and contingencies focusattention on the apparent need for moresuccessful avoidance repertoires (i.e.,elimination of disturbing emotions,thoughts, memories, impulses, and so on).The presence of these learned stimulusfunctions for private events can prevent
contact with other sources of reinforce-ment. ACT attempts to disrupt this prob-lematic stimulus control, opening up thepossibility of contact with alternativesources of reinforcement.We will first describe in very general
ways the components of ACT, arrangedinto several short sections (Table 1). Wewill then explore aspects of two of these

ACCEPTANCE AND COMMITMENT THERAPY 293
components in detail, so that the readercan get a better sense of what actuallygoes on in ACT and the reasons for it.
Creative HopelessnessIn the first component of ACT, the
therapist attempts to establish a condi-tion of "creative hopelessness," in whichformer "solutions" begin to be seen bythe client as problems in themselves. Un-der such conditions, the client is moreopen to entirely new courses of action.When all "solutions" are no longer so-lutions, the client may view the situationas hopeless, but it is a creative conditionbecause now fundamentally new ap-proaches are possible.
Because the client's solutions are near-ly all both logical and reasonable, thetherapist must behave in ways that areneither. The purpose ofthis phase ofACTis to confront the social/verbal supportsfor the client's means-ends formulations(based on these contexts of literality, rea-son giving, and experiential control). Allofthe client's efforts at emotional controlare explored in detail and in each casethe client is asked if, in their experience,this approach truly solved the problem.To some degree, the answer must be "no,"or the client would not be in therapy. Thetherapist emphasizes the great exertionand minimal benefit of efforts to controlemotions, thoughts, sensations, memo-ries, and other private events. Becausethe client has already attempted logical,commonsense solutions, some changebeyond ordinary verbal logic is clearlyneeded. Clients often have an underlyingfear that the situation is hopeless. Thissense is brought out and affirmed. Withinthe context in which the client has beenworking, the therapist agrees that the sit-uation is hopeless. The client's sense ofbeing stuck is also brought out and af-firmed.
In behavioral terms, "relief' is a ver-bally constructed consequence for theclient's avoidance repertoires (see Hayes& Wilson, 1993, for a discussion of ver-bal vs. nonverbal purpose). The purposeof this phase of ACT is motivative. Weseek to deestablish "relief' as a valued
verbal consequence and thereby increasethe probability that other repertoiresmight emerge, through which other con-sequences might be contacted.The following is an actual example from
a session early in ACT. It has been slight-ly edited for clarity and to protect con-fidentiality:
Therapist: Right. That doesn't make sense. It'snot logical-it's not like that anywhere else in yourlife. You've worked hard. If you're building some-thing, you work on it, it gets better.
Client: Uh hum-it doesn't make sense-I'vethought about it a lot, a lot of long hours just ofhard thinking just about this.
Therapist: We have to consider the possibilitythat what is the most obvious thing to you, the mostobvious thing, is actually not so; the most clear thingyou have to do in terms ofmoving ahead, that that'sactually the problem, not the solution, it's the prob-lem.
Client: My mind stops working here.Therapist: Good, good-actually that may be
helpful. Because again, ifwhat I'm saying right nowmakes sense, you'd say "oh yeah, that's right," but,if it makes sense that's probably not it. Becauseyou've already done everything that makes sense.
Confusion is used deliberately to preventthe client from intellectualizing and com-partmentalizing his or her dilemmas intothe same solutions that have alreadyfailed. In addition to these paradoxicalinterventions, many interventions inACT are nonlinear and metaphorical.This use ofmetaphor fits fairly well withother, more humanistic uses ofmetaphorin the clinical setting (see McCurry &Hayes, 1993, for a review), but it differsin that specific ACT-relevant themes arealways at the focus of such metaphoricaltalk.
Trying to Control PrivateEvents as the Problem
In the second component of ACT,therapists target emotional and cognitivecontrol as the core obstacle preventingsuccessful solution ofthe problems in liv-ing faced by the client. As discussedabove, by the time the client comes totherapy, he or she has been well trainedto view control of private events as im-portant. At this stage oftherapy, the ther-apist gives examples ofways in which weare socialized to exercise such control.Among those emphasized are:

294 STEVEN C. HAYES & KELLY G. WILSON
1. We experience direct instruction tocontrol emotion: "stop that crying," "justforget about it," "put it behind you."
2. Significant persons have modeledapparent control of thoughts, emotions,and the like. Adults are often adept athiding their emotional responses fromchildren. From the perspective of thechild, emotional responses appear to beabsent: "See, daddy isn't afraid."
3. There is likely to be generalizationfrom situations in which children are en-couraged and are successful at controllingenvironmental events. A repertoire ofverbally governed control efforts worksvery well in dealing with the world, butit works horribly in dealing with one'sown history or one's own private events.
4. Emotional control may actually beeffective in limited or temporary ways.Distraction, for example, may be an ef-fective strategy for the management ofaversive emotional responding when thesource ofthat response is temporary (i.e.,an impending dental appointment).However, if the source of the response ispersistent or permanent, such as an incesthistory, these strategies become less ten-able both because the temporary effectsof distraction wear off, setting the stagefor another round of distraction efforts,and because such deliberate avoidanceactually increases the behavior regula-tory function and thus the psychologicalimportance of the avoided event.
Clients are encouraged to examine theirown experience to see if the rule thatworks in the world of objects ("If youdon't like something, figure out how toget rid of it and then get rid of it") hasworked in the world of private events.We suggest that a more accurate rule forthe arena ofprivate events is "Ifyou aren'twilling to have it, then you've got it."Again, metaphor and paradox are usedto highlight this dilemma (e.g., see thepolygraph metaphor below).The therapist, in describing the client's
experience, elaborates tracks that the cli-ent is following, along with the actuallycontacted, rather than verbally con-structed, consequences offollowing thosetracks. In addition, the therapist attemptsto undermine the client's pliance with so-
cial sanctions to avoid "unpleasant" pri-vate events.
Establishing Selfas ContextRather Than ContentThe third component ofACT helps the
client to discriminate the person he orshe calls "I," and the problem behaviorthat the client wants to eliminate. Thistopic is behaviorally difficult, and spacelimitations preclude a detailed discussion(see Hayes, 1984, 1987). The essentialidea is that verbal training leads to a formof self-awareness that consists of the lo-cus ofverbal events, rather than the con-tent ofsuch events. That is, humans learnnot only to observe their own actions (oneform of self-awareness) but also to do sofrom a consistent locus or point ofview-what is usually called "I."ACT uses various experiential exercis-
es and metaphors to help this sense of"I" come into focus. Most people canexperientially recognize the essentialcontinuity between the "I"s referred toin the statements "I went to first grade"and "I am in therapy now," even ifmanydecades have passed from one to the oth-er and virtually everything in the realmof content has changed.Other techniques are used at this point
in ACT to begin to separate thoughts,emotions, and other private events fromthe person having them. For example, weask clients at least temporarily to adopta particular verbal style in therapy inwhich the type of verbal event is named,rather than simply stating the content ofthat event. For example, clients are taughtto say "I'm having the thought that I can'tgo to the mall" (as opposed to simplystating, "I can't go to the mall"), or "I'mhaving the evaluation that I'm a bad per-son" (as opposed to "I'm a bad person").Clients have often attempted to separatethemselves from negatively evaluatedthoughts and emotions. Here, however,the separation is to increase contact withthe private event rather than to decreaseit-which has been the client's agenda.A commonly used ACT metaphor may
help to clarify this point. In the meta-phor, the client's private events (both

ACCEPTANCE AND COMMITMENT THERAPY 295
negatively and positively evaluated) aresaid to be like pieces on a chess board.Within this metaphor, the counterpart for"self as context" is not the chess pieces(the content) but the board itself. If theclient is observing events "from piecelevel," certain pieces on the board maybe obscured or altogether invisible de-pending on their placement on the board.The board, however, is fully in contactwith all of the pieces. It is also worthnoting that pieces on the board maythreaten one another: A white piece suchas "I'll get through this" may be threat-ened by a large black queen shouting "Notin this lifetime!" The board, however,contains and is fully in contact with, butnot threatened by, any piece, be it posi-tive or negative. Such metaphors areaimed at altering the verbally establisheddiscriminative and motivative context inwhich control of private events is nec-essary.
Choosing and Valuing a DirectionIn the fourth component of ACT, the
therapist supports the client in establishingtracks linked to verbally constructed con-sequences. Often the goals that a client hasfor therapy emerge in the context of ex-ploring his or her avoidance repertoires.The client may come to therapy wantingto be rid ofdepression or anxiety, and thatwish will often be explicitly linked to someoutcome he or she would choose-if onlythese problematic thoughts and feelingswould abate. So an agoraphobic clientmight say that he or she needs to get ridof panic so that he or she can really moveforward in a career. Or the incest survivormight say that the memories need to stopso that he or she can develop a truly in-timate relationship with a spouse. At othertimes, we may see clients for whom beingpsychologically present to what they val-ue-and believe that they cannot have-is so aversive that they might pronounceloudly that they want the opposite. It hasbeen our experience in the application ofthis therapy, however, that as avoidancerepertoires subside, valued outcomesemerge.ACT therapists make several distinc-
tions as they discuss the issue of valuing.Among these is the distinction betweenvaluing as a feeling and valuing as anactivity. These two are often thoroughlyconnected for clients. The verbal supportfor this connection between private eventsrelated to values and active valuing isattacked. The example of valuing a lov-ing relationship with one's spouse pro-vides an instructive example. One's feel-ings of love may wax and wane acrosstime and situation. To behave lovingly(i.e., respectfully, thoughtfully, etc.) onlywhen one had feelings of love, and tobehave in opposite ways when the op-posite feelings emerged, would be likelyto have problematic effects on a mar-riage. We ask our clients "Could you be-have lovingly, even when you were notfeeling loving?" We are careful here toassure the client that we are not talkingabout faking love-duplicity wouldhardly characterize loving behavior.What we are attempting to highlight isthe client's ability to control some thingsand not others, and to get the client toexercise control in the areas where con-trol is effective.The ACT therapist focuses on valuing
and choosing as activities, not becausethe feeling aspect of a client's valuing isunimportant, but because efforts at con-trol are effective in the domain of activ-ities, whereas they are problematic in theareas of thoughts and feelings. In tech-nical terms, valuing as an activity is op-erant behavior, whereas valuing as a feel-ing is more likely to be respondent. Wefurther characterize valuing and choosingas activities that are unavoidable. Amongthe techniques used are questions such as"What do you want your life to standfor?" or "Ifyour epitaph were to be writ-ten, based upon what you are doing to-day, what would it read?" Clients willseldom endorse an epitaph such as "Shededicated her life to avoiding anxiety."We often speak ofthis active componentof valuing as "valuing with your feet."We ask them, "In the direction of whatvalued end are your feet currently takingyou?" Sometimes clients try to avoidchoosing a direction, and at those timeswe point out that choosing not to choose

296 STEVEN C. HAYES & KELLY G. WILSON
is also a choice -in the very direct senseof a selection among behavioral alter-natives. In such cases, the epitaph mightread "He dedicated his life to not choos-ing."
Letting Go ofthe Struggle/EmbracingSymptoms
In the fifth component of ACT, weencourage clients to begin deliberatelyexperiencing thoughts, feelings, bodilysensations, memories, or behavioral pre-dispositions that, if taken literally, mustbe avoided. There are many times whenself-rules point to ineffective actions.When we encourage clients to give up thestruggle with experiential control, we arenot asking them to "grin and bear it," orto "tough it out" until their symptomscan be endured. Rather, we are askingthe client to lean forward into the "symp-toms." We encourage them not only tostop struggling but to embrace the verythings that they most dread. This trans-forms the functional meaning of theseevents, without changing their form.When a private event no longer occasionsavoidance, it begins to lose its impor-tance. The purpose of this component ofACT is to help the client make contactwith the shaping impact of directly ex-perienced contingencies present when thesecond-order agenda of avoiding certainprivate events is absent.Many techniques are used in this pro-
cess, especially "willingness exercises."Avoided private events are brought intothe therapy room (via imagery or exer-cises) and disassembled into componentpieces: bodily sensations, thoughts, be-havioral predispositions, memories, andso on. In all cases, the goal is not to gaincontrol over them but to experience themwithout any attempt to modify or escapethem.
Commitment and Behavior ChangeThe sixth goal of ACT is to aid the
client in making commitments to action.All forms of psychopathology are asso-ciated with ineffective styles ofliving andbehaving. Now that one's history and theresulting elicited thoughts and feelings
associated with that history need not bechanged first, the focus can be on theclient's chosen behavior change. A clientat this point in ACT therapy has lost so-cially sanctioned "reasonable" problem-atic private events as causes for a failureto follow through. Nor will any attemptbe made to punish recalcitrant clients orto trick them into keeping their com-mitments. Rather, a verbal environmenthas been created in therapy that allowsno logical escape -the central issue is en-tirely what works rather than what is rea-sonable even ifit doesn't work. ACT triesto establish a discrimination between self-rules that cannot be followed effectively(i.e., rules of emotional avoidance) andself-rules that can be followed effectively,and if followed will lead to positive con-sequences (e.g., commitments to behav-ior change). Promises usually work bestwhen they are kept. This contingency isdirect and natural, rather than imposedby the therapist.
The Therapeutic RelationshipThe therapeutic relationship is crucial
to ACT for several reasons. First, ther-apists cannot readily train what they donot model. We cannot ask clients to openthemselves up to experiencing deliteral-ized thoughts and feelings undefendedwithout doing so as therapists. Our cli-ents come to us with seemingly insur-mountable difficulties. They are in a greatdeal of pain. No one open to the realityofhuman misery can be in a therapy roomwithout often feeling sad or anxious. If,from the opening moments of therapy,the therapist can be present to the client'sburden and not balk or turn away, theclient is already contacting the processand purpose of ACT. This openness onthe part of the therapist establishes apowerful and intimate therapeutic alli-ance.Second, we consider that given the
contingencies that established and main-tain emotional avoidance, careful atten-tion to the therapeutic relationship isnecessary to the goals ofACT. Emotionalavoidance is, in many respects, a socialact. The historical context in which emo-

ACCEPTANCE AND COMMITMENT THERAPY 297
tional avoidance is established begins inearly childhood in the context of intense-ly intimate and dependent interpersonalrelationships. Behaviorally speaking,treating behavior in the actual context inwhich it was learned and continues tooccur improves generalization to rele-vant nontherapy contexts. In a numberof respects, an intimate therapeutic re-lationship may mirror the context inwhich avoidance repertoires were estab-lished in the first place. Many of our cli-ents indicate difficulties in their inter-personal relationships, especially intimateones. Thus an intimate therapeutic re-lationship may bring to bear importantcontextual variables that have been as-sociated with problematic functioning.
Finally, ACT attempts to disrupt prob-lematic verbal control in its paradoxicaland metaphorical attacks on the contextofliterality. Ifproblematic verbal controlis interfering with a client's probabilityof making contact with important non-verbal contingencies, then an attack onthis control, if successful, makes the cli-ent more susceptible to nonverbal con-tingencies in the therapeutic interaction.Thus, emotional avoidance on the partof the therapist can be extremely prob-lematic because it would provide a dis-torted and unhealthy learning experienceto a person newly opened up to direct,contingent influences on behavior.
EXAMPLES OF SPECIFIC ACTTECHNIQUES
The ACT protocol is a book-lengthdocument (Hayes, Strosahl, & Wilson, inpress), comprising over a hundred spe-cific procedures organized around thesekey principles. Thus, it is not possible todescribe ACT in detail here. What fol-lows, however, is a sample of a few spe-cific metaphors, exercises, and other pro-cedures. In each case we will describewhat an ACT therapist does or says, andwill then attempt briefly to analyze thismaterial behaviorally.
The Polygraph MetaphorThe following is an example of a spe-
cific metaphor that is used early in ACT.
It is written much as an ACT therapistmight deliver it:Suppose I had you hooked up to the best polygraphmachine that's ever been built. This is a perfectmachine, the most sensitive ever made. When youare all wired up to it there is no way you can bearoused or anxious without the machine knowingit. You have a very simple task here: All you haveto do is stay relaxed. Ifyou get the least bit anxious,I will know it. But I know you want to try hard andI want to give you an incentive to do so, so I alsohave a .44 magnum that I'll hold to your head. Ifyou just stay relaxed, I won't blow your brains out,but if you get nervous (and I'll know it becauseyou're wired up to this perfect machine), I'm goingto have to kill you. So, just relax! What do youthink would happen? Guess what you'd get? Bamm!The tiniest bit ofanxiety would be terrifying. You'dbe going "Oh, my God! I'm getting anxious! Hereit comes!" BAMM! How could it work otherwise?
The purpose of this metaphor is to ex-pose the client to the actual contingenciesoperating when emotional control is cru-cial. Metaphors are useful because theyare forms of verbal activity that are notrule-like, and thus are unlikely to initiatepliance to please the therapist, but in-stead present pictures or stories that aremore like a verbal approximation of ex-perienced contingencies. In the abovemetaphor, almost everyone can imme-diately see, in a commonsense way, thefutility of the situation. The ACT ther-apist may bring this out in high relief,once the client has already contacted thecentral point:Now, you have the perfect polygraph machine al-ready hooked up to you: It's you own nervous sys-tem. It is better than any machine humans haveever made. You can't really feel something and nothave your nervous system in contact with it, almostby definition. And you've got something pointed atyou that is more powerful and more threateningthan any gun-your own self-esteem, self-worth,and the workability ofyour life. So you actually arein a situation very much like this. You're holdingthe gun to your head and saying, "Relax!" So guesswhat you get?
DeliteralizationThe essence of deliteralization is the
weakening of the response functions ofverbal events that depend upon a strongrelational network, and the weakening ofthe transfer of psychological functionsthrough this relational network. If a lan-guage history is a method of training or

298 STEVEN C. HAYES & KELLY G. WILSON
(one might say) creating a mind, then de-literalization is a method of blowing amind or opening a mind.No amount of deliteralization will
eliminate derived relations, nor is thisdesirable. To make this point, ACT ther-apists challenge clients to try to hear whatis being said in therapy in the same waythey would hear words spoken in an un-known foreign language. They can't. Thesame could be asked of our readers atthis moment: Kindly read this sentencewe are now writing, but as you read eachword in this sentence we challenge youto see each word in the same way that aperson sees words in a totally foreign lan-guage. Read this sentence but have noidea ofwhat you are reading, or even thatthere are words. This does not occur, andno ACT client has yet met the challenge.An inherent difference exists between"this is a sentence" and "ouwnm aoi polUslhk." Once a relational repertoire is ac-quired and applied to the conventionalstimuli within a language community,these stimuli are-to a degree -mean-ingful by virtue of the arbitrarily appli-cable relations they sustain.
Deliteralization has the goal of weak-ening-not eliminating-the relationalresponse such that other response formscan coexist with verbal forms. The fol-lowing exercise can begin to make thepoint. It was first used by Titchener todemonstrate his "context theory ofmeaning." It is presented in transcriptform to show how it is used in actualsessions.The "Milk, Milk, Milk" ExerciseTherapist: Let's do a little exercise. I'm going to
ask you to say a word. Then you tell me what comesto mind. I want you to say the word, "Milk." Sayit once.
Client: Milk.Therapist: Good. Now what came to mind when
you said that?Client: I have milk at home in the refrigerator.Therapist: OK. What else. What shows up when
we say "milk?"Client: I picture it.Therapist: Good. What else?Client: I can taste it. Sort of.Therapist: Exactly. And can you feel what it might
feel like to drink a glass? Cold. Creamy. Coats yourmouth. Goes "glug, glug" as you drink it. Right?
Client: Sure.Therapist: OK, so let's see if this fits. What shot
through your mind were things about actual milkand your experience with milk. All that happenedwas that we made a strange sound, and lots ofthesethings showed up. Notice that there isn't any milkin this room. None at all. Yet milk was in the roompsychologically. You and I were seeing it, tastingit, feeling it-yet only the word was actually here.Now, here is the little exercise, if you're willing totry it. The exercise is a little silly, and so you mightfeel a little embarrassed doing it, but I am going todo the exercise with you so we can be silly together.What I am asking you to do is to say the word"milk," out loud, rapidly, over and over again andthen notice what happens. Are you willing to tryit?
Client: I guess so.Therapist: OK. Let's do it. Say "milk" over and
over again.[As the client does so the ACT therapist does too,
periodically interjecting things like: "As fast as youcan go until I tell you to stop. Faster! Keep going!Faster!" or "Louder! Keep it up." Between theseinterjections, the therapist also is repeatedly andloudly saying the word. This continues for at leasttwo or three minutes.]
Therapist: OK, now stop. Did you notice whathappened to the psychological aspects of milk thatwere here a few minutes ago? What happened toactual milk?
Client: After about 40 times it disappeared. AllI could hearwas the sound. It sounded very strange-in fact, I had a funny feeling that I didn't even knowwhat words I was saying for a few moments. Itsounded more like a bird making a sound than aword.
Therapist: Right. The creamy, cold, gluggy stuffjust goes away. The first time you said it, it was asif milk were actually here, in the room. But all thatreally happened was that you said a word. The firsttime you said it, it was really meaning-full, it wasalmost solid. But when you said it again and againand again, you began to lose that meaning and thewords began to also be just a sound.
Client: I see that, but I don't quite see your point.Therapist: Well, when you say things to yourself
in addition to any meaning behind those words isn'tit also true that these words are just words? Thewords are just smoke. There isn't anything solid inthem. How is "milk" any different from "I'm bad"?
What we are doing in ACT is traininghumans to weaken derived relations, andto suspend the "sense-making" effort instrategically important areas. This weak-ening is what we mean by deliteraliza-tion. Literality is an automatic process inwhich the world has fimctions that emergefrom derived stimulus relations. The"milk, milk, milk" exercise creates a con-text in which sense making is not appli-cable. After 50 or 100 times of sayingsomething, the next time the word is said,nothing is added by operating on the ba-

ACCEPTANCE AND COMMITMENT THERAPY 299
sis of a derived relation, and the directfunctions ofthe word (e.g., auditory func-tions) begin to dominate. This exerciseopens up a truth: In addition to any ver-bal meaning a word may have, it is alsojust a sound. Just as there is no reasonto avoid sounds, there is no necessaryreason to avoid even the most negativewords, when they are considered to bewords.
Language ConventionsMany language conventions are adopt-
ed in ACT. The purpose of these con-ventions is to disentangle the client fromthe conventional emotional control agen-da built into normal locution. A goodexample is the use of the word "but."This word commonly carries with it animplicit statement about the organiza-tion ofpsychological events. Consider thestatement, "I want to go, but I am anx-ious." This simple statement carries adeep message about the role of feelingsin human action. Considered literally, thestatement says that although wanting togo would normally lead to going, anxietycontradicts the effect of wanting to go.Going cannot occur with anxiety.The etymology of the word "but" re-
veals this dynamic quite clearly. Accord-ing to the Oxford English Dictionary"but" is from the Old English "be-utan"meaning "on the outside, without." InMiddle English this became "bouten" andwas gradually phonetically weakened tobuten, bute, and thus "but." The Old En-glish word "be-'utan" is a combination of"be" (meaning something quite similarto the modem word "be") and "'utan"which is a form of "(ut"-an early formof our modem word "out." Etymologi-cally, "but" means "Be out." It is a callfor whatever follows the word to "goaway" or else threaten whatever precedesthe word. In other words, "but" is a fight-ing term. It says that two reactions thatdo exist cannot coexist and still be as-sociated with effective action. One or theother must go. This is a conventionalagenda that is directly contradictory tothe ACT perspective and more generallyto a behavioral view ofthe role ofprivateevents in behavioral regulation.
Here is a language convention drawnfrom the ACT protocol that we call "Get-ting Off Our Buts":
There is another verbal convention I'd like us toadopt in here. This is one that we can use through-out our time together. It has to do with our use ofthe word "but." This is a word that draws us intothe struggle with our thoughts and feelings becauseit is so commonly associated with explaining be-havior on the basis of private events and then pit-ting one set ofprivate events against another. "But"literally means that what follows the word contra-dicts what went before the word. It originally camefrom the words be out. When we use it we often say"this private event be out that private event. It'sliterally a call to fight, so it is no wonder it pulls usup into the piece level-into the war zone. [Noteto readers: this phrase "piece level" is a referenceto the chessboard metaphor described earlier.] Let'sconsider some examples. Here is one: "I love myhusband, but I get so angry with him." Here isanother: "I want to go, but I am too anxious."Notice that although both say "this be out that,"what the person actually experienced in both caseswas two things: this and that. The "be out" partisn't a description of what happened-it is a pro-scription about how private events should go to-gether. This proscription, however, is exactly whatwe are trying to back out of. No one experiencedthat two private events have to be resolved-in-stead two private events were experienced. If theword "but" is replaced by the word "and," it isalmost always much more honest. So in our ex-amples, it is much more honest and directly in con-tact with what actually happened to say "I love myhusband and I get angry with him" or to say "Iwant to go and I am anxious." So the little con-vention I'd like us to adopt is to say "and" insteadof "but" when we talk. Ifyou try it, you'll see thatalmost always "and" is more true to your experi-ence. "I want to go and I am anxious." Both thingsare true, the wanting to go and the feeling ofanxiety.By calling attention to what we're saying with theuse of this little convention, it will help make youmore sensitive to one of the ways that people getpulled into the piece-level struggle with themselves.It will help us a lot to get off our buts in here. Ifyou really must say the word "but" at some point,then at least we should say it in a way that empha-sizes what we are actually doing. The original formdoes this pretty well, so if we really have to say"but" we will say it in here as "be out."
This convention greatly opens up thepsychological space within which clientsand therapists can work. "And" is a de-scriptive rather than a proscriptive term,and thus can be associated with manycourses of action. All possibilities areopen. The motivated avoidance of pri-vate events that results from their con-ventional connection to action can be re-duced.

300 STEVEN C. HAYES & KELLY G. WILSON
Reactions as Barriers
Here is a lengthy edited excerpt froman ACT session transcript in which theclient raises barrier after barrier. Insteadof these barriers being problems to ther-apeutic work, the ACT therapist treatsthem as the focus oftherapy, as problemsbeing treated in the ACT work. This cli-ent came in complaining of getting con-fused and anxious in work settings. Hewas clinically depressed. The same con-tent-confusion and anxiety-emergedin therapy and was quite distressing thereas well. Note how the therapist repeat-edly undermines psychological avoid-ance and turns the issue from the literalcontent of thoughts and feelings to theunwillingness of the client to experiencethe psychological content that is imme-diately present.
Client: It's hard to hang onto what we're goingthrough.
Therapist: So, don't try to.Client: It's hard not to try to. (chuckle or sigh)Therapist: So, notice that you have the thought
that you want to try to.Client: OK.Therapist: And is it OK to think that you want
to try to hang onto it? That you need to hang on toit? Is it OK to think that?
Client: I would like to say it's OK, but it's reallynot. I feel like I should hold on to it. (sigh)
Therapist: OK, but now let'sjust think that. We'vegot this thing "I got to hang on to this." Is it OKto think "I've got to hang on to this?"
Client: Sure (sigh and chuckle). No-I guess I'mafraid that I won't get it back if I can't hang on tosomething.
Therapist: OK, so you have the thought that itwon't come back ... Is it OK to have those words,"it won't come back?"
Client: If it didn't come back that wouldn't beOK.
Therapist: But you didn't experience that it didn'tcome back, right?
Client: Right, just the fear.Therapist: The fear, right.Client: Uh huh.Therapist: And you also experienced some words
in your head called "But it wouldn't be OK if itdidn't come back."
Client: Right.Therapist: Is it OK to experience the fact that
you have the words called, "but it wouldn't be OKif it didn't come back."
Client: Sure, it's . . . it's OK to have that feeling.Therapist: Great. Next thought.Client: But what if it doesn't come back? (giggle)
Same thing?Therapist: That's the next thought. What's here
to accept is not what it says it is but what youexperience it to be. Now what did you actually ex-perience?
Client: The fear that I'm getting confused and itmight not ever come back. I might not ever un-derstand.
Therapist: is that OK?Client: The fear is OK, um. So right, um, when
I blanking, when I blank out, I'm stuck behind thewords. I couldn't have told you that. There weren'tany thoughts there to describe.
Therapist: Isn't that the most amazingthing; that'strue. The most amazing thing is that when you lookat the world from words you don't actually see thewords.
Client: Yeah, there weren't any. I was just con-fused. I get into a place and my mind isjust nothing,zero.
Therapist: Go with that.Client: And that anything we're talking about here
in the last hour is gone, it's not-Therapist: Stay with that.Client: I can't remember anything.Therapist: OK. Good!Client: Yeah. The thought is that my mind is a
blank and I can't remember.Therapist: OK "my mind is blank" um-any-
thing else your mind has to share?Client: I'm confused.Therapist: Go with that, go right this moment
with that confusion.Client: I have a blank wall in front of me. Oh-
Oh, I had it a second ago. I can't remember whatit is.
Therapist: What was that? Isn't that a thought?Client: Yeah. I had the thought that I can't re-
member what that is.Therapist: OK.Client: (19-s pause) I feel like I don't even know
what we're talking about right now.Therapist: OK, good. Is that OK-to feel that?Client: I need to keep my mind working.Therapist: OK. So you're now having a thought
that you have to keep your mind working.Client: (8-s pause) I'm thinking I should try and
get back into the groove of where we were. I'mconfused.
Therapist: As you think that, can you let that bea thought-not a thing that you are lookingfrom,but as a thing you're looking at. Just watch whatcomes up. (12-s pause)[Client starts to say something and then shakes hishead vigorously as if to "shake it off"]
Therapist: And at that moment, just when yougrab it, what are you shaking of'?
Client: I'm going backwards.Therapist: You're going backwards. I'm slipping!Client: And, I'm-struggling extra hard.Therapist: Great thought.Client: Because I am going backwards. All I can
think about is "I've got to stop it."Therapist: OK, and as you do that, let that be
what it is. This is the thought that pushes you around,and not just in here.
Client: I just thought I had to stop it. I havedecided it is hopeless, I think.

ACCEPTANCE AND COMMITMENT THERAPY 301
Therapist: Great! It is hopeless. In a funny kindof way. This is a healthy kind of hopeless. That'swhere we started, remember?
Client: Oh yeah. I remember. Yes, I do. The firstsession.
Therapist: Yeah, and that wasn't a trick. That'sreal; it is hopeless, in a healthy way. So, let's seewhat is hopeless. What are we trying to do here?
Client: Just to look at my thoughts.Therapist: Right, and all we are really trying to
do is just be here with whichever ones come upwithout struggling with them. Whatever shows up.No particular thing has to show up. Notice howhard that was. Each one kept inviting you to struggleand run away.
Client: Right.
This client was successfully treated byACT. The core of the work was an aban-donment of this obsessive effort to getclear or to remember -an effort that itselfcreated confusion and distress. Ironical-ly, when we accept a feeling ofconfusion,clarity emerges because it is very clearthat we are confused. Clarity, in otherwords, comes from being present withwhat is already present, and in this client'scase what was present was a string ofthoughts about how he needed to besomewhere else. His task in theACT workwas to learn to get present to thesethoughts as thoughts and to do nothingwith them other than to notice them.
OUTCOME AND PROCESSDATA ON ACT
The impact of ACT has been studiedwith several populations, but the outcomedata are still limited. In a randomized clin-ical trial, ACT was shown to be more ef-fective than Beck's cognitive therapy in thetreatment of depression (Zettle, 1984), asmeasured by standard self-report measuresofdepression, when presented in a 12-weekcourse of individual therapy. This was anextraordinary finding in its own way, be-cause a major focus of the ACT protocolwas to open up the client to feeling de-pressed feelings without defense, while atthe same time doing what needed to bedone overtly. Paradoxically, opening up todepressed feelings reduced their intensityand impact. When conducted in a groupformat, a controlled investigation showedACT to be essentially equivalent to cog-nitive therapy on standard depressionmeasures-several of the means were fa-
vorable to ACT but not significantly so(Zettle & Raines, 1989). ACT has beenused to treat the emotional distress offam-ilies with severely physically handicappedchildren-a situation in which removal ofthe stressor is not possible (Biglan, 1990).ACT has also been found to be effectivewith several different anxiety disorders onstandard anxiety measures (Hayes, 1987;Hayes, Afari, McCurry, & Wilson, 1990)in studies using either single-case analysesor group designs with pre- and posttreat-ment measures.
Process research on the change se-quence with ACT clients shows resultsthat are very much in line with theoret-ical expectations. Compared to clients incognitive therapy, ACT clients beingtreated for depression show a somewhatslower drop in the frequency of self-re-ported depressive thoughts but show amuch more rapid drop in the believabilityofthose thoughts (Zettle & Hayes, 1986).This makes sense, because ACT does notfocus at all on changing the form or fre-quency of private events supposedly re-lated to poorer life functioning. The focusinstead is entirely on changes in thefunc-tion of these events. Taking a thoughtliterally in a technical sense (as describedearlier) is quite similar to what is dis-cussed in lay language as believing athought. Being able to have a thoughtwithout necessarily having to adopt it asa basis for action -without believing it-is a core goal ofACT. Similar differencesin process between ACT and cognitivetherapy have been shown in other studies(Zettle, 1984; Zettle & Raines, 1989). Alsoin line with ACT theory, beneficial out-comes have been shown to be related toreductions in emotional avoidance (Kho-rakiwala, 199 1; McCurry, 199 1). In theseprocess studies, transcripts of ACT ses-sions conducted with successful ACT cli-ents were generated. Actual behavioralmeasures ofemotional willingness in ses-sion were developed and were reliablyapplied to client verbalizations presentedsimultaneously both in audiotape andtranscript form. Emotional willingnessincreased over time, both from the be-ginning of sessions to the end of sessionsand from the beginning of therapy to the

302 STEVEN C. HAYES & KELLY G. WILSON
end oftherapy (Khorakiwala, 1991). Theexpansion ofthe ability to experience pri-vate events without avoidance was as-sociated with other key ACT concepts,such as the ability to make and keep com-mitments.The empirical analysis ofACT is in its
infancy, in part because the treatment de-velopment strategy we have followed isunusual and lengthy. We have conscious-ly built ACT in a six-step process in-volving philosophy, methodology, basictheory and research, applied theory andresearch, assessment technology, and in-tervention technology.
In the usual empirical approach to ap-plied intervention techniques, a specificapplied problem is defined and a prelim-inary approach to its amelioration is de-veloped based on existing techniques anddata. This approach is tested and refinedand then compared to other approachesfor the same problem. In the process, ad-ditions are made to the intervention andit becomes a treatment package. Group-comparison treatment-outcome studiesare then conducted. If it works, a seriesof package-dismantling studies are con-ducted to determine the essential com-ponents. Finally, possible theoreticalmechanisms are examined to determinethe means through which clinical impactoccurs.Our approach has been quite different.
We have attempted to clarify and extendour philosophical assumptions so thatconsistent units ofanalysis and truth cri-teria tied together our basic and appliedwork. Our work on functional contex-tualism was the result (e.g., Hayes, Hayes,& Reese, 1988; Hayes, Hayes, Reese, &Sarbin, 1993). We have tried to developan inductive and intensive approach totreatment development methodology(e.g., Barlow, Hayes, & Nelson, 1984).We have developed a program of basicbehavioral research on how verbal rela-tions change the way contingencies guidebehavior (e.g., Hayes, 1989; Hayes &Hayes, 1992). It is in that context thatwe have developed the beginnings of atheory ofpsychopathology (e.g., Hayes &Wilson, 1993), assessment devices need-ed to assess that theory in the applied
domain (e.g., Khorakiwala, 1991; Mc-Curry, 1991), and finally an interventiontechnology (e.g., Kohlenberg, Hayes, &Tsai, 1993) and preliminary tests of itsefficacy.
In other words, we argue that much ofthe current support for the ACT ap-proach can be found in the foundationalwork that underlies the technique. Fol-lowing an inductive, technique-buildingstrategy, we are only now to the point atwhich larger scale outcome studies seemto be worthwhile. We have recently re-ceived a grant from the National Instituteon Drug Abuse to launch such an effort.Whether ACT will be more helpful thanother approaches is not presently clear,but it does seem clear that ACT can haveat least some beneficial impact and thatit may act according to different pro-cesses than other forms of psychothera-py-
CONCLUSIONBehavior analysis has had a very lim-
ited impact on adult outpatient psycho-therapy work, compared to its dramaticimpact on work with children or insti-tutionalized populations. This is largelybecause the core ofadult outpatient ther-apy is work on the role ofhuman verbalbehavior. Behavior therapists have large-ly "gone cognitive" because of this core,but they have adopted a mechanistic andmentalistic model in part because no oth-er approaches have presented them-selves. Contemporary behavior-analyticviews of verbal behavior provide a pow-erful alternative. In the examples above,ACT therapists at times use mentalisticand dualistic terms (e.g., "mind") tocommunicate most readily with clients,but at every point the underlying ratio-nale and theory is both nonmentalisticand contextualistic. Behavior-analyticpsychotherapies provide a new domainwithin which to explore the applied im-pact of contemporary behavioral theory.
REFERENCESBarlow, D. H., Hayes, S. C., & Nelson, R. 0. (1984).The scientist-practitioner: Research and account-

ACCEPTANCE AND COMMITMENT THERAPY 303
ability in clinical and educational settings. NewYork: Pergamon.
Biglan, A. (1990). A contextual approach to treat-ing family distress. In G. Singer & L. Irvin (Eds.),Supporting the family: Enabling a positive ad-justment to children with disabilities (pp. 299-31 1). Baltimore: Paul H. Brookes.
Hayes, S. C. (1984). Making sense of spirituality.Behaviorism, 12, 99-1 10.
Hayes, S. C. (1987). A contextual approach totherapeutic change. In N. S. Jacobson (Ed.), Psy-chotherapists in clinical practice: Cognitive andbehavioralperspectives (pp. 327-387). New York:Guilford.
Hayes, S. C. (Ed.). (1989). Rule-governed behav-ior: Cognition, contingencies, and instructionalcontrol. New York: Plenum.
Hayes, S. C., Afari, N., McCurry, S. M., & Wilson,K. (1990, May). The efficacy ofcomprehensivedistancingin the treatment ofagoraphobia. Posterpresented at the 16th annual convention of theAssociation for Behavior Analysis, Nashville, TN.
Hayes, S. C., Brownstein, A. J., Devany, J. M.,Kohlenberg,B.S.,&Shelby,J. (1987). Stimulusequivalence and the symbolic control of behav-ior. Mexican Journal of Behavior Analysis, 13,361-374.
Hayes, S. C., & Hayes, L. J. (1989). The verbalaction of the listener as a basis for rule-gover-nance. In S. C. Hayes (Ed.), Rule-governed be-havior: Cognition, contingencies, and instruction-al control (pp. 153-190). New York: Plenum.
Hayes, S. C., & Hayes, L. J. (1992). Verbal rela-tions and the evolution of behavior analysis.American Psychologist, 47, 1383-1395.
Hayes, S. C., Hayes, L. J., & Reese, H. W. (1988).Finding the philosophical core: A review of Ste-phen C. Pepper's World hypotheses. Journal ofthe Experimental Analysis of Behavior, 50, 97-111.
Hayes, S. C., Hayes, L. J., Reese, H. W., & Sarbin,T. R. (Eds.). (1993). Varieties ofscientific con-textualism. Reno, NV: Context Press.
Hayes, S. C., Kohlenberg, B. S., & Hayes, L. J.(1991). Transfer of consequential functionsthrough simple and conditional equivalenceclasses. Journal of the Experimental Analysis ofBehavior, 56, 119-137.
Hayes, S. C., Kohlenberg, B. S., & Melancon, S. M.(1989). Avoiding and altering rule control as astrategy ofclinical treatment. In S. C. Hayes (Ed.),Rule-governed behavior: Cognition, contingen-cies, andinstructional control (pp. 359-385). NewYork: Plenum.
Hayes, S. C., & Melancon, S. M. (1989). Com-
prehensive distancing, paradox, and the treat-ment ofemotional avoidance. In M. Ascher (Ed.),Paradoxicalprocedures inpsychotherapy(pp. 184-218). New York: Guilford.
Hayes, S. C., Strosahl, K., & Wilson, K. D. (inpress). Acceptance and Commitment Therapy.New York: Guilford.
Hayes, S. C., & Wilson, K. G. (1993). Some ap-plied implications of a contemporary behavior-analytic account of verbal events. The BehaviorAnalyst, 16, 283-301.
Khorakiwala, D. (1991). An analysis oftheprocessofclient change in a contextual approach to ther-apy. Unpublished doctoral dissertation, Univer-sity of Nevada, Reno.
Kohlenberg, B. S., Hayes, S. C., & Hayes, L. J.(1991). The transfer of contextual control overequivalence classes through equivalence classes:A possible model of social stereotyping. Journalofthe ExperimentalAnalysis ofBehavior, 56,505-518.
Kohlenberg, R. J., Hayes, S. C., & Tsai, M. (1993).Radical behavioral psychotherapy: Two contem-porary examples. Clinical PsychologyReview, 13,579-592.
Kohlenberg, R. J., Tsai, M., & Dougher, M. J.(1993). The dimensions of clinical behavioranalysis. TheBehaviorAnalyst, 16, 271-282.
McCurry, S. M. (1991). Client metaphor use in acontextualform oftherapy. Unpublished doctoraldissertation, University of Nevada, Reno.
McCurry, S. M., & Hayes, S. C. (1993). Metaphor:A basic and applied analysis. Clinical PsychologyReview, 12, 763-785.
Sidman, M., & Tailby, W. (1982). Conditionaldiscrimination versus matching to sample: Anexpansion ofthe testing paradigm. Journal oftheExperimental Analysis ofBehavior, 37, 5-22.
Wulfert, E., & Hayes, S. C. (1988). The transferof conditional sequencing through conditionalequivalence classes. Journal ofthe ExperimentalAnalysis ofBehavior, 50, 125-144.
Zettle, R. D. (1984). Cognitive therapy ofdepres-sion:A conceptual and empirical analysis ofcom-ponent and process issues. Unpublished doctoraldissertation, University of North Carolina atGreensboro.
Zettle, R. D., & Hayes, S. C. (1986). Dysfunc-tional control by client verbal behavior: The con-text of reason giving. The Analysis of Verbal Be-havior, 4, 30-38.
Zettle, R. D., & Raines, J. C. (1989). Group cog-nitive and contextual therapies in treatment ofdepression. Journal of Clinical Psychology, 45,438-445.




















