2 3 Comparing effectiveness of two anticoagulation management models in a Malaysian tertiary...
10
1 23 International Journal of Clinical Pharmacy International Journal of Clinical Pharmacy and Pharmaceutical Care ISSN 2210-7703 Int J Clin Pharm DOI 10.1007/s11096-013-9796-6 Comparing effectiveness of two anticoagulation management models in a Malaysian tertiary hospital Subramaniam Thanimalai, Asrul Akmal Shafie, Mohamed Azmi Hassali & Jeyaindran Sinnadurai
Transcript of 2 3 Comparing effectiveness of two anticoagulation management models in a Malaysian tertiary...

1 23
International Journal of ClinicalPharmacyInternational Journal of ClinicalPharmacy and Pharmaceutical Care ISSN 2210-7703 Int J Clin PharmDOI 10.1007/s11096-013-9796-6
Comparing effectiveness of twoanticoagulation management models in aMalaysian tertiary hospital
Subramaniam Thanimalai, Asrul AkmalShafie, Mohamed Azmi Hassali &Jeyaindran Sinnadurai

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Science
+Business Media Dordrecht. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you wish
to self-archive your article, please use the
accepted manuscript version for posting on
your own website. You may further deposit
the accepted manuscript version in any
repository, provided it is only made publicly
available 12 months after official publication
or later and provided acknowledgement is
given to the original source of publication
and a link is inserted to the published article
on Springer's website. The link must be
accompanied by the following text: "The final
publication is available at link.springer.com”.

RESEARCH ARTICLE
Comparing effectiveness of two anticoagulation managementmodels in a Malaysian tertiary hospital
Subramaniam Thanimalai • Asrul Akmal Shafie •
Mohamed Azmi Hassali • Jeyaindran Sinnadurai
Received: 21 October 2012 / Accepted: 12 May 2013
� Springer Science+Business Media Dordrecht 2013
Abstract Backgrounds Limited evidence is available
regarding pharmacist managed anticoagulation clinic in the
Southeast Asian region where there is marked difference in
terms of care model, genetic composition and patient
demographics. Objectives This study aimed at comparing
the anticoagulation clinic managed by the pharmacist with
physician advisory and the usual medical care provided in
Kuala Lumpur Hospital (KLH) in terms of anticoagulation
control and adverse outcomes. Setting A 2,302 bedded
government tertiary referral hospital in Malaysia. Methods
A 6-month retrospective cohort study of the effectiveness
of two models of anticoagulation care, the pharmacist
managed anticoagulation clinic which is known as warfarin
medication therapy adherence clinic (WMTAC) and usual
medical clinic (UMC) in KLH was conducted, where a
random number generator was used to recruit patients.
The UMC patients received standard medical care where
they are managed by rotational medical officers in the
physicians’ clinic. As for the WMTAC with physician
advisory, the pharmacist will counsel and review the
patients internationalised normalization ratio at each clinic
visit and also adjust the patients’ warfarin dose accord-
ingly. Patients are referred to physicians if immediate
attention is required. Main outcome measure The main
therapeutic outcome is time in therapeutic range (TTR)
both actual and expanded TTR and thromboembolic and
bleeding complications. Results Each of the WMTAC and
usual medical care recruited 92 patients, which totals to
184 patients. The patient demographics in terms of age,
race and indication of treatment were comparable. At the
end of the 6 months follow-up, patients in the WMTAC
group had significantly higher actual-TTR (65.1 vs.
48.3 %; p \ 0.05) compared to those in usual medical care
group. Rates of admission were 6.5 versus 28.2 events per
100 person-years for the WMTAC and UMC groups,
respectively. Though the bleeding incidences were not
significantly different, it was reduced. Conclusions These
findings will impact local warfarin patient management
services and policies because there was no available evi-
dence supporting the role of pharmacists in the manage-
ment of warfarin patients prior to this study.
Keywords Anticoagulation clinic � Malaysia �Pharmacists � Therapeutic range � Warfarin
Impacts on practice
– Pharmacists in Malaysia can have a clear role in the
management of warfarin therapy in a chronic care
clinic.
– The assistance of pharmacists in managing warfarin
therapy in a clinic in Malaysia improves adherence and
is cost effective.
S. Thanimalai (&)
Kuala Lumpur Hospital, Jln. Pahang, 50586 Kuala Lumpur,
Malaysia
e-mail: [email protected]
S. Thanimalai
Discipline of Social and Administrative Pharmacy,
School of Pharmaceutical Sciences, Universiti Sains Malaysia,
11800 George Town, Penang, Malaysia
A. A. Shafie � M. A. Hassali
School of Pharmaceutical Sciences, Universiti Sains Malaysia,
11800 George Town, Penang, Malaysia
J. Sinnadurai
Department of General Medicine, Kuala Lumpur Hospital,
Jln. Pahang, 50586 Kuala Lumpur, Malaysia
123
Int J Clin Pharm
DOI 10.1007/s11096-013-9796-6
Author's personal copy

Introduction
Warfarin has become the most widely used oral anticoag-
ulant since its introduction in 1954. Due to its pharmaco-
kinetic and pharmacodynamic complexities, the
management of warfarin therapy to obtain an optimal
outcome is a great challenge. Inadequate doses lead to
thromboembolic events, while patients that receive exces-
sive anticoagulation are at risk of bleeding [1, 2]. Multiple
factors have been shown to affect anticoagulation control,
such as warfarin dosage, warfarin dosage preparation, drug
or food interactions, patient compliance, patient knowledge
and the setting of anticoagulation services [3].
The effective management of warfarin therapy requires
a considerable amount of clinician time and resources
because of the need for frequent International Normaliza-
tion Ratio (INR) laboratory tests and dosing adjustments
[4]. Thus, various approaches have been recommended to
improve anticoagulant care. These approaches include
anticoagulation monitoring services, point-of-care testing,
computer decision support systems and patient self-man-
agement [5]. Studies have shown that an anticoagulation
management service that is administered by a pharmacist is
one of the most effective methods for the management of
anticoagulation [6, 7]. Additionally, a meta-analysis has
demonstrated that anticoagulation management services
have improved care, in terms of anticoagulation control,
and reduced thromboembolic and hemorrhagic events. In a
random-effect meta-analysis of randomized controlled tri-
als (RCTs), the group that received pharmacist-supported
warfarin therapy had statistically significant improvements
in the prevention of total bleeding [RR, 0.51; 95 % confi-
dence interval (CI), 0.28–0.94]. However, the effects on
major bleeding (RR, 0.64; 95 % CI, 0.18–2.36), thrombo-
embolic events (RR, 0.79; 95 % CI, 0.33–1.93), mortality
from all causes (RR, 0.93; 95 % CI, 0.41–2.13) and mor-
tality from warfarin-related causes (RR, 0.65; 95 % CI,
0.18–2.42) were not significant [3]. Most of these studies
were conducted in North America or Europe [8, 9]. While
some Asian-based studies are now available, there are
major variations in terms of the healthcare management
system [9–12], and inter-country variations include reim-
bursement policies, prescribing patterns, traditions, opinion
leaders with conflicts of interests, domestic pharmaceutical
production and clinical practice guidelines [13].
The usual medical clinic (UMC) service that is used for
the management of warfarinized patients in Malaysian
government health facilities is a clinic that is run by rota-
tional medical officers and physicians. Patients are seen on
an appointment basis for their follow-up.
To offer comprehensive and focused patient care, the
Pharmaceutical Service Division of the Ministry of Health
Malaysia has initiated the Medication Therapy Adherence
Clinic (MTAC) as part of their ambulatory pharmacy ser-
vices. The pharmacist-managed anticoagulation clinic, or
the Warfarin MTAC (WMTAC), was initiated in Malaysia
in 2005 [14].
Aim of the study
The WMTAC is being introduced in a step-wise manner in
Malaysia. Formal assessments of these clinics are needed
to appraise their value prior to nationwide initiation.
Therefore, this study aims to compare the impact of the
WMTAC service with the UMC service that is provided at
a general medical clinic in terms of anticoagulation control.
Methods
The study subjects were patients who had been indicated
for and treated with chronic warfarin therapy. These
patients had been monitored for at least 6 months at the
Department of General Medicine, Kuala Lumpur Hospital
(KLH), which is a 2300-bedded national referral center in
Malaysia.
Anticoagulation management model in KLH
UMC
At the first clinic visit, patients were seen by a medical
officer for history taking and assessment. During this visit,
the patients received a warfarin record book. At subsequent
follow-ups, the warfarin dose was adjusted by the rota-
tional medical officers according to the patients’ INR. If
there was a marked derangement of the INR, a brief
counseling session was provided by the medical officers.
The patients were also referred to the physician on call for
further review if necessary.
WMTAC
The WMTAC is managed by pharmacists with support
from physicians. A management protocol that was
approved by the Pharmaceutical Services Division, Min-
istry of Health Malaysia, was adopted following discus-
sions between the Head of the Medical Department and the
pharmacists that were involved in the WMTAC. Upon
referral to the WMTAC, all new patients were informed of
the role of the WMTAC in the patients’ anticoagulation
care. The pharmacist then collected a detailed patient his-
tory pertaining to anticoagulation therapy before providing
each patient with an individualized educational session and
an information package. The information package
Int J Clin Pharm
123
Author's personal copy

consisted of a patient education guidebook on warfarin
therapy and a warfarin consumption record sheet spanning
12 months. The education session was conducted accord-
ing to a standard in-house counseling checklist that was
developed by the WMTAC pharmacists. The patients were
counseled on the importance of communicating any chan-
ges in their general health, medications or lifestyle. The
risks and benefits of warfarin, the factors that affect its
efficacy and an awareness of the signs and symptoms of
hemorrhagic and thromboembolic complications were also
addressed. The patients who returned for their subsequent
monitoring appointments were assessed by the pharmacist
according to their INRs and to a standard question list that
was developed by the WMTAC pharmacists. The infor-
mation was then documented and used to determine the
most appropriate warfarin dose and the date of the next
monitoring appointment. Standard questions were used to
assess patient compliance and changes in the patients’
medication, food or lifestyle and to identify adverse drug
events. Another pharmacist in the WMTAC counter-
checked the doses and appointment dates before providing
the patients with their warfarin supply. The patients were
only referred to the physician on call if needed or in cases
of emergencies, as stated in the management protocol [15].
The on-call physician reviewed the prescriptions at the end
of the clinic day, and a discussion was initiated with the
pharmacist if needed. As part of continuous quality assur-
ance, the WMTAC pharmacists also held regular case
discussions to address specific patients or issues that were
in need of attention at the end of the clinic day.
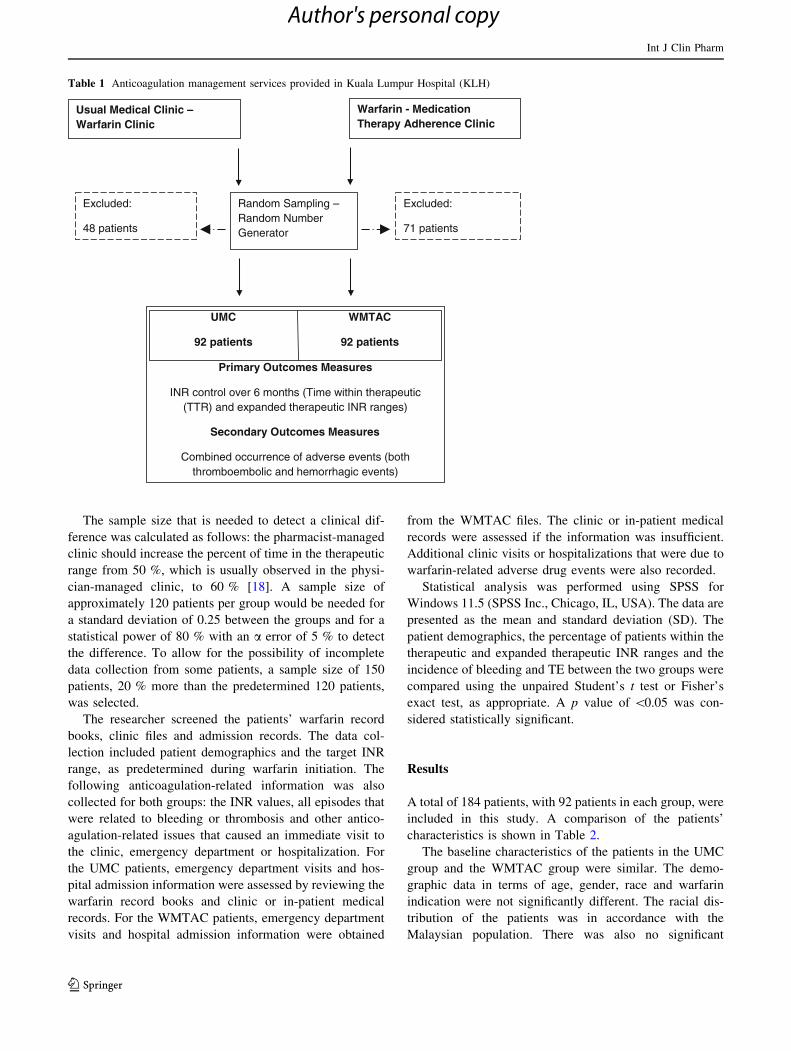
A six-month retrospective cohort study was conducted
to compare the effectiveness of the two anticoagulation
care models, the WMTAC and the UMC. The study design
is illustrated in Table 1. The data for the UMC were col-
lected between January 2008 and January 2011. The
WMTAC was established in the hospital in 2008 and
operated concurrently with the UMC. Data from between
January 2009 and January 2012 were used for the WMTAC
group. Both groups were followed for 6 months from the
initiation of their warfarin therapy.
A web-based random number generator (http://www.
randomizer.org/) was used to generate identifiers for the
patients that were included in this study. These patients
were selected from the list of patients that were enrolled in
both the UMC and the WMTAC. Warfarinized patients
were included if their age was above 18 years and if they
had been managed for at least 6 months in either one of the
clinics. The exclusion criteria that were used were as fol-
lows: patients were excluded if their warfarin indication
was due to anti-phospholipid syndrome, if they were
managed for less than 6 months in one of the care models
or if their medical records were inaccessible due to death or
relocation.
The primary outcome measure was the control of the
INR over 6 months, per proportion of the time within both
the therapeutic (TTR) range and the expanded therapeutic
INR range in the management protocol. The therapeutic
INR ranges for anticoagulation are 2.0–3.0 for prophylaxis
and for the treatment of uncomplicated disease and 2.5–3.5
for patients with mechanical heart valves or for failure with
previous warfarin treatment. These ranges are in accor-
dance with the recommendations of the American College
of Chest Physicians Consensus Conference on Antithrom-
botic Therapy [16]. The therapeutic INR range was
expressed in terms of the proportion of time that the INR
values of the individuals were within the target/therapeutic
INR range. Being at risk for thromboembolic or bleeding
was the outcome that was used as the effectiveness mea-
surement [17]. The expanded therapeutic INR range was
defined as the therapeutic range ±0.2 INR units [11, 18].
This expanded range is not considered clinically important
and would not necessarily require a dosage adjustment
[18]. As described by Rosendaal et al., the percentage of
time that the patients were within the therapeutic and
expanded therapeutic INR ranges was estimated using
linear interpolation between the measured INR values [19].
This method allowed the determination of the optimal
effects of anticoagulation [19] and took into account the
actual number of days in the target range. This method also
enabled the calculation of the INR-specific incidence rates
of adverse events [16].
The secondary outcome measurement that was used was
the combined occurrence of adverse events, including both
thromboembolic and hemorrhagic events. The classifica-
tion criteria for thromboembolic events (TE) were pre-
specified as follows: the severity was categorized as life
threatening if it involved irreversible damage that required
an emergency procedure or admission to an intensive care
unit or as significant if it involved hospitalization or an
emergency visit. The hemorrhagic events were classified
by the site of the bleeding and categorized as life threat-
ening if they resulted in a serious permanent injury or
required surgical or angiographic intervention or as
potentially life threatening if they were associated with 2 of
the following conditions: severe blood loss, hypotension,
which is defined by a C20 mmHg drop in systolic blood
pressure to B90 mmHg, or the requirement of hospital-
ization or an emergency visit. The guidelines suggest a
minimum of 4 weeks between INR assessments for stable
patients [20], with programs often allowing for a maximum
time of 6 weeks between INR assessments [21]. Travelling
costs that are incurred due to monthly clinic visits, which
are often required in cases of unstable INR control, are
known to be burdensome to patients [22]. Thus, in addition
to the above outcomes, the average number of clinic visits
was also measured.
Int J Clin Pharm
123
Author's personal copy
The sample size that is needed to detect a clinical dif-
ference was calculated as follows: the pharmacist-managed
clinic should increase the percent of time in the therapeutic
range from 50 %, which is usually observed in the physi-
cian-managed clinic, to 60 % [18]. A sample size of
approximately 120 patients per group would be needed for
a standard deviation of 0.25 between the groups and for a
statistical power of 80 % with an a error of 5 % to detect
the difference. To allow for the possibility of incomplete
data collection from some patients, a sample size of 150
patients, 20 % more than the predetermined 120 patients,
was selected.
The researcher screened the patients’ warfarin record
books, clinic files and admission records. The data col-
lection included patient demographics and the target INR
range, as predetermined during warfarin initiation. The
following anticoagulation-related information was also
collected for both groups: the INR values, all episodes that
were related to bleeding or thrombosis and other antico-
agulation-related issues that caused an immediate visit to
the clinic, emergency department or hospitalization. For
the UMC patients, emergency department visits and hos-
pital admission information were assessed by reviewing the
warfarin record books and clinic or in-patient medical
records. For the WMTAC patients, emergency department
visits and hospital admission information were obtained
from the WMTAC files. The clinic or in-patient medical
records were assessed if the information was insufficient.
Additional clinic visits or hospitalizations that were due to
warfarin-related adverse drug events were also recorded.
Statistical analysis was performed using SPSS for
Windows 11.5 (SPSS Inc., Chicago, IL, USA). The data are
presented as the mean and standard deviation (SD). The
patient demographics, the percentage of patients within the
therapeutic and expanded therapeutic INR ranges and the
incidence of bleeding and TE between the two groups were
compared using the unpaired Student’s t test or Fisher’s
exact test, as appropriate. A p value of \0.05 was con-
sidered statistically significant.
Results
A total of 184 patients, with 92 patients in each group, were
included in this study. A comparison of the patients’
characteristics is shown in Table 2.
The baseline characteristics of the patients in the UMC
group and the WMTAC group were similar. The demo-
graphic data in terms of age, gender, race and warfarin
indication were not significantly different. The racial dis-
tribution of the patients was in accordance with the
Malaysian population. There was also no significant
Table 1 Anticoagulation management services provided in Kuala Lumpur Hospital (KLH)
Warfarin - Medication Therapy Adherence Clinic
Random Sampling –Random Number Generator
Excluded:
48 patients
Excluded:
71 patients
UMC
92 patients
WMTAC
92 patients
Primary Outcomes Measures
INR control over 6 months (Time within therapeutic (TTR) and expanded therapeutic INR ranges)
Secondary Outcomes Measures
Combined occurrence of adverse events (both thromboembolic and hemorrhagic events)
Usual Medical Clinic –Warfarin Clinic
Int J Clin Pharm
123
Author's personal copy

difference in terms of the smoking status or the alcohol
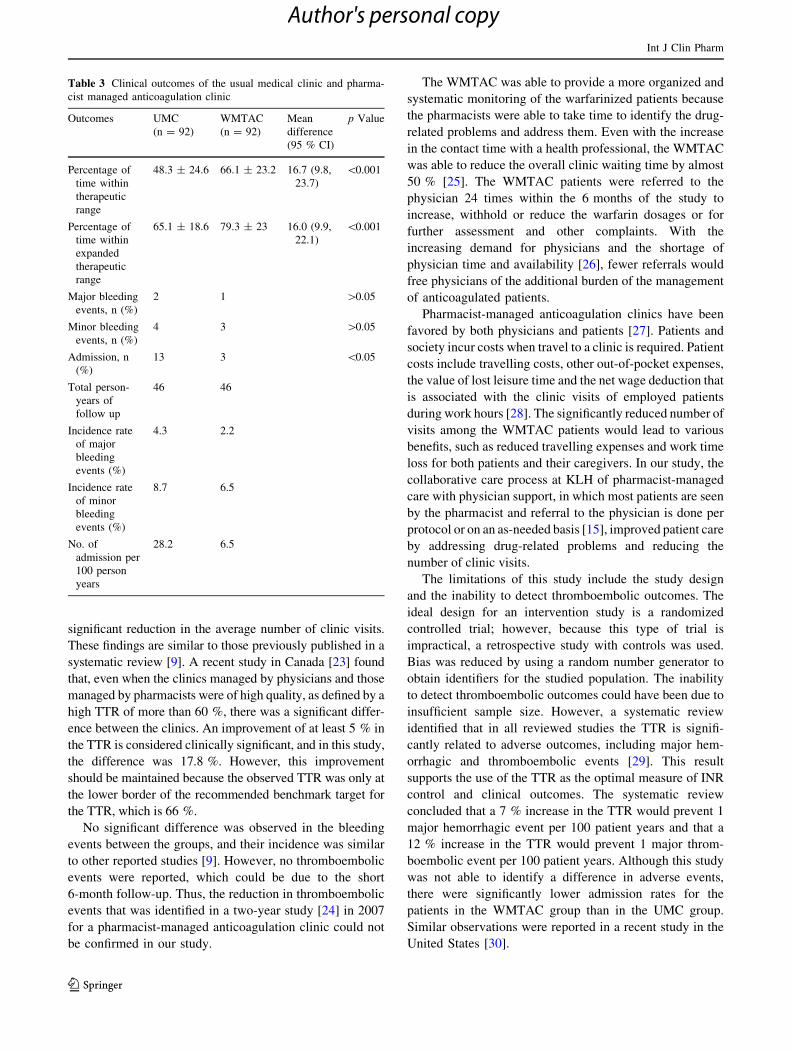
consumption status. As shown in Table 3, the primary
outcome of the TTR was significantly increased in the
WMTAC patients compared with that in the UMC patients
(66.1 vs. 48.3 %; p \ 0.001). The significantly longer TTR
that was observed in the WMTAC group was maintained
even when the expanded therapeutic range was used (79.3
vs. 65.1; p \ 0.001).
The number of admissions was significantly higher
(p = 0.016) among the UMC patients than among the
WMTAC patients. The rates of admission were 6.5 and
28.2 events per 100 person-years for the WMTAC group
and the UMC group, respectively. There were 13 UMC
patient admissions that were due to over-anticoagulation,
and one patient was admitted for suspected thromboem-
bolism. Of the 10 patients that were admitted for over-
anticoagulation, none were classified as life threatening, 1
was classified as potentially life threatening, and the rest
were classified as significant hemorrhagic events. The
admission for probable thromboembolism was classified as
a significant thromboembolic event. Among the over-an-
ticoagulated patients, 2 were admitted for bruises, 2 for
vaginal bleeding, 2 for gum bleeding, 1 for blood in the
urine and 1 for blood in the stool. More than 2 bleeding
sites, such as blood in the urine and vaginal bleeding, were
observed in 2 patients. In the UMC group, another 2
patients were admitted for observation. All 3 WMTAC
patients who were admitted were admitted for over-anti-
coagulation. None of the admitted patients were classified
as life threatening. One patient was classified as potentially
life threatening, and the other 2 were classified as signifi-
cant. One patient had both vaginal and urinary tract
bleeding, 1 patient had bruises, and the other had gum
bleeding. In the WMTAC patients, the incidence of both
major and minor bleeding was lower than that in the UMC
patients; however, this difference was not statistically
significant (p = 1.000 for both).
The average number of clinic visits was significantly
lower for the WMTAC patients (7.9 ± 2.4) than for the
UMC patients (11.2 ± 3.1) (p \ 0.05).
Discussion
The pharmacist-managed anticoagulation clinic, the
WMTAC, has been shown to provide significantly better
anticoagulation control. The individual assessment of the
patients’ INRs and the relevant factors that contribute to
changes in the INRs, if any, by the pharmacist enables the
adjustment of the appropriate dosage. The use of a treatment
protocol also ensures the uniformity and appropriateness of
the treatment. In our study, the introduction of the WMTAC
also led to a reduction in bleeding-related admissions and to a
Table 2 Characteristics of patients from both usual medical clinic
(UMC) and pharmacist managed anticoagulation clinic (WMTAC)
Characteristics UMC
(n = 92)
WMTAC
(n = 92)
p Value
Age, mean (SD) 64.1 (11.9) 63.2 (13.0) 0.600
Gender, n (%) 0.700
Male 48 (52.2) 46 (50)
Female 44 (47.) 46 (50)
Race, n (%) 0.130
Malay 50 (54.3) 53 (57.6)
Chinese 28 (30.4) 33 (35.9)
Indian 13 (14.1) 4 (4.3)
Others 1 (1.1) 2 (2.2)
Warfarin indications, n (%) 0.152
Atrial fibrillation (AF) 80 (87) 70 (76.1)
Mechanical valve
replacement (MVR)
2.2 (2) 4 (4.3)
Aortic valve replacement
(AVR)
1.1 (1) 0 (0)
Deep vein thrombosis (DVT) 1.1 (1) 6 (6.5)
Others 8.7 (8.9) 12 (13)
Co-morbidity (%) 87 (94.6) 84 (91.3) 0.388
Hypertension 59 (64.1) 61 (66.3)
Diabetes mellitus 35 (38) 26 (28.3)
Dyslipidemia 22 (23.9) 23 (25)
Ischemic heart disease 17 (18.5) 17 (18.5)
Stroke 6 (6.5) 3 (3.3)
Thyroid disorder 6 (6.5) 7 (7.6)
Gastro disorder 1 (1.1) 3 (3.3)
Congestive cardiac failure/
heart failure
8 (8.7) 7 (7.6)
Asthma 4 (4.3) 3 (3.3)
CRHD 3 (3.3) 2 (2.2)
Acute coronary syndrome 4 (4.3) 2 (2.2)
Uric acid disorder 2 (2.2) 3 (3.3)
Chronic kidney disease 1 (1.1) 1 (1.1)
Cardiomyopathy 2 (2.2) 3 (3.3)
Mitral regurgitation 2 (2.2) 1 (1.1)
Others 7 (7.6) 11 (12)
Alcohol consumption (%) 0.109
Non consumer 88 (81) 81.5 (75)
Seldom consumer 4.3 (3) 1.1 (1)
Occasional consumer 3.3 (4) 6.5 (6)
Regular consumer 2.2 (2) 0 (0)
High consumer 1.1 (1) 4.3 (4)
Unknown 1.1 (1) 6.5 (6)
Smoker status (%) 0.08
Non-smoker 85.9 (79) 82.6 (76)
Ex-smoker 5.4 (5) 5.4 (5)
Smoker 8.7 (8) 5.4 (5)
Unknown 0 (0) 6.5 (6)
Int J Clin Pharm
123
Author's personal copy
significant reduction in the average number of clinic visits.
These findings are similar to those previously published in a
systematic review [9]. A recent study in Canada [23] found
that, even when the clinics managed by physicians and those
managed by pharmacists were of high quality, as defined by a
high TTR of more than 60 %, there was a significant differ-
ence between the clinics. An improvement of at least 5 % in
the TTR is considered clinically significant, and in this study,
the difference was 17.8 %. However, this improvement
should be maintained because the observed TTR was only at
the lower border of the recommended benchmark target for
the TTR, which is 66 %.
No significant difference was observed in the bleeding
events between the groups, and their incidence was similar
to other reported studies [9]. However, no thromboembolic
events were reported, which could be due to the short
6-month follow-up. Thus, the reduction in thromboembolic
events that was identified in a two-year study [24] in 2007
for a pharmacist-managed anticoagulation clinic could not
be confirmed in our study.
The WMTAC was able to provide a more organized and
systematic monitoring of the warfarinized patients because
the pharmacists were able to take time to identify the drug-
related problems and address them. Even with the increase
in the contact time with a health professional, the WMTAC
was able to reduce the overall clinic waiting time by almost
50 % [25]. The WMTAC patients were referred to the
physician 24 times within the 6 months of the study to
increase, withhold or reduce the warfarin dosages or for
further assessment and other complaints. With the
increasing demand for physicians and the shortage of
physician time and availability [26], fewer referrals would
free physicians of the additional burden of the management
of anticoagulated patients.
Pharmacist-managed anticoagulation clinics have been
favored by both physicians and patients [27]. Patients and
society incur costs when travel to a clinic is required. Patient
costs include travelling costs, other out-of-pocket expenses,
the value of lost leisure time and the net wage deduction that
is associated with the clinic visits of employed patients
during work hours [28]. The significantly reduced number of
visits among the WMTAC patients would lead to various
benefits, such as reduced travelling expenses and work time
loss for both patients and their caregivers. In our study, the
collaborative care process at KLH of pharmacist-managed
care with physician support, in which most patients are seen
by the pharmacist and referral to the physician is done per
protocol or on an as-needed basis [15], improved patient care
by addressing drug-related problems and reducing the
number of clinic visits.
The limitations of this study include the study design
and the inability to detect thromboembolic outcomes. The
ideal design for an intervention study is a randomized
controlled trial; however, because this type of trial is
impractical, a retrospective study with controls was used.
Bias was reduced by using a random number generator to
obtain identifiers for the studied population. The inability
to detect thromboembolic outcomes could have been due to
insufficient sample size. However, a systematic review
identified that in all reviewed studies the TTR is signifi-
cantly related to adverse outcomes, including major hem-
orrhagic and thromboembolic events [29]. This result
supports the use of the TTR as the optimal measure of INR
control and clinical outcomes. The systematic review
concluded that a 7 % increase in the TTR would prevent 1
major hemorrhagic event per 100 patient years and that a
12 % increase in the TTR would prevent 1 major throm-
boembolic event per 100 patient years. Although this study
was not able to identify a difference in adverse events,
there were significantly lower admission rates for the
patients in the WMTAC group than in the UMC group.
Similar observations were reported in a recent study in the
United States [30].
Table 3 Clinical outcomes of the usual medical clinic and pharma-
cist managed anticoagulation clinic
Outcomes UMC
(n = 92)
WMTAC
(n = 92)
Mean
difference
(95 % CI)
p Value
Percentage of
time within
therapeutic
range
48.3 ± 24.6 66.1 ± 23.2 16.7 (9.8,
23.7)
\0.001
Percentage of
time within
expanded
therapeutic
range
65.1 ± 18.6 79.3 ± 23 16.0 (9.9,
22.1)
\0.001
Major bleeding
events, n (%)
2 1 [0.05
Minor bleeding
events, n (%)
4 3 [0.05
Admission, n
(%)
13 3 \0.05
Total person-
years of
follow up
46 46
Incidence rate
of major
bleeding
events (%)
4.3 2.2
Incidence rate
of minor
bleeding
events (%)
8.7 6.5
No. of
admission per
100 person
years
28.2 6.5
Int J Clin Pharm
123
Author's personal copy

The pre-determined sample size was not achieved due to a
temporary change in policy to enroll patients into the
WMTAC after 3 months at the UMC. This change made
patients ineligible to be included in the study because they
have already been treated at the UMC. This temporary
change in policy, which was reverted, interrupted the study;
thus, the intended number of samples could not be attained
within the planned duration of the study recruitment.
Conclusion
This study has shown that the WMTAC resulted in better
anticoagulation care compared with the UMC. These
findings will impact local warfarin patient management
services and policies because there was no available evi-
dence supporting the role of pharmacists in the manage-
ment of warfarin patients prior to this study. Although a
higher cost is expected due the use of pharmacists and the
use of point-of-care testing, future research should evaluate
the cost effectiveness of such services in preventing
adverse events that are associated with warfarin use.
Acknowledgments We would like to acknowledge and thank the
Kuala Lumpur Hospital for granting permission to use the hospital
and its resources to conduct this study. We gratefully acknowledge all
of the hospital staff who contributed to the study and DAWN Clinical
Software for the AC software used to provide the percentage of time
within the therapeutic range calculations.
Funding The research is funded by the University Sains Malaysia,
Research University Grant. The author is sponsored by the Federal
Training Grant, Ministry of Health for post-graduate research.
Conflicts of interest No conflict of interest to declare.
References
1. Pirmohamed M. Warfarin: almost 60 years old and still causing
problems. Br J Clin Pharmacol. 2006;62(5):509–11.
2. Wysowski DK, Nourjah P, Swartz L. Bleeding complications
with warfarin use: a prevalent adverse effect resulting in regu-
latory action. Arch Intern Med. 2007;167(13):1414–9.
3. Saokaew S, Permsuwan U, Chaiyakunapruk N, Nathisuwan S,
Sukonthasarn A. Effectiveness of pharmacist-participated war-
farin therapy management: a systematic review and meta-analy-
sis. J Thromb Haemost. 2010;8(11):2418–27.
4. Sullivan PW, Arant TW, Ellis SL, Ulrich H. The cost effective-
ness of anticoagulation management services for patients with
atrial fibrillation and at high risk of stroke in the US. Pharma-
coeconomics. 2006;24(10):1021–33.
5. Ansell J, Hirsh J, Dalen J, Bussey H, Anderson D, Poller L, et al.
Managing oral anticoagulant therapy. Chest. 2001;119(1 Sup-
pl):22S–38S.
6. Bungard TJ, Gardner L, Archer SL, Hamilton P, Ritchie B,
Tymchak W, et al. Evaluation of a pharmacist-managed antico-
agulation clinic: Improving patient care. Open Med. 2009;3(1):
e16–21.
7. Donovan JL, Drake JA, Whittaker P, Tran MT. Pharmacy-man-
aged anticoagulation: assessment of in-hospital efficacy and
evaluation of financial impact and community acceptance.
J Thromb Thrombolysis. 2006;22(1):23–30.
8. You JH, Chan FW, Wong RS, Cheng G. Cost-effectiveness of
two models of management for patients on chronic warfarin
therapy—a Markov model analysis. Thromb Haemost.
2003;90(6):1106–11.
9. Saokaew S, Sapoo U, Nathisuwan S, Chaiyakunapruk N, Perm-
suwan U. Anticoagulation control of pharmacist-managed col-
laborative care versus usual care in Thailand. Int J Clin Pharm.
2012;34(1):105–12.
10. Choe H, Kim J, Choi K, Mueller B. Implementation of the first
pharmacist-managed ambulatory care anticoagulation clinic in
South Korea. Am J Health-Syst Pharm. 2002;59(9):872–4.
11. Chan FW, Wong RS, Lau WH, Chan TY, Cheng G, You JH.
Management of Chinese patients on warfarin therapy in two
models of anticoagulation service—a prospective randomized
trial. Br J Clin Pharmacol. 2006;62(5):601–9.
12. Kong MC, Ng HJ, Lee PL, Chan YH, Tan D, Lee LH. Imple-
mentation and impact of a hybrid pharmacist-assisted anticoag-
ulation clinic model on the quality of anticoagulation therapy.
Clin Appl Thromb Hemost. 2012;18(3):334–7.
13. Fretheim A, Oxman AD. International variation in prescribing
antihypertensive drugs: its extent and possible explanations.
BMC Health Serv Res. 2005;5(1):21.
14. Government of Malaysia. Pekeliling Perkhidmatan. In: Malaysia
PSDo, editor. Putrajaya; 2007. p. 1–545.
15. Medication Therapy Adherence Clinic. Warfarin. First Edition
2010. Kuala Lumpur: Perpustakaan Negara Malaysia; 2010.
16. Hirsh J, Dalen J, Anderson DR, Poller L, Bussey H, Ansell J,
et al. Oral anticoagulants: mechanism of action, clinical effec-
tiveness, and optimal therapeutic range. Chest. 2001;119(1 Sup-
pl):8S–21S.
17. Fitzmaurice DA, Blann AD, Lip GYH. Bleeding risks of anti-
thrombotic therapy. BMJ. 2002;325(7368):828–31.
18. Wilson SJ-A, Wells PS, Kovacs MJ, Lewis GM, Martin J, Burton
E, et al. Comparing the quality of oral anticoagulant management
by anticoagulation clinics and by family physicians: a random-
ized controlled trial. Can Med Assoc J. 2003;169(4):293–8.
19. Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A
method to determine the optimal intensity of oral anticoagulant
therapy. Thromb Haemost. 1993;69(3):236–9.
20. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G.
Pharmacology and management of the vitamin K antagonists:
American College of chest physicians evidence-based clinical
practice guidelines (8th edition). Chest. 2008;133(6 Suppl):
160S–98S.
21. Chamberlain MA, Sageser NA, Ruiz D. Comparison of antico-
agulation clinic patient outcomes with outcomes from traditional
care in a family medicine clinic. J Am Board Fam Pract.
2001;14(1):16–21.
22. Hwang JM, Clemente J, Sharma KP, Taylor TN, Garwood CL.
Transportation cost of anticoagulation clinic visits in an urban
setting. J Manag Care Pharm. 2011;17(8):635–40.
23. Young S, Bishop L, Twells L, Dillon C, Hawboldt J, O’Shea P.
Comparison of pharmacist managed anticoagulation with usual
medical care in a family medicine clinic. BMC Fam Pract.
2011;12(88):1471–2296.
24. Poon IO, Lal L, Brown EN, Braun UK. The impact of pharma-
cist-managed oral anticoagulation therapy in older veterans.
J Clin Pharm Ther. 2007;32(1):21–9.
25. Thanimalai S CT, Ariffin F, Chan CK, Chan BS, Chong SH,
Heng SY. Achieving INR targets and improving satisfaction of
Warfarinized patients, Kuala Lumpur Hospital. J Quality
Improvement. 2010;2:50–67 [Original Article].
Int J Clin Pharm
123
Author's personal copy

26. Cindy J, Guy L. Enhancing patient care via a pharmacist-man-
aged rural anticoagulation clinic. Healthc Q. 2009;13(Sp):69–74.
27. Lodwick AD, Sajbel TA. Patient and physician satisfaction with a
pharmacist-managed anticoagulation clinic: implications for
managed care organizations. Manag Care. 2000;9(2):47–50.
28. Jowett S, Bryan S, Mahe I, Brieger D, Carlsson J, Kartman B,
et al. A multinational investigation of time and travelling costs in
attending anticoagulation clinics. Value Health. 2008;11(2):
207–12.
29. Wan Y, Heneghan C, Perera R, Roberts N, Hollowell J, Glasziou
P, et al. Anticoagulation control and prediction of adverse events
in patients with atrial fibrillation: a systematic review. Circ
Cardiovasc Quality Outcomes. 2008;1(2):84–91.
30. Rudd KM, Dier JG. Comparison of two different models of
anticoagulation management services with usual medical care.
Pharmacotherapy. 2010;30(4):330–8.
Int J Clin Pharm
123
Author's personal copy