A Case of Zollinger-Ellison Syndrome whose Pancreatic ...
15
Jap. J. Clin. Oncol. 1978, 8(1), 75-89 A Case of Zollinger-Ellison Syndrome whose Pancreatic Tumor Produced Multiple Hormones and a Review of 48 Cases Reported in the Japanese Literature HiROSHI TAKAMI, M.D., KEN YAMAGUCHI, M.D.*, KAORU ABE. M.D.*, ISAMU ADACHr, M.D.*, SABURO ARAI, M.D.*, TORU KAMEYA, M.D.*, KATSUMI YAMACHIKA, M.D.**, MASAO TASHIRO, M.D., YORIO NAKAGAWA, M.D. and OSAHIKO ABE, M.D. Departments of Surgery and Pathology, Kelo University School of Medicine, Tokyo, Japan * Endocrinology and Pathology Divisions, National Cancer Center Research Institute, Tokyo, Japan **Yamachika Hospital, Kanagawa, Japan Abstract A 46-year-old man developed a peptic ulcer disease and a diagnosis of Zollinger-Ellison Syndrome was strongly suspected following gastric acid stu- dies. Plasma gastrin level was found to be elevated. The operation revealed a pancreatic tumor localized at the pancreas tail. The resected tumor tissue was proved to contain large amounts of immunoreactive gastrin. In addition, calci- tonin, VIP and insulin were found to be present either as a result of immuno- fluorescence studies or the respective radioimmunoassays. Therefore, this was a case of a multiple hormone producing tumor of pancreas islet cell origin, and the symptoms due to gastrin hypersecretion were the main clinical features. In addition, 48 cases of Zollinger-Ellison Syndrome reported in Japanese liter- atures were reviewed. Introduction for ZES, and the number of reported cases is increasing (Wilson, 1973). Recently, Zollinger-Ellison Syndrome (ZES) is a secretin and calcium infusion tests are proved well known but rare clinical entity, which is to be a sensitive and reliable method for caused by overproduction of gastrin in tumor diagnosing ZES (Straus and Yalow, 1975). tissues, mostly in islet cell tumor of the It has become apparent that ZES is one pancreas. Since the gastrin radioimmuno- of the clinical manifestations of multiple assay became available (McGuigan, 1969; endocrine adenomatosis (MEA) type 1 Yalow and Berson, 1970), plasma gastrin (Ballard et al., 1964), and it has become levels have been used as a "tumor marker" important to examine the presence of MEA in patients with ZES and in their family Received May 1, 1978. members This work was supported in part by Grants- „ . , __„ in-Aid from the Ministry of Education, Science Here > we are reporting a case of ZES and Culture, the Ministry of Health and Wei- whose diagnosis was strongly suspected by fare, and Development Medical Research examining gastric acid secretion at the time Foundation for Adult Diseases, Japan. of first operation, which revealed a tumor Reprint requests: Kaoru Abe M.D., Endo- , o c a t e d a t f h e feas tai , p ost tive , crinology Division, National Cancer Center , , • , , , I Research Institute, 5-1-1 Tsukiji, Chuo-ku, he was als0 exam.ned for the presence of Tokyo 104, Japan. MEA. at Pennsylvania State University on September 12, 2016 http://jjco.oxfordjournals.org/ Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of A Case of Zollinger-Ellison Syndrome whose Pancreatic ...

Jap. J. Clin. Oncol. 1978, 8 ( 1 ) , 7 5 - 8 9
A Case of Zollinger-Ellison Syndrome whose Pancreatic TumorProduced Multiple Hormones and a Review of 48
Cases Reported in the Japanese Literature
HiROSHI TAKAMI, M.D., KEN YAMAGUCHI, M.D.*, KAORU ABE. M.D.*,ISAMU ADACHr, M.D.*, SABURO ARAI, M.D.*, TORU KAMEYA, M.D.*,
KATSUMI YAMACHIKA, M.D.**, MASAO TASHIRO, M.D.,YORIO NAKAGAWA, M.D. and OSAHIKO ABE, M.D.
Departments of Surgery and Pathology, Kelo UniversitySchool of Medicine, Tokyo, Japan
* Endocrinology and Pathology Divisions, National Cancer CenterResearch Institute, Tokyo, Japan
**Yamachika Hospital, Kanagawa, Japan
Abstract
A 46-year-old man developed a peptic ulcer disease and a diagnosis ofZollinger-Ellison Syndrome was strongly suspected following gastric acid stu-dies. Plasma gastrin level was found to be elevated. The operation revealed apancreatic tumor localized at the pancreas tail. The resected tumor tissue wasproved to contain large amounts of immunoreactive gastrin. In addition, calci-tonin, VIP and insulin were found to be present either as a result of immuno-fluorescence studies or the respective radioimmunoassays. Therefore, this wasa case of a multiple hormone producing tumor of pancreas islet cell origin,and the symptoms due to gastrin hypersecretion were the main clinical features.In addition, 48 cases of Zollinger-Ellison Syndrome reported in Japanese liter-atures were reviewed.
Introduction for ZES, and the number of reported casesis increasing (Wilson, 1973). Recently,
Zollinger-Ellison Syndrome (ZES) is a secretin and calcium infusion tests are provedwell known but rare clinical entity, which is to be a sensitive and reliable method forcaused by overproduction of gastrin in tumor diagnosing ZES (Straus and Yalow, 1975).tissues, mostly in islet cell tumor of the It has become apparent that ZES is onepancreas. Since the gastrin radioimmuno- of the clinical manifestations of multipleassay became available (McGuigan, 1969; endocrine adenomatosis (MEA) type 1Yalow and Berson, 1970), plasma gastrin (Ballard et al., 1964), and it has becomelevels have been used as a "tumor marker" important to examine the presence of MEA
in patients with ZES and in their familyReceived May 1, 1978. membersThis work was supported in part by Grants- „ . , __„
in-Aid from the Ministry of Education, Science H e r e> w e a r e reporting a case of ZESand Culture, the Ministry of Health and Wei- whose diagnosis was strongly suspected byfare, and Development Medical Research examining gastric acid secretion at the timeFoundation for Adult Diseases, Japan. o f first operation, which revealed a tumor
Reprint requests: Kaoru Abe M.D., Endo- , o c a t e d a t f h e f e a s t a i , p o s t t i v e ,crinology Division, National Cancer Center , , • , , , IResearch Institute, 5-1-1 Tsukiji, Chuo-ku, h e w a s a l s 0 exam.ned for the presence ofTokyo 104, Japan. MEA.
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
76 TAKAMI et al.Jap. J. Clin. Oncol.June 1978
In the tumor tissue, various polypeptidehormones such as gastrin, calcitonin, vaso-active intestinal polypeptide (VIP), C-pep-tide and insulin were examined either byradioimmunoassays or by immunofluorescenttechniques.
In addition, ZES in Japanese literaturesreported between 1961 and 1976 were re-viewed.
Case Report
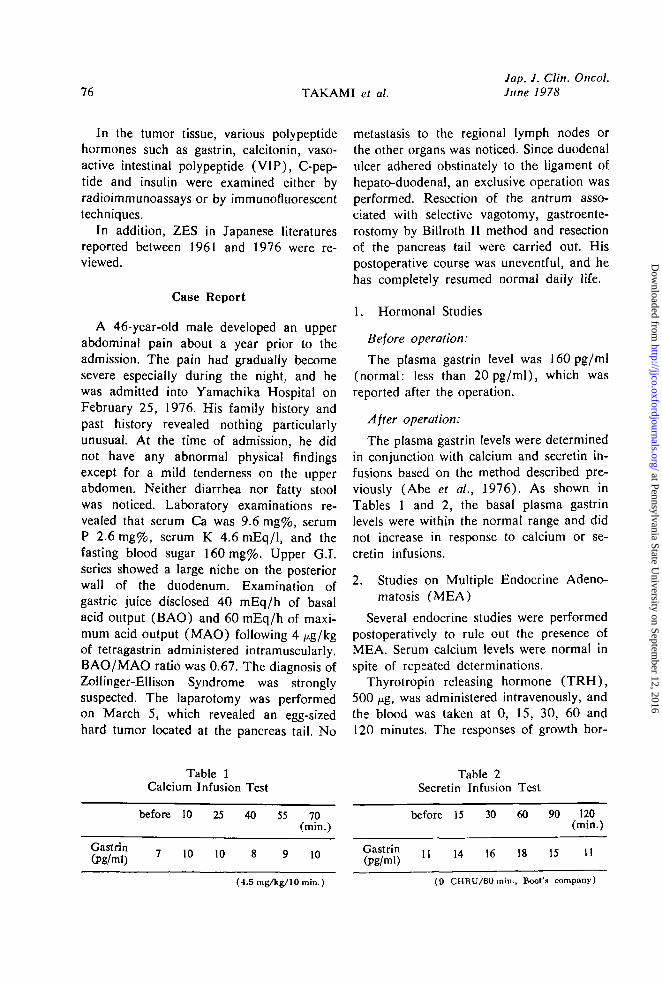
A 46-year-old male developed an upperabdominal pain about a year prior to theadmission. The pain had gradually becomesevere especially during the night, and hewas admitted into Yamachika Hospital onFebruary 25, 1976. His family history andpast history revealed nothing particularlyunusual. At the time of admission, he didnot have any abnormal physical findingsexcept for a mild tenderness on the upperabdomen. Neither diarrhea nor fatty stoolwas noticed. Laboratory examinations re-vealed that serum Ca was 9.6 mg%, serumP 2.6 mg%, serum K 4.6 mEq/1, and thefasting blood sugar 160 mg%. Upper G.I.series showed a large niche on the posteriorwall of the duodenum. Examination ofgastric juice disclosed 40 mEq/h of basalacid output (BAO) and 60 mEq/h of maxi-mum acid output (MAO) following 4 /ng/kgof tetragastrin administered intramuscularly.BAO/MAO ratio was 0.67. The diagnosis ofZollinger-Ellison Syndrome was stronglysuspected. The laparotomy was performedon March 5, which revealed an egg-sizedhard tumor located at the pancreas tail. No
metastasis to the regional lymph nodes orthe other organs was noticed. Since duodenalulcer adhered obstinately to the ligament ofhepato-duodenal, an exclusive operation wasperformed. Resection of the antrum asso-ciated with selective vagotomy, gastroente-rostomy by Billroth II method and resectionof the pancreas tail were carried out. Hispostoperative course was uneventful, and hehas completely resumed normal daily life.
1. Hormonal Studies
Before operation:
The plasma gastrin level was 160pg/ml(normal: less than 20pg/ml), which wasreported after the operation.
After operation:
The plasma gastrin levels were determinedin conjunction with calcium and secretin in-fusions based on the method described pre-viously (Abe et al., 1976). As shown inTables 1 and 2, the basal plasma gastrinlevels were within the normal range and didnot increase in response to calcium or se-cretin infusions.
2. Studies on Multiple Endocrine Adeno-matosis (MEA)
Several endocrine studies were performedpostoperatively to rule out the presence ofMEA. Serum calcium levels were normal inspite of repeated determinations.
Thyrotropin releasing hormone (TRH),500 fxg, was administered intravenously, andthe blood was taken at 0, 15, 30, 60 and120 minutes. The responses of growth hor-
Table 1Calcium Infusion Test
before 10 25 40 55 70(min.)
Gastrin(Pg/ml) 10 10 10
(4.5 mgAg/10 min.)
Table 2Secretin Infusion Test
before 15 30 60 90 120(min.)
gggj 1! 14 .6 18 15 11
(9 CHRU/60 min., Boot's company)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 Z0LL1NGER-ELLIS0N SYNDROME 77
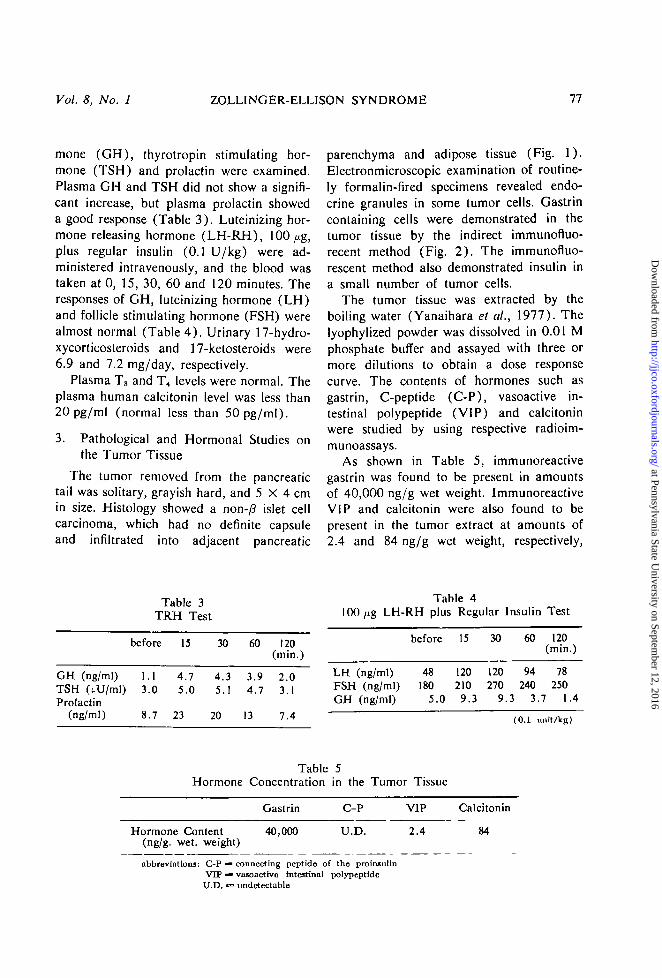
mone (GH), thyrotropin stimulating hor-mone (TSH) and prolactin were examined.Plasma GH and TSH did not show a signifi-cant increase, but plasma prolactin showeda good response (Table 3). Luteinizing hor-mone releasing hormone (LH-RH), 100/ig,plus regular insulin (0.1 U/kg) were ad-ministered intravenously, and the blood wastaken at 0, 15, 30, 60 and 120 minutes. Theresponses of GH, luteinizing hormone (LH)and follicle stimulating hormone (FSH) werealmost normal (Table 4) . Urinary 17-hydro-xycorticosteroids and 17-ketosteroids were6.9 and 7.2 mg/day, respectively.
Plasma T3 and T^ levels were normal. Theplasma human calcitonin level was less than20pg/ml (normal less than 50pg/mI).
3. Pathological and Hormonal Studies onthe Tumor Tissue
The tumor removed from the pancreatictail was solitary, grayish hard, and 5 X 4 cmin size. Histology showed a non-/3 islet cellcarcinoma, which had no definite capsuleand infiltrated into adjacent pancreatic
parenchyma and adipose tissue (Fig. 1).Electronmicroscopic examination of routine-ly formalin-fired specimens revealed endo-crine granules in some tumor cells. Gastrincontaining cells were demonstrated in thetumor tissue by the indirect immunofluo-recent method (Fig. 2) . The immunofluo-rescent method also demonstrated insulin ina small number of tumor cells.
The tumor tissue was extracted by theboiling water (Yanaihara et ah, 1977). Thelyophylized powder was dissolved in 0.01 Mphosphate buffer and assayed with three ormore dilutions to obtain a dose responsecurve. The contents of hormones such asgastrin, C-peptide (C-P), vasoactive in-testinal polypeptide (VIP) and calcitoninwere studied by using respective radioim-munoassays.
As shown in Table 5, immunoreactivegastrin was found to be present in amountsof 40,000 ng/g wet weight. ImmunoreactiveVIP and calcitonin were also found to bepresent in the tumor extract at amounts of2.4 and 84 ng/g wet weight, respectively,
GH (ng/ml)TSH (tU/ml)Prolactin
(ng/ml)
Table 3TRH Test
before 15
1.1 4.73.0 5.0
8.7 23
30
4.35.1
20
60
3.94.7
13
120(min.)
2.03.1
7.4
Table 4lOO^g LH-RH plus Regular
LH (ng/ml)FSH (ng/ml)GH (ng/ml)
before
48180
5.0
15
120210
9.3
30
120270
9
Insulin Test
60 120(min.)
94 78240 250
.3 3.7 1.4
(0.1 unitAg)
Table 5Hormone Concentration in the Tumor Tissue
Gastrin C-P VIP
Hormone Content 40,000(ng/g. wet. weight)
U.D. 2.4
Calcitonin
84
abbreviations: C-P ^ connecting peptide of the proinsullnVTP ^ vasonctive intestinal polypeptideU.D. •» undetectable
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
78 TAKAMI et al.Jap. J. Clin. Oncol.June 1978
Table 6ZES Reported in Japanese Literatures
Chief ComplaintNo. Age Sex (on initial
operation)
t Gastricft.0* Juiceu l c c r (mEq/h)
GastrinLevel
(pg/ml)
Course afterJ L ! l the InitialOperation operation
1 39 M upper abdominal duodenum hyperaciditypain
2 69 M hematemesis stomach hyperacidityconstipation
3 43 M upper abdominal stomach hyperaciditypain, hemate-mesis
4 43 M upper abdominal stomach hyperaciditypain
gastric resec-tion withpancreas tailresection ofulcergastricresection,B-I
gastricresection
stomal ulcer
stomal ulcer
5 38 F (+) hyperacidity
6 51 M upper abdominal duodenum, hyperaciditypain, melena stomach
gastricresection
stomal ulcer
7 35 M abdominal tumor stomach, hyperacidity& watery diarrhea duodenum
laparotomy abdominalpain, ileus
45 M duodenum, hyperaciditystomach
9 57 M epigastralgia stomach hyperacidity
10 65 M upper abdominal duodenum,pain, melena, stomachhematemesis
11 55 M upper abdominal duodenum hyperaciditypain, melenahematemesis
12 57 F pancreatic tumor stomach at night2000ml/12hfree acid164mEq/l
13 72 M watery diarrhea, stomach hyperacidityhematemesis,melena
gastricresection
gastricresectionwith B-Ugastricresection
stomal
stomal
ulcer
ulcer
laparotomy stomal ulcer
no operation
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLINGER-ELLISON SYNDROME 79
FinalOperation
total gastrec-tomy with pan-creatic body &tail resectiontotal gastrec-tomy with pan-creas head andtail resectionsubtotalgastrectomyresection ofpancreatic headsubtotal gas-trectomy andvagotomy withtumorresection
total gastrec-tomy resectionof tumorpancreatoduo-denectomy
gastric resec-tion
Number j ^ e t a .
ation
1 (-)
1 (+)
4 (-)
4 (-)
5 (-)
3 lymphnodes onpan-creas
1 (-)
4 (-)
4 (-)
1 (-)
4 (-)
1 liver
0 ( - )
Tumor
Location
pancreastail
pancreas
pancreasbody
pancreastail
pancreashead
duodenum
pancreasheadmultiple
pancreastail
pancreashead
pancreasbody andtailpancreas
pancreas,multiple
pancreaticbody
Pathology
non-y? isletcell adenoma
islet-cellcarcinomanon-/3 isletcell adenoma
islet cellmicro-adenomatosis
islet celladenoma
non-/? isletcellcarcinoma
non-fi isletcell adenoma
non-)3 isletcell adenoma
islet cellmicro-adenomatosisislet cellmicro-adenomatosisislet cellhyperplasia
islet cellcarcinoma
pancreasduct cellcarcinoma
Outcome
alive
died
alive
died
died7 days pop. (pneu-monia)
died ofileus 11days p op.
alive
alive
died10 days pop.
alive
died ofhemate-mesis &melena
Remarks
MEA?serum Ca11.4 mg%serum. K1.9-3.3mEq/lG T T -DM pattern
ulcer inseveralmembers offamilyIt.-adrenaltumor
Reporter(year)
Murata (1961)
Kozawa(1963)Daikoku etal. (1964)
Murata et al.(1965)
Yaoreported byTanaka(1966)Yoshinaga(1966)
Oda (1966)
Murata et al.(1967)
Murata et al.(1967)
JHamaguchi &Komi( 1967)
Abe et al.(1967)
Sugisakiet al.(1967)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from

80
No.
14
15
16
17
18
19
20
21
Age
57
65
33
13
64
53
33
28
Sex
F
M
F
M
M
M
M
F
Chief Complaint(on initialoperation)
epigastralgia
upper abdominalpain
epigastralgia
epigastralgia,melena
pyloric stenosis,upper abdominalpain
upper abdominalpain
upper abdominalDain. vomitine.
TAKAMI et al.
Location ofInitial UlceT
stomach
duodenum
duodenum
duodenum
stomach
duodenum
stomach,duodenum
duodenum
Gastric GastrinJuice Level
(mEq/h) (pg/ml)
hyperacidityat night950ml/12hhyperacidity
hypersecre-tion
*2MAO 11.5
hyperacidity #32550(N=<100)
MAO 24.6ratio 0.79
Jap.June
InitialOperation
subtotalgastrectomyB-Igastric resec-tion, B-I
gastricresection
gastricresection
gastricresection
gastricresectionB-I
gastricresectionB-ngastricresection
/. Clin. Oncol.1978
Course afterthe InitialOperation
stomal ulcer
stomal ulcerwaterydiarrheastomal ulcer
stomal ulcerupperabdominalpain
stomal ulcerhematemesis
stomal ulcerhematemesis
22 40 M hematemesis
23 25 M
25 56
duodenum # 2BAO 45.4MAO 60.3ratio 0.75
BAO 33.6MAO 59.5ratio 0.56
pain
F attack ofhypoglycemia
$2390-860
#3180-640
24 44 M upper abdominal stomach, BAO 10.5 265
26 37 M
duodenum MAO 28.1ratio 0.59at night1100ml/12hrs
duodenum,stomach
(+) hyperacidity
gastricresectionB-U
gastricresectionB-U
upperabdominalpain,hematemesisupperabdominalpain,hematemesis,melena
resection of Co^-irradia-pancreatic tion to thetail & spleen liver
27 40
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLINGER-ELLISON SYNDROME 81
Final dumber M e ( a .Operation ° \ ^ r ' stasis
Tumor
Location PathologyOutcome Remarks Reporter
(year)
1
subtotal gas-trectomy withduodenaltumor resection
gastric resec-tion, R-Y
gastric resec-tion
gastric resec-tion & vago-tomy, resectionof pancreatictailtotal gastrec-tomy
total gastrec-tomy, resectionof transversecolon
totalgastrectomy
gastricresection R-Y
pancreasbody & tail
duodenum
pancreas,multiple
pancreas
pancreastail
pancreastail
pancreas
pancreastail
islet cellmicroadeno-matosissubmucosaltumor
islet celladenoma
islet cellcarcinoma
non-3 isletcellcarcinomanon-/f isletcarcinoma
normal onmacroscopicobservationislet cellhyperplasia
alive
alive
died ofbleeding 14days p op.died
died ofbleeding
died ofcancer in2.5 yearsP op.
alive
died on 22days p op.
alive
alive
alive
Murata et al.(1967)
Yamaguchi &Hiramatsu(1968)
Kishimoto etal. (1968)
Hirota et al.(1968)
MEA? Nagai(1968)
Hisama et al.(1969)
Tanaka & Tai(1972)
MEA+ Ichinomiya etparathyroid al. (1973)adenomaadrenocorti-cal adenoma
Sugiyama etal. (1973)
Sugiyama etal. (1973)
Segawa et al.(1973)
(angio. andERCP)
subtotalgastrectomyresection ofpancreatictumor
(+) pancreas
( - ) pancreas
( —) pancreas
islet cellcarcinoma
died
diedislet celladenomaislet cell aliveadenoma
Maruyama etal. (1973)
Nagashima etal. (1973)Nagashima etal. (1973)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
82 TAKAMI et al.Jap. J. Clin. Oncol.June 1978
Chief ComplaintNo. Age Ssx (on initial
operation)
GastricJuice
(mEq/h)
GastrinLevel
(Pg/ml)
Initial Course after
<*&• ISJSK28 66 M stomach
29 45 F upper abdominal doudenum hyperaciditypain, hemate-mesis
gastricresection
stomal ulcer,hematemesis,melena
30 37 M upper abdominal duodenum $ 2 $ 2pain 3000- 690-980
5000ml/dayBAO 14.4MAO 22.5ratio 0.64
31 44 M G.I. symptoms stomach hyperacidity elevated
gastricresectionB-U
gastricresectionB-II
upperabdominalpain, tarrystool, stomalulcer
hematemesisdiarrhea
33 38 M
34 46 M
35 44
36 57 M
37 42
38 58
39 40
perforation
thoracic pain,hematemesis,melena
upper abdominalpain
hematemesismelena
upper abdominaland back pain
duodenalperforation
duodenalperforation
stomach
duodenum
cardiaduodenum
duodenum
duodenum
duodenum
hyperacidity2000-2500 ml/24hrs
hyperacidityratio 0.65at night1750ml/12h
BAO 19.28MAO 7.09ratio 2.72
hyperacidity
BAO 35MAO 56.3ratio 0.62at night2100ml/12hhyperacidityratio 0.14
hyperacidityratio 0.5
hyperacidity
preoperation1400-1800postopera-tion normal
preoperation1400,postopera-tion200-normal
1300
after #2 op.1M 4253M 1630
18M 65523M 557#2630, 1380
gastricresectionB-n
subtotalgastrectomyresection ofthe pancrea-tic body &tailgastricresectionB-I
gastricresectionB-IIlaparotomybiopsy
gastricresection,B-n
gastricresection
gastricresection
perforation,melena
stomal ulcer
stomal ulcer
stomal ulcer,upper ab-dominal pain
hematemesisand melena
stomal ulcer
stomal ulcerhematemesismelena
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLINGER-ELLISON SYNDROME 83
Final dumber M e t a .Operation VtiAn stasis
Tumor
ation Location PathologyReporter
(year)
totalgastrectomyresection ofpancreatic tailgastricre-resection
vagotomy
totalgastrectomyresection ofpancreatic tail
0 pancreas
pancreas
pancreas
pancreas
pancreaticbody
islet cell died ofhyperplasia cerebral
bleedingislet cell died ofcarcinoma cancer
micro- diedadenomatosis
2 adenoma µ-adenomatosis
non-3 isletcell adenoma
normal onmcarcoscopicobservation
died
alive
alive
MEA?
waterydiarrhea
MEA-1pituitaryhyperplasiaparathyroidhyperplasia
MEAparathyroidmicro-adenomaadrenalmicro-adenoma
antral G cellhyperplasia
Emoto (1973)
Hirate andNegishi(1973)
Sugiyama etal. (1973)
Yamada et al.(1973)
Yoshizaki etal. (1973)
M. Abe(1974)
totalgastrectomy,R-Y
selective vago-tomy resectionof tumor
( - )
totalgastrectomy,partial pan-creatomy andsplenectomyresection ofpancreatic tail
totalgastrectomy
2
2
1
2
3
3
( - )
liver
lymph-nodeliver
liver
( - )
pancreatichead
pancreas
pancreastail
pancreastail
pancreaticbody
non-/? isletcell adenoma
malignantislet celltumor
non-/? isletcellcarcinoma
non-/? isletcellcarcinomaislet celladenoma
alive
alive
alive
alive
died
Ca. andSecretin testbeforeoperation
#3Ca. & Sec.test
Endo, A.,et al. (1975)
Emina &Yura (1975)
Shiono et al(1975)
Endo, I., etal. (1975)
Inomata et al(1975)
Tomita et al(1975)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from

84 TAKAMI et al.Jap. J. Clin. Oncol.June 1978
No. Age SexChief Complaint
(on initialoperation)
GastricJuice
(mEq/h)
GastrinLevel
(Pg/ml)
InitialOperation
Course afterthe InitialOperation
40 59 M stomachduodenum
41
42
43
44
37
42
68
34
M
M
M
M
upper abdominalpain
upper abdominalpain
upper abdominalpain
perforationbleeding
duodenum
duodenum
stomach
duodenumstomach
hyperacidity
#2BAO 4.1MAO 3.5
#2BAO 40
82BAO 4.6MAO 5.3ratio 0.86
#2920tumor4820pg/mg*284(normal<20)
#2145-180(normal <20)
gastricresection,B-ngastricresection
gastricresection
gastricresection
stomal ulcerupper ab-dominal painstomal ulcer
diarrheastomal ulcer
45 71 upper abdominalpain
stomach #550(normal<20)
gastricresection
stomal ulcerhematemesismelena
46 32 F upper abdominal duodenum hyperacidity p op.pain ratio 0.76 26M 405
42M 970
47 66 F vomitting duodenum hyperacidity 1300-3200
48 46 M upper abdominal duodenum BAO 40 792pain MAO 60
ratio 0.67
gastricresection,B-n totalvagotomygastricresection
antrum re-section, B-IIselectivevogotomy
stomal ulcer
vomittingupper ab-dominal painno problem
# indicates the number of operation, and the studies were performed prior to this operation
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLING ER-ELLISON SYNDROME 85
Final "umber Meta-Operation o t
a ^ r " stasisTumor
Location PathologyOutcome Remarks Reporter
(year)
pancreas non-5 isletcellcarcinoma,immuno-staininggastrin ( + )
Miyoshi et al.(1976)
subtotal gastrec-tomy resection ofpancreatic tailtotalgastrectomypartial resec-tion of pancreastotalgastrectomypartial resec-tion of pancreas
totalgastrectomyresection ofpancreatictumor
totalgastrectomypartiat resec-tion of pancreas
totalgastrectomy
subtotalgastrectomy
( - )
4
3
2
3
5
4
2
1
( —)
( - )
( —)
( - )
( - )
( + )liver
(+)liver
( - )
pancreatictail
pancreas
pancreasmultiple
pancreas
pancreas
pancreas
gallbladder
pancreastail
islet cellhyperplasia
4 non-/?islet celladenomas
non-5 isletcell adenoma
non-/? isletcell adenomaimmuno-staininggastrin ( + )
non-5 isletcell adenomaimmuno-staininggastrin ( + )
non-5 isletcellcarcinoma
non islet cellcarcinomaimmuno-staininggastrin (+ )tumor tissuegastrin39.6//g/g
alive
alive
died
alive
died
alive
died
alive
#2Ca test(positive)
#2Ca test(positive)MEA-Ifamilyhistory ( + )MEA-1familyhistory ( + )PTHl.Ong/ml(normal 0.3)GH (acro-megalicresponse toglucose &TRH)before #5 opCa & Sec test(positive)MEA ( + )thyroidadenoma,GI tractcarcinoid,adrenaladenoma,
Ca & insulintest response
Matsuki et al«(1976)
Ando et al.(1976)
K. Abe et al.(1976)
K. Abe et al.(1976)
K. Abe et al.(1976)
Komi et al.(1976)
Hirai et al.(1976)
Takami et al.(1976)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from

88 TAKAMI et at.Jap. 1. Clin. Oncol.June 1978
'**&
r-ig. I : Histology oi non-/-: islet eel! carcinoma showing infiltration to the sur-rounding tissue without definite capsule. (H.E. X650)
Fig. 2: The presence of gastrin in the cells of the islet cell carcinoma, revealedby indirect immunofluorescent method, using rabbit antiserum to synthetic gastrin(supplied by Dr. N. Yanaihara, Shizuoka College of Pharmacy, Shizuoka).(X400)
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLINGER-ELLISON SYNDROME 87
Table 7Pathological Findings of ZES Reported
in Japanese Literature
Cases examinedAdenoma (multiple)Carcinoma (meta +)Microadenomatosis
or hyperplasia
No. of
401615
9
Case
( 6)(11)
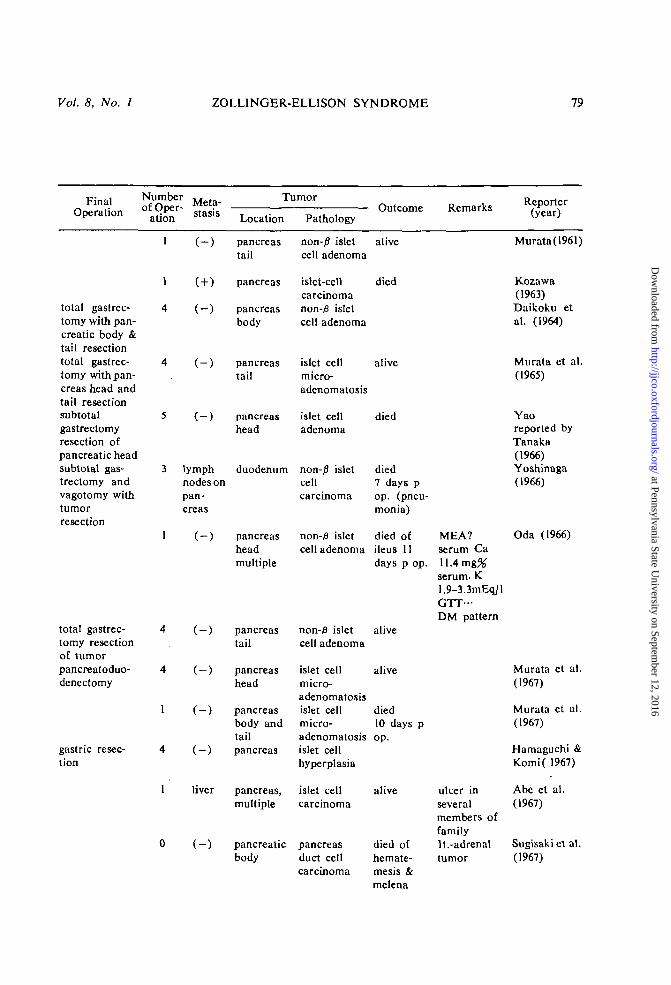
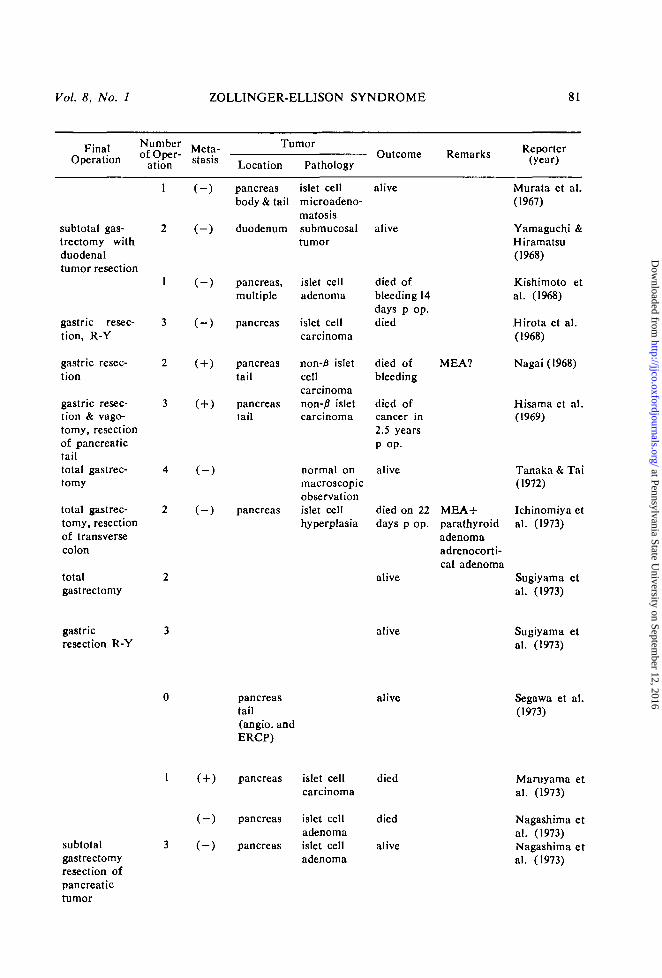
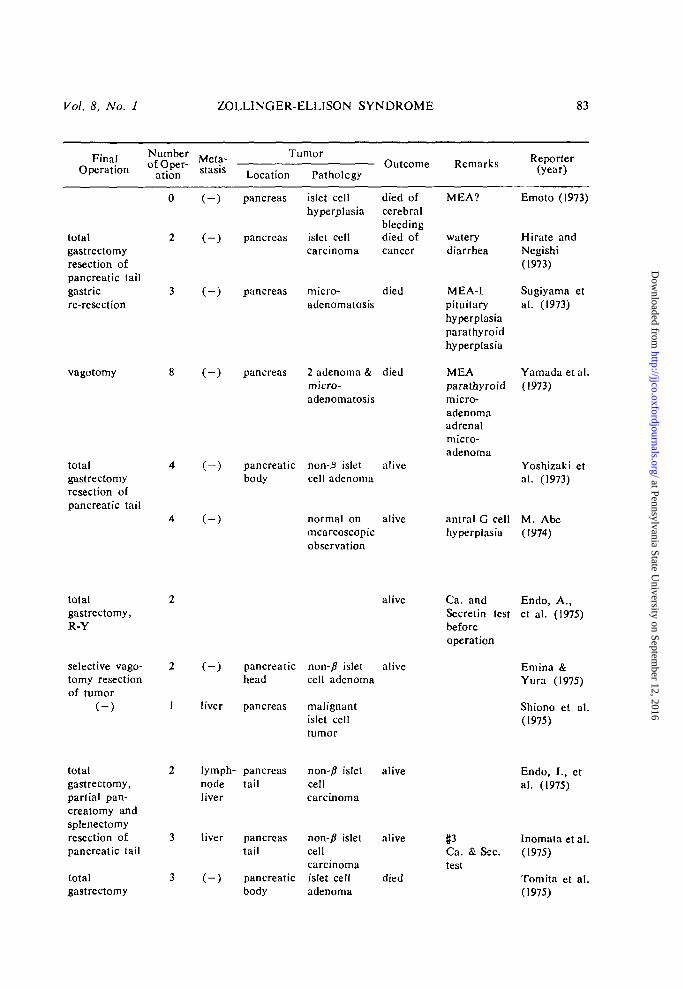
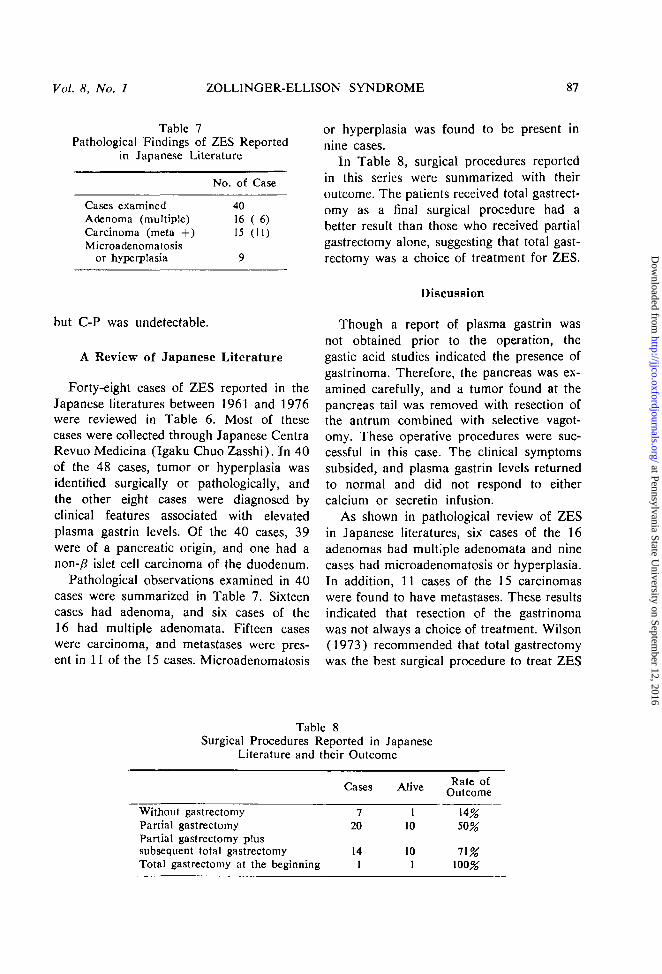
or hyperplasia was found to be present innine cases.
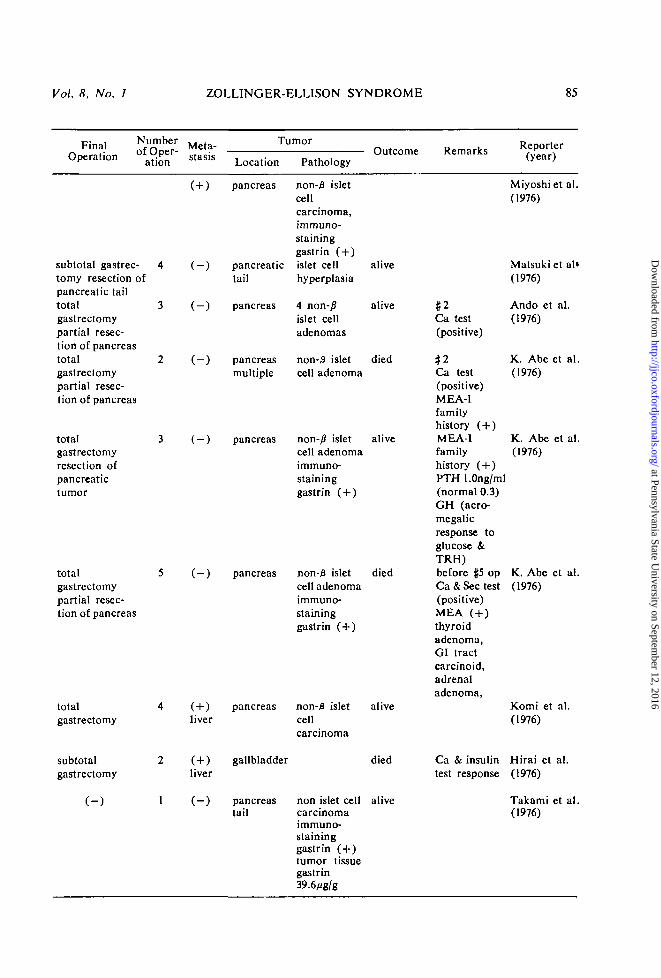
In Table 8, surgical procedures reportedin this series were summarized with theiroutcome. The patients received total gastrect-omy as a final surgical procedure had abetter result than those who received partialgastrectomy alone, suggesting that total gast-rectomy was a choice of treatment for ZES.
but C-P was undetectable.
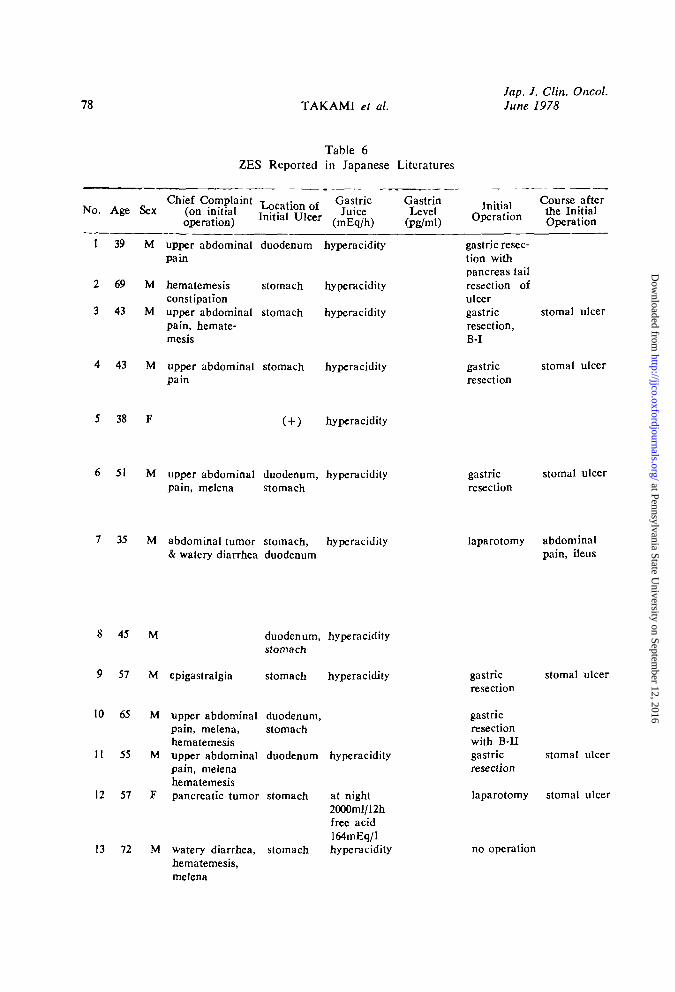
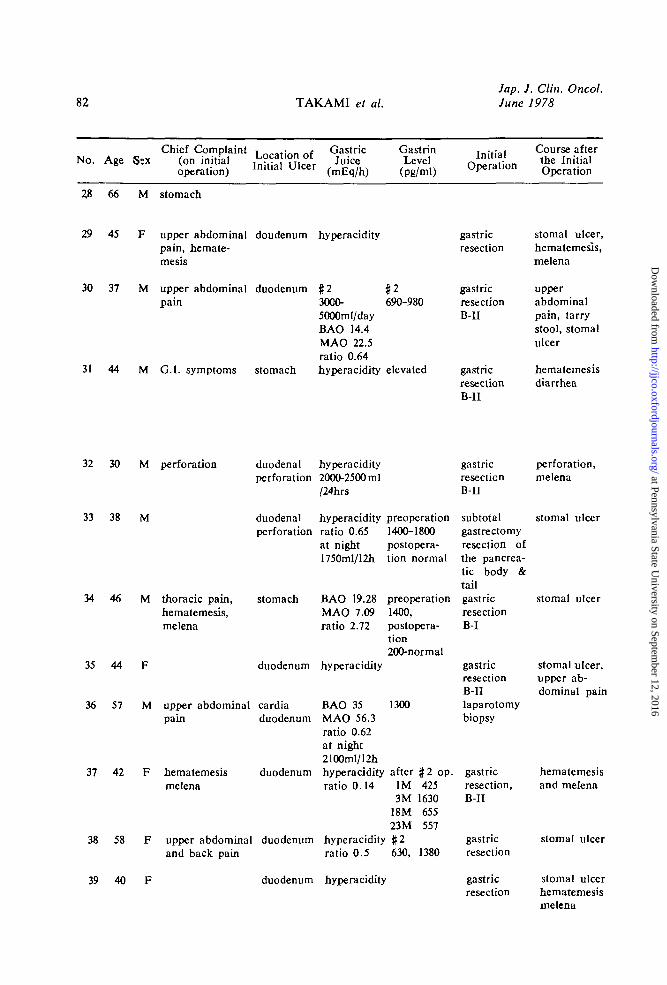
A Review of Japanese Literature
Forty-eight cases of ZES reported in theJapanese literatures between 1961 and 1976were reviewed in Table 6. Most of thesecases were collected through Japanese CentraRevuo Medicina (Igaku Chuo Zasshi). In 40of the 48 cases, tumor or hyperplasia wasidentified surgically or pathologically, andthe other eight cases were diagnosed byclinical features associated with elevatedplasma gastrin levels. Of the 40 cases, 39were of a pancreatic origin, and one had anon-/? islet cell carcinoma of the duodenum.
Pathological observations examined in 40cases were summarized in Table 7. Sixteencases had adenoma, and six cases of the16 had multiple adenomata. Fifteen caseswere carcinoma, and metastases were pres-ent in 11 of the 15 cases. Microadenomatosis
Discussion
Though a report of plasma gastrin wasnot obtained prior to the operation, thegastic acid studies indicated the presence ofgastrinoma. Therefore, the pancreas was ex-amined carefully, and a tumor found at thepancreas tail was removed with resection ofthe antrum combined with selective vagot-omy. These operative procedures were suc-cessful in this case. The clinical symptomssubsided, and plasma gastrin levels returnedto normal and did not respond to eithercalcium or secretin infusion.
As shown in pathological review of ZESin Japanese literatures, six cases of the 16adenomas had multiple adenomata and ninecases had microadenomatosis or hyperplasia.In addition, 11 cases of the 15 carcinomaswere found to have metastases. These resultsindicated that resection of the gastrinomawas not always a choice of treatment. Wilson(1973) recommended that total gastrectomywas the best surgical procedure to treat ZES
Table 8Surgical Procedures Reported in Japanese
Literature and their Outcome
Cases Alive Rate ofOutcome
Without gastrectomyPartial gastrectomyPartial gastrectomy plussubsequent total gastrectomyTotal gastrectomy at the beginning
720
141
110
10
50%
71%100%
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
88 TAKAMI et al.Jap. J. Clin. Oncol.June 1978
from the studies of their registered cases,and our data supported his conclusion.
As for this case, total gastrectomy wasnot performed, and there is a possibility ofrecurrence in the future. Therefore, weare following him carefully. In general, cal-cium and secretin infusion tests are the mostsensitive and reliable method to detect therecurrence of the gastrinoma.
It is interesting to note that this tumortissue was proved to contain immunoreac-tive calcitonin and VIP in addition to largeamounts of gastrin. The immunofluorescencestudy demonstrated the presence of tumorcells contained insulin. These data suggestthat this was a case of multiple hormoneproducing tumor and that large amounts ofgastrin which was produced in the tumortissue evoked the clinical features in thiscase.
References
Abe, K., I. Adachi, K. Yamaguchi, F. Zezeand M. Tanaka, Journal of Clinical Surgery(RINSHO GEKA) 31: 1001, 1976 (in Japa-nese).
Abe, M., N. Nose, S. Yamaoka, A. Murata,T. Maeda and Y. Watanabe, Jap J Gastro-enterol (Tokyo) 64: 1271, 1967 (in Japa-nese).
Abe, M., S. Kidokoro, M. Aoki and K. Sada,Stomach and Intestine (I to CHO) 9: 1265,1974 (in Japanese).
Abe, M., The Journal of Adult Disease (RIN-SHO SEIJINBYO) 4: 303, 1974 (in Japa-nese).
Ando, N., M. Endo, T. Isomoto, Y. Yama-moto, Y. Kinugasa and K. Sano, The Japa-nese Journal of Gastroenterological Surgery(NIPPON SHOKAK1 GEKA GAKKAIZASSHl) 9: 174, 1976 (in Japanese).
Ballard, H. S., B. Frame and R. J. Hartsook,Medicine 43: 481, 1964.
Daikoku, Y., Y. Oguma and Y. Sakai, TheJournal of the Japanese Practical SurgeonSociety (NIPPON RINSHO GEKA IGAK-KAI ZASSHl) 25: 53, 1964 (in Japanese).
Emina, M. and J. Yura, CHUBU GEKAGAKKAI KIROKU 11: 39, 1975 (in Japa-nese).
Emoto, M., Modern Medicine (SAISH1N IGA-
KU) 28: 349, 1973 (in Japanese).Endo, A., K. Kono, T. Yamaguchi and M.
Katsumi, Jap J Gastroenterol (Tokyo) 72:1349, 1975 (in Japanese).
Endo, I., Y. Tadashi, Y. Nohara, H. Nakachi,Y. Miyagi, M. Matayoshi, K. Gengawa, A.Sotoma, N. Nagamine, Y. Sugiura, J. Yogi,S. Nakamatsu, T. Akamatsu, K. Sashima,1. Kondo, K. Iwamura and S. Omata, ClinEndocrinol (Tokyo) 23: 817, 1975 (in Japa-nese).
Hakoda, M., Surgical Therapy (GEKA CHI-RYO) 16: 623, 1967 (in Japanese).
Hamaguchi, H. and N. Komi, Surgical Diag-nosis and Treatment (GEKA SHINRYO) 9:287, 1967 (in Japanese).
Hirai, Y., A. Nakahara, S. Ootomo, S. Shimizu,I. Ooki, S. Nakamura and K. Sato, Gastro-enterological Endoscopy 18 : 357, 1976 (inJapanese).
Hirate, S. and T. Negishi, SA1SEI 533: 27,1973 (in Japanese).
Hirota, K., M. Odaka and K. Nakano, TheJournal of the Japanese Practical SurgeonSociety (NIPPON RINSHO GEKA GAK-KAI ZASSHl) 29: 351, 1968 (in Japanese).
Hisama, S., T. Kasakawa, K. Nishiyama, T.Ookubo and T. Tomita, The Japanese Jour-nal of Gastroenterological Surgery (NIPPONSHOKAK1 GEKA GAKKAI ZASSHl) 1:26, 1969 (in Japanese).
Ichinomiya, G., S. Tonoda, N. Nakamichi, M.Kashiya, Z. Kawaguchi, Y. Kuru, Y. Naka-mura, K. Nagai, M. Emoto and T. Yama-moto, Journal of Clinical Surgery (RINSHOGEKA) 28: 1013, 1973 (in Japanese).
Inomata, Y., S. Aoki, K. Hirai, H. Akimotoand F. Nagao, Jap J Surg (Tokyo) 76: 549,1975 (in Japanese).
Kishimoto, H., S. Shirasawa, I. Sakai, E. Naitoand T. Nakamura, The Journal of the Nago-ya City University Medical Association 19:273, 1968 (in Japanese).
Komi, N., H. Watanabe, T. Kushida, M.Kuramoto, H. Udaka, M. Kinoshita, R.Fujino and M. Takahashi, The JapaneseJournal of Gastroenterological Surgery(NIPPON SHOKAKI GEKA GAKKAIZASSHl) 9: 456, 1976 (in Japanese).
Kozawa, M., Gastroenterological Endoscopy5: 66, 1963 (in Japanese).
Maruyama, I., T. Okuda, H. Kakiuchi andK. Takahara, IGAKU NO AYUMI 84: 139,1973 (in Japanese).
Matsuki, K., T. Fuchimoto, T. Yamasaki, T.Murakami, H. Nishida and Y. Takano,
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from
Vol. 8, No. 1 ZOLLINGER-ELLISON SYNDROME 89
Surgery (GEKA) 38: 840, 1976 (in Japa-nese).
McGuigan, J. E., Gastroenterology 56: 429,1969.
Miyoshi, A. and S. Kishimoto, Diagnosis andTreatment (SHINDAN to CHIRYO) 64: 78,1976 (in Japanese).
Murata, 1., Jap J Gastroenterol (Tokyo) 58:1253, 1961 (in Japanese).
Murata, I., S. Maeda, A. Nakagawa and Y.Daikoku, Jap J Gastroenterol (Tokyo) 62:1428, 1965 (in Japanese).
Murata, I., Y. Hirono and A. Maeda, SurgicalDiagnosis and Treatment (GEKA SHIN-RYO) 9: 983, 1967 (in Japanese).
Nagai, R., The Journal of the Nagoya CityUniversity Medical Association 19: 273,1968 (in Japanese).
Nagashima, R., M. Kimura, K. Miyagawa, M.Watanabe, S. Noguchi, T. Saki and M.Takami, Jap J Surg (Tokyo) 74: 671, 1973(in Japanese).
Oda, M., T. Matsuoka, H. Miyashita, M. Fuji-yama, J. Tsukioka and Y. Koike, / JapSoc Intern Med (Tokyo) 5 5 : 886. 1966 (inJapanese).
Segawa, K., S. Nakazawa, K. Imai, N. Matsuo,Y. Yamamoto and M. Shiobara, Clinic AII-Round (SOGO RINSHO) 22: 2257, 1973(in Japanese).
Shiono, K., H. Sanada, N. Miyaue, S. Ryu, K.Kato, Y. Watanabe and H. Kidokoro, JapJ Gastroenterol (Tokyo) 72 : 1065, 1975 (inJapanese).
Straus, E. and R. S. Yalow, GastrointestinalHormones, a symposium, (edited by Thomp-son, J. C.) University of Texas Press, Austinand London, 99, 1975.
Sugisaki, T., E. Tanaka and M. Saito, / JapSoc Intern Med (Tokyo) 5 6 : 305, 1967 (inJapanese).
Sugiyama, M., K. Sato, K. Shimada, H. Sugita,
K. Nishiyama, T. Fukushima, S. Fujisawa,T. Okubo, S. Tsuchiya, M. Watanabe, N.Ishikawa, R. Kitamura, I. Seika and T.Yamagishi, The Journal of the JapanesePractical Surgeon Society (NIPPON RIN-SHO GEKA IGAKKAI ZASSHI) 34: 469,1973 (in Japanese).
Tanaka, S., Diagnosis and Treatment (SHIN-DAN to CHIRYO) 54: 1289, 1966 (inJapanese).
Tanaka, S. and C. Tai, Diagnosis and Treat-ment (SHINDAN to CHIRYO) 60: 2158,1972 (in Japanese).
Tomita, Y., T. Ito, M. Nachi, A. Goto, T.Miyashita, S. Suzuki, J. Kato and M. Kato,Jap J Surg (Tokyo) 77: 1607, 1975 (inJapanese).
Wilson, S. D., The Pancreas (edited by Carey,L. C ) , C. V. Mosby Co., 259, 1973.
Yalow, R. S. and S. A. Berson, Gastroenterol-ogy 58: 1, 1970.
Yamada, M., M. Tei, N. Sugiyama, T. Saito,A. Goto, H. Kuwakado, M. Ikuta, K.Kazama, F. Sagawa and K. Tashiro, TheJournal of the Showa Medical Association33: 176, 1973 (in Japanese).
Yamaguchi, K., K. Abe, F. Zeze, I. Adachi,M. Tanaka, T. Kameya, H. Kitaoka, K.Kobayashi and M. Sasagawa, Jap J ClinOncol 6: 83, 1976.
Yamaguchi, N. and M. Hiramatsu, The Journalof the Japanese Practical Surgeon Society(NIPPON RINSHO GEKA IGAKKAIZASSHI) 29: 351. 1968 (in Japanese).
Yoshizaki, S., H. Watanabe, N. Aikawa, N.Tokita and N. Watanabe, The Journal ofthe Japanese Practical Surgeon Society(NIPPON RINSHO GEKA IGAKKAIZASSHI) 34: 470, 1973 (in Japanese).
Yoshinaga, T., Journal of Clinical Science(RINSHO KAGAKU) 2: 907, 1966 (inJapanese).
at Pennsylvania State University on Septem
ber 12, 2016http://jjco.oxfordjournals.org/
Dow
nloaded from