VBAC Uterine Scar Measurement Info_ January 2011
23
7/5/12 VBAC Uterine Scar Measurement Info: January 2011 1/23 thevbacer.blogspot.com/2011_01_01_archive.html FRIDAY, JANUARY 14, 2011 More exchanges with Dr. Rozenberg Here are other questions I sent Dr. Rozenberg that relate to this measurement, and his responses. They provide additional information on the measurement as well as his thoughts as to its helpfulness in predicting uterine rupture. Start at the bottom and work your way up. #4 - Second Response from Dr. Rozenberg Dear [Me] 1)"There have been other studies on this topic [other than yours] and not all are so favorable". > I disagree with this assertion. I enclose you a recent review of studies about this topic. all are corresponding; however, most have biases. 2)"A uterine scar could be thick at 37 weeks and thin at 39 weeks. For that matter, it could be thick at the onset of labor but thin two hours later." > I agree with it. however, our study showed that when the low uterine segment was thick around 37 weeks, the risk of uterine rupture during a trial of labor was very low. Moreover, most of thin low uterine segments are not pathologic. In all, in order to help you to understand : - when the low uterine segment is thick around 37 weeks, it is usually strong - when the low uterine segment is thin around 37 weeks, you can not correctly predict the issue. I hope that my explanations will help you to understand. Give me news when you will be delivered (or before if you have any other questions) sincerely THIS BLOG DOES NOT CONSTITUTE MEDICAL ADVICE! Nothing in this blog is to be construed as medical advice. As with anything else, please consult a licensed health care professional regarding all things discussed in this blog. Note specifically that the information provided on uterine segment measurements is not to be construed as advice from a health care professional, but simply as information a woman can present to her health care professional in the context of deciding upon or planning a VBAC. And as should be obvious, uterine segment measurements are not 100% reliable in predicting uterine rupture, so a VBAC attempt should be undertaken only after a women fully understands all of the risks and benefits and with the knowledge that there is no way to know with absolute surety whether she will be in the small percentage of women who will develop a uterine rupture or other complication. BLOG ARCHIVE ▼ 2011 (3) ▼ January (3) More exchanges with Dr. Rozenberg Berbagi Laporkan Penyalahgunaan Blog Berikut» Buat Blog Masuk VBAC UTERINE SCAR MEASUREMENT INFO
-
Upload
asep-budiman -
Category
Documents
-
view
88 -
download
0
Transcript of VBAC Uterine Scar Measurement Info_ January 2011

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
1/23thevbacer.blogspot.com/2011_01_01_archive.html
F R I D A Y, J A N U A R Y 1 4 , 2 0 1 1
More exchanges with Dr. Rozenberg
Here are other questions I sent Dr. Rozenberg that relate to this
measurement, and his responses. They prov ide additional
information on the measurement as well as his thoughts as to its
helpfulness in predicting uterine rupture. Start at the bottom and
work y our way up.
#4 - Second Response from Dr. Rozenberg
Dear [Me]
1)"There have been other studies on this topic [other than y ours]
and not all are so favorable".
> I disagree with this assertion. I enclose y ou a recent rev iew of
studies about this topic. all are corresponding; however, most
have biases.
2)"A uterine scar could be thick at 37 weeks and thin at 39 weeks.
For that matter, it could be thick at the onset of labor but thin two
hours later."
> I agree with it. however, our study showed that when the low
uterine segment was thick around 37 weeks, the risk of uterine
rupture during a trial of labor was very low. Moreover, most of
thin low uterine segments are not pathologic. In all, in order to
help y ou to understand :
- when the low uterine segment is thick around 37 weeks, it is
usually strong
- when the low uterine segment is thin around 37 weeks, y ou can
not correctly predict the issue.
I hope that my explanations will help y ou to understand. Give me
news when y ou will be delivered (or before if y ou have any other
questions)
sincerely
T H I S B L O G D O E S N O T C O N S T I T U T E
M E D I C A L A D V I C E !
Nothing in this blog is to be
construed as medical adv ice. As
with any thing else, please consult a
licensed health care professional
regarding all things discussed in
this blog. Note specifically that the
information prov ided on uterine
segment measurements is not to be
construed as adv ice from a health
care professional, but simply as
information a woman can present
to her health care professional in
the context of deciding upon or
planning a VBAC. And as should be
obvious, uterine segment
measurements are not 100%
reliable in predicting uterine
rupture, so a VBAC attempt should
be undertaken only after a women
fully understands all of the risks
and benefits and with the
knowledge that there is no way to
know with absolute surety whether
she will be in the small percentage
of women who will develop a
uterine rupture or other
complication.
B L O G A R C H I V E
▼ 2011 (3)
▼ January (3)
More exchanges with Dr.
Rozenberg
Berbagi Laporkan Penyalahgunaan Blog Berikut» Buat Blog Masuk
V B A C U T E R I N E S C A RM E A S U R E M E N T I N F O

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
2/23thevbacer.blogspot.com/2011_01_01_archive.html
patrick
#3 - Second Em ail to Dr. Rozenberg
Dear Dr. Rozenberg,
A few months ago I emailed y ou about y our studies regarding the
connection between the thickness of the LUS and a patient's
chances of uterine rupture during a VBAC attempt. I believe, at
the time, I emailed and thanked y ou for y our prompt and
informative responses, and I'd like to do so again now. If y ou don't
mind indulging me one last time, I'd like to ask y ou one more
question.
After corresponding with y ou, I asked an American doctor, Bruce
Flamm, who has published books and articles on VBAC over here,
why most American doctors don't perform a LUS measurement on
their VBAC patients. His response was this: "There have been other
studies on this topic [other than y ours] and not all are so
favorable. A uterine scar could be thick at 37 weeks and thin at 39
weeks. For that matter, it could be thick at the onset of labor but
thin two hours later."
My question is, do y ou agree with this? I am just a lay person, of
course, but I have read many other studies (accessed through
online journal banks like Pub Med) and they all suggest that
women with a prior cesarean section scar, on average,
consistently have thinner LUS segments than women with
unscarred uteruses. So, I'm tempted to think his response is
incorrect, but I wanted y our opinion.
Thanks again,
[Me]
#2 - Dr. Rozenberg's Response
Dear Leigha
> My question is, do y ou still believe this finding is accurate?
Y es, I do and we practice this examination in our department
before deciding on the mode of delivery with our patients
>If so, why don't more doctors do sonograms to measure this
when they have a VBAC candidate?
I think that most obstetricians feel uncomfortable with the
perspective of legal suits in rare cases of uterine rupture in case of
How to perform lower uterine
segment measurement
Studies on ultrasonographic
measurement of the low...

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
3/23thevbacer.blogspot.com/2011_01_01_archive.html
trial of labour and prefer to perform repeat Cesarean Sections.
Even in France, the LUS measurement is rarely performed.
Sincerely y ours
Patrick
#1 - My first em ail to Dr. Rozenberg
Dear Dr. Rozenberg,
My name is [Me].... I am writing y ou because I had a cesarean
section with my first child in December 2004 because she was
breech, and I am contemplating getting pregnant again soon. I
have been researching in-depth the possibility of hav ing a VBAC
with my next baby . In doing his search, I found an article y ou
wrote in 1996 on how measurements of a woman's lower uterine
segment in the third trimester can predict whether she will suffer a
uterine rupture during a trial of labor. Specifically , y our article
showed that women with a measurement of over 3.5mm are
almost guaranteed not to rupture. This is of great interest to me
because, like many other potential VBAC candidates, I am afraid
to try a VBAC for fear of hav ing a uterine rupture. My question is,
do y ou still believe this finding is accurate? If so, why don't more
doctors do sonograms to measure this when they have a VBAC
candidate? What can I say to my doctor (who I don't think does
this ty pe of measurement) to get him to do it when I'm pregnant?
I'm
pretty convinced by y our findings that I want this ty pe of
measurement done but it just doesn't seem to be done that
commonly over here.
Any advice/encouragement/information is appreciated.
[Me]
POSTED BY LEIGHA AT 12:52 PM 2 COM M ENTS:
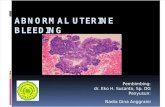
How to perform lower uterine segment
measurement
Here is a description of how one doctor performs a uterine
segment measurement. This information is from Dr. Patrick
Rozenberg, the author of the best studies on the subject. He does it
v ia transabdominal ultrasound (the kind that goes over y our
belly ), but my sonographer actually did it v ia transvaginal

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
4/23thevbacer.blogspot.com/2011_01_01_archive.html
ultrasound because she thought she could get better readings that
way (and, in fact, a later study suggested that she was correct).
I measured a 4mm when my sonographer did it. Dr. Rozenberg's
1996 study on this measurement suggested a cut-off of 3.5mm;
because I had a higher measurement than this, I felt comfortable
going forward with my VBAC attempt.
Here's the link to the description of the 1996 study .
Description of how Dr. Rozenberg perform s the
m easurem ent:
From: [Dr. Rozenberg]
To: [Me]
Sent: Wednesday , August 1 , 2007 12:28:00 PM
Subject: RE how to perform ultrasonographic measurement of the
lower uterine segment
Transabdominal examination
Between 36 and 38 weeks
Full bladder (v isualization of the whole LUS)
Sagittal sections of the LUS
Measure of the thinnest zone (upper third of the LUS)
Calipers at the interface of the bladder and the amniotic fluid-
decidua
(on-to-on)
LUS in an almost horizontal plane
3 measurements (smallest value chosen)
sincerely
PR(See attached file: SI.5.3.jpg)

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
5/23thevbacer.blogspot.com/2011_01_01_archive.html
POSTED BY LEIGHA AT 11:43 AM NO COM M ENTS:
Studies on ultrasonographic measurement of the
lower uterine segment
These are all of the studies I could find on the national medical
studies database, http://www.pubmed.com/, related to the
ultrasonographic measurement of the lower uterine segment on
patients with a prior cesarean section and its success in predicting
uterine rupture/safety of trial of labor. If y ou are an information
junkie like me, these might be helpful in y our decision as to
whether or not to discuss with y our health care professional the
possibility of hav ing this measurement performed.
J Obstet Gy naecol Can. 2010 Apr;32(4):321-7 .
Sonographic lower uterine segm ent thickness and risk of
uterine scar defect: a sy stem atic review.
Jastrow N, Chaillet N, Roberge S, Morency AM, Lacasse Y , Bujold
E.
Department of Obstetrics and Gy naecology , Centre Hospitalier
Universitaire Sainte-Justine, Faculty of Medicine, Université de
Montréal, Montreal QC.
OBJECTIVE: To study the diagnostic accuracy of sonographic
measurements of the lower uterine segment (LUS) thickness near
term in predicting uterine scar defects in women with prior
Caesarean section (CS).

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
6/23thevbacer.blogspot.com/2011_01_01_archive.html
DATA SOURCES: PubMed, Embase, and Cochrane Library (1965-
2009).
METHODS OF STUDY SELECTION: Studies of populations of
women with prev ious low transverse CS who underwent third-
trimester evaluation of LUS thickness were selected. We retrieved
articles in which number of patients, sensitiv ity , and specificity to
predict a uterine scar defect were available.
DATA SY NTHESIS: Twelve eligible studies including 1834 women
were identified. Uterine scar defect was reported in a total of 121
cases (6.6%). Seven studies examined the full LUS thickness only ,
four examined the my ometrial lay er specifically , and one
examined both measurements. Weighted mean differences in LUS
thickness and associated 95% confidence intervals between
women with and without uterine scar defect were calculated.
Summary receiver operating characteristic (SROC) analy sis and
summary diagnostic odds ratios (DOR) were used to evaluate and
compare the area under the curve (AUC) and the association
between LUS thickness and uterine scar defect. Women with a
uterine scar defect had thinner full LUS and thinner my ometrial
lay er (weighted mean difference of 0.98 mm; 95% CI 0.37 to 1 .59,
P = 0.002; and 1 .13 mm; 95% CI 0.32 to 1 .94 mm, P = 0.006,
respectively ). SROC analy sis showed a stronger association
between full LUS thickness and uterine scar defect (AUC: 0.84 +/-
0.03, P < 0.001) than between my ometrial lay er and scar defect
(AUC: 0.7 5 +/- 0.05, P < 0.01). The optimal cut-off value varied
from 2.0 to 3.5 mm for full LUS thickness and from 1 .4 to 2.0 for
my ometrial lay er.
CONCLUSION: Sonographic LUS thickness is a strong predictor for
uterine scar defect in women with prior Caesarean section.
However, because of the heterogeneity of the studies we analy zed,
no ideal cut-off value can y et be recommended, which underlines
the need for more standardized measurement techniques in future
studies.
Arch Gy necol Obstet. 2010 Feb 10.
Sonographic assessm ent of lower uterine segm ent at
term in wom en with previous cesarean delivery .
Kushtagi P, Garepalli S.
KMC Quarters Manipal University Campus, Manipal, 57 6104,
India, [email protected].
OBJECTIVE: To correlate lower uterine segment (LUS) thickness

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
7/23thevbacer.blogspot.com/2011_01_01_archive.html
measured by abdominal sonography at term pregnancy with that
measured manually using caliper at cesarean delivery and to find
out minimum LUS thickness indicative of its integrity in women
with prev ious cesarean.
METHODS: In 106 women with prev ious cesarean delivery and 68
with unscarred uterus, abdominal sonographic assessment of LUS
was carried out within a week of delivery . Sonographic
measurements were correlated with manual measurement of
lower flap of LUS using Vernier calipers in 96 of these women (64
with prev ious cesarean and 32 of unscarred uterus) who had
elective cesarean delivery .
RESULTS: Sonographically determined LUS was thinner among
women with prev ious cesarean delivery than in those without
(4.58 SD 1 .05 vs. 4.8 SD 0.8; t = 1 .986; p = 0.04). Women with
vaginal birth after cesarean had thicker LUS than women with
repeat cesarean delivery (4.4 SD 0.97 vs. 4.48 SD 1 .0). The
findings were not influenced by engaged fetal head status or
amount of bladder fullness. Directly measured LUS thickness using
Vernier calipers before delivery of the baby confirmed ultrasound
measurements, but showed smaller differences between them.
There were eight cases with defective uterine scar at cesarean.
LUS thickness at term of 3 mm provided 87 .5% sensitiv ity and
specificity , and was found to have negative predictive value of
98%. But in two of seven cases the actual LUS was not measurable
despite sonographic measurement of 3 mm, and there were two
records of scar dehiscence in those with 3 and 4 mm of LUS
thickness.
CONCLUSION: LUS thickness of 3 mm measured by abdominal
ultrasonography prior to delivery at term in women with prev ious
cesarean is suggestive of stronger LUS but is not a reliable
safeguard for trial of labor.
Am J Obstet Gy necol. 2009 Sep;201(3):320.e1-6.
Prediction of com plete uterine rupture by sonographic
evaluation of the lower uterine segm ent.
Bujold E, Jastrow N, Simoneau J, Brunet S, Gauthier RJ.
Department of Obstetrics and Gy naecology , Faculty of Medicine,
Centre de recherche du Centre hospitalier universitaire de
Québec, Université Laval, Québec, QC, Canada.
OBJECTIVE: The purpose of this study was to establish the validity

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
8/23thevbacer.blogspot.com/2011_01_01_archive.html
of sonographic evaluation of lower uterine segment (LUS)
thickness for complete uterine rupture.
STUDY DESIGN: A prospective cohort study of women with
prev ious cesarean delivery was conducted. LUS thickness (full
thickness and my ometrial thickness only ) was measured between
35 and 38 weeks gestation, and the thinnest measurement was
considered to be the dependent variable. Receiver operating
curve analy ses and logistic regression were used.
RESULTS: Two hundred thirty -six women were included in the
study . Nine uterine scar defects (3 cases of complete rupture
during a trial of labor and 6 cases of dehiscence) were reported.
Receiver operating curve analy ses showed that full thickness of
<2.3 mm was the optimal cutoff for the prediction of uterine
rupture (3/33 vs 0/92; P = .02). Full thickness was also identified
as an independent predictor of uterine scar defect (odds ratio,
4.66; 95% confidence interval, 1 .04-20.91)
CONCLUSION: Full LUS thickness of <2.3 mm is associated with a
higher risk of complete uterine rupture.
Int J Gy naecol Obstet. 2009 Nov;107 (2):140-2. Epub
2009 Aug 13.
Com parison of transabdom inal versus transvaginal
ultrasound to m easure thickness of the lower uterine
segm ent at term .
Marasinghe JP, Senanay ake H, Randeniy a C, Seneviratne HR,
Arambepola C, Dev lieger R.
University Obstetrics and Gy necology Unit, De Soy za Hospital for
Women, Colombo, Sri Lanka. jeevanmarasinghe@y ahoo.com
OBJECTIVE: To compare the accuracy of transvaginal (TVS)
versus transabdominal (TAS) ultrasound to assess the thickness of
the lower uterine segment (LUS).
METHODS: Eighty -three pregnant women admitted for an elective
cesarean delivery were enrolled. LUS thickness was measured
using both TVS and TAS prior to the cesarean. The actual
thickness of the LUS was measured using a sterile metal ruler after
the neonate had been delivered.
RESULTS: Seventeen women had unscarred uteri (20.1%); 41 had
had one prev ious cesarean (49.4%); and 25 had had two prev ious
cesareans (30.1%). Mean thickness of the LUS measured after

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
9/23thevbacer.blogspot.com/2011_01_01_archive.html
delivery was 7 .58+/-1 .3 mm in unscarred uteri; 5.09+/-1 .4 mm
for one cesarean; and 3.92+/-1 .1 mm for two cesareans (P<0.01).
Actual thickness of the LUS showed a significant correlation with
TVS among the total (r(s)=0.89); with unscarred uteri (r(s)=0.68);
with 1 cesarean (r(s)=0.89); and 2 cesareans (r(s)=0.68), while
with TAS the correlations were significant only with the total
(r(s)=0.53) and 2 prev ious cesareans (r(s)=0.63) (P<0.01).
CONCLUSION: TVS is a more accurate method of assessing the
thickness of the LUS compared with TAS.
Ultrasound Obstet Gy necol. 2009 Mar;33(3):301-6.
Lower uterine segm ent thickness m easurem ent in
pregnant wom en with previous Cesarean section:
reliability analy sis using two- and three-dim ensional
transabdom inal and transvaginal ultrasound.
Martins WP, Barra DA, Gallarreta FM, Nastri CO, Filho FM.
Departamento de Ginecologia e Obstetrícia da Faculdade de
Medicina de Ribeirão Preto, Universidade de São Paulo and Escola
de Ultra-sonografia de Ribeirão Preto, Ribeirão Preto, São Paulo,
Brazil. [email protected]
OBJECTIVE: To evaluate the reliability of two- and three-
dimensional ultrasonographic measurement of the thickness of
the lower uterine segment (LUS) in pregnant women by
transvaginal and transabdominal approaches.
METHODS: This was a study of 30 pregnant women who had had at
least one prev ious Cesarean section and were between 36 and 39
weeks' gestation, with singleton pregnancies in cephalic
presentation. Sonographic examinations were performed by two
observers using both 4-7 -MHz transabdominal and 5-8-MHz
transvaginal volumetric probes. LUS measurements were
performed using two- and three-dimensional ultrasound,
evaluating the entire LUS thickness transabdominally and the LUS
muscular thickness transvaginally . Each observer measured the
LUS four times by each method. Reliability was analy zed by
comparing the mean of the absolute differences, the intraclass
correlation coefficients, the 95% limits of agreement and the
proportion of differences < 1 mm.
RESULTS: Transvaginal ultrasound prov ided greater reliability in
LUS measurements than did transabdominal ultrasound. The use
of three-dimensional ultrasound improved significantly the
reliability of the LUS muscular thickness measurement obtained

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
10/23thevbacer.blogspot.com/2011_01_01_archive.html
transvaginally .
CONCLUSIONS: Ultrasonographic measurement of the LUS
muscular thickness transvaginally appears more reliable than
does that of the entire LUS thickness transabdominally . The use of
three-dimensional ultrasound should be considered to improve
measurement reliability .
Gy necol Obstet Fertil. 2005 Dec;33(12):1003-8.
T he counselling of patient with prior C-section.
Rozenberg P.
Departement de gy necologie-obstetrique, centre hospitalier de
Poissy --Saint-Germain, universite Versailles-Saint-Quentin,
France. prozenberg@chi-poissy -st-germain.fr
A trial of labor after prior cesarean delivery is associated with a
greater perinatal risk than is elective repeated cesarean delivery
without labor, although absolute risks are low. Information and
counselling aim to estimate specific risks and to balance these
risks according to indiv idual factors. Therefore, the phy sician has
to answer two questions: (i) which would be the probability of
successful vaginal delivery ? (ii) which would be the risk of uterine
rupture with a trial of labor? The risk factors for failure of trial of
labor are: increased maternal age, obesity , and fetal macrosomia.
The risk factors for uterine rupture are: increased maternal age,
postpartum fever after the prev ious cesarean delivery , short
interdelivery interval, history of at least two prev ious cesarean
deliveries, and a history of classical incision. Conversely , other
factors are of good prognosis: a prior vaginal delivery and,
particularly , a prior VBAC (Vaginal Birth After Caesarean) are
associated with a higher rate of successful trial of labor compared
with patients with no prior vaginal delivery ; ultrasonographic
measurement of the lower uterine segment thickness>3.5 mm has
an excellent negative predictive value for the risk of uterine
defect. Finally , the wish for additional pregnancies following a
cesarean section must be considered as an argument in favour of a
trial of labor after accounting for the increasing risks correlated
with repeated elective cesarean deliveries.
J Obstet Gy naecol Can. 2005 Jul;27 (7 ):67 4-81.
Sonographic m easurem ent of the lower uterine segm ent
thickness in wom en with previous caesarean section.
Cheung VY .
Department of Obstetrics and Gy naecology , North Y ork General
Hospital, Toronto, ON.

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
11/23thevbacer.blogspot.com/2011_01_01_archive.html
OBJECTIVES: To evaluate the accuracy of prenatal sonography in
determining the lower uterine segment (LUS) thickness in women
with prev ious Caesarean section and to assess the usefulness of
measuring LUS thickness in predicting the risk of uterine rupture
during a trial of vaginal birth.
METHODS: Sonographic examination was performed in 102
pregnant women with one or more prev ious Caesarean sections at
between 36 and 38 weeks' gestation to assess the LUS thickness,
which was defined as the shortest distance between the urinary
bladder wall-my ometrium interface and the
my ometrium/chorioamniotic membrane-amniotic fluid interface.
Of the 102 women examined, 91 (89.2%) had transabdominal
sonography only , and 11 (10.8%) had both transabdominal and
transvaginal examinations. The sonographic measurements were
correlated with the delivery outcome and the intraoperative LUS
appearance.
RESULTS: The mean sonographic LUS thickness was 1 .8 mm,
standard dev iation (SD) 1 .1 mm. An intraoperatively diagnosed
paper-thin or dehisced LUS, when compared with an LUS of
normal thickness, had a significantly smaller sonographic LUS
measurement (0.9 mm, SD 0.5 mm, vs. 2.0 mm, SD 0.8 mm,
respectively ; P < 0.0001). Two women had uterine dehiscence,
both of whom had prenatal LUS thickness of < 1 mm. Thirty -two
women (31 .4%) had a successful vaginal delivery , with a mean LUS
thickness of 1 .9 mm, SD 1 .5 mm; none had clinical uterine rupture.
A sonographic LUS thickness of 1 .5 mm had a sensitiv ity of 88.9%,
a specificity of 59.5%, a positive predictive value of 32.0%, and a
negative predictive value of 96.2% in predicting a paper-thin or
dehisced LUS.
CONCLUSIONS: Sonography permits accurate assessment of the
LUS thickness in women with prev ious Caesarean section and
therefore can potentially be used to predict the risk of uterine
rupture during trial of vaginal birth.
Int J Gy naecol Obstet. 2004 Dec;87 (3):215-9.
Ultrasonographic evaluation of lower uterine segm ent
thickness in patients of previous cesarean section.
Sen S, Malik S, Salhan S. Department of Obstetrics and Gy necology ,
Vardhman Mahavir Medical College and Safdarjung Hospital, New
Delhi, India. dr_sumana_sen@y ahoo.com

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
12/23thevbacer.blogspot.com/2011_01_01_archive.html
OBJECTIVE: To evaluate by ultrasonography , the lower uterine
segment thickness of women with a prev ious cesarean delivery
and determine a critical thickness above which safe vaginal
delivery is predictable.
METHODS: A prospective observational study of 7 1 antenatal
women with prev ious cesarean delivery and 50 controls was
carried out. Transabdominal and transvaginal ultrasonography
were used in both groups to evaluate lower uterine segment
thickness. The obstetric outcome in patients with successful
vaginal birth and intraoperative findings in women undergoing
cesarean delivery were correlated with lower segment thickness.
RESULTS: The overall vaginal birth after cesarean section (VBAC)
was 46.5% and VBAC success rate was 63.5%, the incidence of
dehiscence was 2.82%, and there were no uterine ruptures. There
was a 96% correlation between transabdominal ultrasonography
with magnification and transvaginal ultrasonography . The critical
cutoff value for safe lower segment thickness, derived from the
receiver operator characteristic curve, was 2.5 mm.
CONCLUSION: Ultrasonographic evaluation permits better
assessment of the risk of scar complication intrapartum, and could
allow for safer management of delivery .
J Ultrasound Med. 2004 Jul;23(7 ):907 -11; quiz 913-4.
Second-trim ester sonographic com parison of the lower
uterine segm ent in pregnant wom en with and without a
previous cesarean delivery .
Sambaziotis H, Conway C, Figueroa R, Elimian A, Garry D.
Department of Obstetrics, Gy necology , and Reproductive
Medicine, State University of New Y ork Health Sciences Center at
Stony Brook, Stony Brook, New Y ork 117 94, USA.
OBJECTIVE: To compare measurements of the lower uterine
segment during a second-trimester sonographic examination in
women with and without a prev ious cesarean delivery .
METHODS: Women undergoing second-trimester sonographic
examination, 24 with a history of cesarean delivery and 30
control subjects with no history of cesarean delivery , were
recruited for transvaginal sonographic evaluation of the lower
uterine segment with a high-frequency probe. The uterine niche or
prev ious cesarean scar site was defined as a small triangular
anechoic defect in the anterior wall of the uterus. The uterine wall

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
13/23thevbacer.blogspot.com/2011_01_01_archive.html
thickness was measured successively at the level where the
bladder dome meets the lower uterine segment. Measurements
were obtained with cursors at the interface of the urine-bladder
and the amniotic fluid-decidua. The study was approved by the
Institutional Rev iew Board, and P < .05 was considered
significant.
RESULTS: The uterine niche was identified in 14 (58%) of 24
women with a prev ious cesarean delivery . The lower uterine
segment was significantly thinner in women with a prev ious
cesarean delivery compared with control subjects (mean +/- SD,
4.7 +/- 1 .1 versus 6.6 +/- 2.0 mm; P < .001). In the prev ious
cesarean group, the mean lower uterine segment thickness was
similar in the 5 women with 2 cesarean deliveries when compared
with those with 1 cesarean delivery (4.6 +/- 1 .0 versus 4.7 +/- 1 .4
mm; P = .91). In a linear regression model, the only variable
retaining significance in the prediction of uterine wall thickness
was prev ious cesarean delivery (P= .002). Maternal age, parity ,
number of prev ious cesarean deliveries, and gestational age did
not attain significance in the model.
CONCLUSIONS: The lower uterine segment during a second-
trimester sonographic examination is significantly thinner in
women with a prev ious cesarean delivery . Identification of the
scar niche is possible in most of these women.
J Ultrasound Med 23:1441-1447 (2004)
Sonographic Evaluation of the Lower Uterine Segm ent in
Patients With Previous Cesarean Delivery .
Cheung, V., Constantinescu, O., Ahluwalia, B. Department of
Obstetrics and Gy necology , North Y ork General Hospital,
Toronto, Ontario, Canada (V.Y .T.C.); and BSA Diagnostic Imaging,
Toronto, Ontario, Canada (O.C.C., B.S.A.), vcheung@ny gh.on.ca.
Objective. To evaluate the appearance of the lower uterine
segment (LUS) in pregnant women with prev ious cesarean
delivery and to compare the LUS thickness with that in women
with unscarred uteri.
Methods. In a prospective study , sonographic examination was
performed on 53 pregnant women with prev ious cesarean
delivery (cesarean group), 40 nulliparas (nullip-control), and 40
women who had 1 or more childbirths with unscarred uteri
(multip-control) between 36 and 38 weeks’ gestation to assess the
appearance and compare the thickness of the LUS. In the cesarean

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
14/23thevbacer.blogspot.com/2011_01_01_archive.html
group, the sonographic findings were correlated with the delivery
outcome and the intraoperative LUS appearance.
Results. In the cesarean group, 44 patients (83.0%) had a normal-
appearing LUS indistinguishable from that of control groups; 2
patients (3.8%) had an LUS defect suggestive of dehiscence; and 7
patients (13.2%) had thickened areas of increased echogenicity
with or without my ometrial thinning. Although the cesarean
group had a thinner LUS (1 .9 ± 1 .4 mm) when compared with both
the nullip-control group (2.3 ± 1 .1 mm; P > .05) and the multip-
control group (3.4 ± 2.2 mm; P < .001), only the latter difference
achieved statistical significance. One of the 2 patients who had a
sonographically suspected LUS defect had confirmed uterine
dehiscence during surgery . An intraoperatively diagnosed paper-
thin LUS, when compared with an LUS of normal thickness, had
significantly smaller sonographic LUS measurements (1 .1 ± 0.6
versus 2.0 ± 0.8 mm, respectively ; P = .004).
Conclusions. Prior cesarean delivery is associated with a
sonographically thinner LUS when compared with those with
prior vaginal delivery . Prenatal sonographic examination is
potentially capable of diagnosing a uterine defect and determining
the degree of LUS thinning in patients with prev ious cesarean
delivery .
Aust N Z J Obstet Gy naecol. 2000 Nov;40(4):402-4.
Preoperative diagnosis of dehiscence of the lower uterine
segm ent in patients with a single previous Caesarean
section.
Suzuki S, Sawa R, Y oney ama Y , Asakura H, Araki T.
Department of Obstetrics and Gy necology , Nippon Medical
School, Toky o, Japan.
Preoperative diagnoses were checked during surgery in 39
patients who underwent elective repeat Caesarean section with (n
= 20) and without (as control, n = 19) a preoperative diagnosis of
wall dehiscence (thinning) of the lower uterine segment (LUS). All
patients were examined manually and by ultrasonography at 36
weeks gestation before labour. A preoperative diagnosis of wall
dehiscence was made when the wall thickness was less than 2 mm
and/or the patient felt pain and tenderness in the LUS. Surgical
findings of dehiscence were defined as a subperitoneal separation
of the uterine scar in the LUS. The sensitiv ity and specificity of our
ultrasonographic evaluations were found to be 100% and 83% (p <
0.05), respectively . On the other hand, there were no surgical

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
15/23thevbacer.blogspot.com/2011_01_01_archive.html
findings of dehiscence in patients who felt pain and tenderness in
the LUS with a wall thickness greater than 2 mm, nor among those
in the control group.
J Nippon Med Sch. 2000 Oct;67 (5):352-6.
Prediction of uterine dehiscence by m easuring lower
uterine segm ent thickness prior to the onset of labor:
evaluation by transvaginal ultrasonography .
Asakura H, Nakai A, Ishikawa G, Suzuki S, Araki T. Department of
Obstetrics and Gy necology , Nippon Medical School, Sedagi,
Toky o, Japan. asakura [email protected]
OBJECTIVE: Lower uterine segment thickness was measured by
transvaginal ultrasound examination and its correlations with the
occurrence of uterine dehiscence and rupture was examined.
METHODS: The thickness of the muscular lay er of the lower
uterine segment was measured in 186 term grav idas with prev ious
uterine scars and its correlation with uterine dehiscence/rupture
was investigated.
RESULTS: Uterine dehiscence was found in 9 cases or 4.7 %. There
were no cases of the uterine rupture. The thickness of the lower
uterine segment among the grav idas with dehiscence was
significantly less in than those without dehiscence (p< 0.01). The
cut-off value for the thickness of the lower uterine segment was 1 .6
mm as calculated by the receiver operating characteristic curve.
The sensitiv ity was 7 7 .8%; specificity 88.6%; positive predictive
value 25.9%; negative predictive value 98.7 %.
CONCLUSION: Measurement of the lower uterine segment is useful
in predicting the absence of dehiscence among grav idas with
prev ious cesarean section. If the thickness of the lower uterine
segment is more than 1 .6 mm, the possibility of dehiscence during
the subsequent trials of labor is very small.
Obstet Gy necol. 2000 Apr;95(4):596-600.
Predicting incom plete uterine rupture with vaginal
sonography during the late second trim ester in wom en
with prior cesarean.
Gotoh H, Masuzaki H, Y oshida A, Y oshimura S, Miy amura T,
Ishimaru T. Department of Obstetrics and Gy necology , Nagasaki
University School of Medicine, Nagasaki, Japan.
OBJECTIVE: To evaluate the usefulness of serial transvaginal

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
16/23thevbacer.blogspot.com/2011_01_01_archive.html
ultrasonographic measurement of the thickness of the lower
uterine segment in the late second trimester for predicting the risk
of intrapartum incomplete uterine rupture in women with
prev ious cesarean delivery .
METHODS: Serial transvaginal ultrasonography with full bladder
was performed in 37 4 women without prev ious cesarean delivery
(control group) and 348 women with prev ious cesarean delivery
(cesarean group) from 19 to 39 weeks' gestation. The thickness of
the lower uterine segment was measured in the longitudinal plane
of the cerv ical canal.
RESULTS: The thickness of the lower uterine segment decreased
from 6.7 +/- 2.4 mm (mean +/- standard dev iation [SD]) at 19
weeks' gestation to 3.0 +/- 0.7 mm at 39 weeks' gestation in the
control group, but the thickness was more than 2.0 mm
throughout this period in each control subject. In the cesarean
group, the thickness decreased from 6.8 +/- 2.3 mm at 19 weeks'
to 2.1 +/- 0.7 mm at 39 weeks' gestation and was significantly
thinner than that of the control group after 27 weeks' gestation (P
<.05). Eleven of 12 women (91%) with lower uterine segment less
than the mean control - 1 SD in the late second trimester had a
very thin lower uterine segment at cesarean delivery with fetal
hair being v isible through the amniotic membrane, ie, incomplete
uterine rupture. In 17 of 23 women (7 4%) with lower uterine
segment less than 2.0 mm in thickness within 1 week (4 +/- 3 day s)
before repeat cesarean delivery , intrapartum incomplete uterine
rupture developed.
CONCLUSION: Transvaginal ultrasonography is useful for
measurement of the uterine wall after prev ious cesarean delivery .
Eur J Obstet Gy necol Reprod Biol. 1999 Nov;87 (1):39-45.
T hickness of the lower uterine segm ent: its influence in
the m anagem ent of patients with previous cesarean
sections.
Rozenberg P, Goffinet F, Philippe HJ, Nisand I. Department of
Gy necology and Obstetrics, Poissy Hospital, University Paris V,
France. gy nobs.poissy @wanadoo.fr
OBJECTIVE: To determine how ultrasound measurement of the
lower uterine segment affects the decision about delivery for
patients with prev ious cesarean sections (CS) and what are the
consequences on cesarean section rates and uterine rupture or
dehiscence.

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
17/23thevbacer.blogspot.com/2011_01_01_archive.html
PATIENTS: 198 patients: all women with a prev ious CS who gave
birth in our department during 1995 and 1996 to an infant with a
gestational age of at least 36 weeks and who underwent ultrasound
measurement of their lower uterine segment (95-96 study group),
compared with a similar population from 1989 to 1994 whose
measurements were not prov ided to the treating obstetrician.
RESULTS: Among the patients with one prev ious CS, the vaginal
delivery rate did not differ significantly during the two periods
(7 0.3% for the 89-94 study period vs. 67 .9% for the 95-96 study
period, P=0.53), but the 95-96 study group experienced a
significant increase in the rate of elective CS, compensated by a
reduction in the rate of emergency CS (6.3% and 23.4%,
respectively , for the 89-94 study period vs. 11 .9% and 20.1% for
the 95-96 study period, P=0.01). There was a very significant
increase in the rate of vaginal delivery for the 95-96 study period
among patients with two prev ious CS (26.7 % vs. 8.0% for the 89-
95 study period, P=0.01). The lower uterine segment was
significantly thicker among women with a trial of labor than
among those with an elective CS (4.5+/-1 .4 mm compared with
3.8 +/- 1 .5 mm; P=0.006); and the trial of labor group contained
significantly fewer women with a lower uterine segment
measurement less than 3.5 mm than did the elective CS group
(24.0% compared with 56.6%; P<0.001). Two patients (0.8%)
were found to have a defect of the uterine scar, a rate significantly
lower than that observed in the early group (3.9%, P=0.03).
CONCLUSIONS: Ultrasound measurement of the lower uterine
segment can increase the safe use of trial of labor, because it
prov ides an additional element for assessing the risk of uterine
rupture.
Minerva Ginecol. 1999 Apr;51(4):107 -12.
T ransvaginal ultrasonic evaluation of the thickness of
the section of the uterine wall in previous cesarean
sections.Montanari L, Alfei A, Drovanti A, Lepadatu C, Lorenzi D,
Facchini D, Iervasi MT, Sampaolo P.
Istituto di Clinica Ostetrica e Ginecologica, Universita degli Studi,
IRCCS San Matteo, Pav ia, Italy .
BACKGROUND: The aim of this study is to evaluate accuracy of
transvaginal sonographic examination of the lower uterine
segment in pregnant women with prev ious cesarean section.

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
18/23thevbacer.blogspot.com/2011_01_01_archive.html
METHODS: Sixty -one pregnant women between 37 and 40 weeks
of gestation, with prev ious cesarean section underwent
transvaginal ultrasonography . Wall thickness of the lower uterine
segment, the length of cerv ix , dilation of the isthmus uteri were
measured. On the basis of the surgical findings (in 53 patients) and
outcome of the trial of labor (in 8 patients) a Score was assigned to
the pregnant women: Score 1 to the women who had good healing
or a trial of labor without complications; Score 2 to the women
with a thin or discontinued scar and in case of threatened rupture
of the uterus in the trial of labor.
RESULTS: The mean thickness of the lower uterine segment is 3.82
mm +/- 0.99 mm. The Score 1 group shows a mean thickness of
4.2 mm +/- 2.5 mm, and the Score 2 group a mean thickness of 2.8
mm +/- 1 .06 mm. The transvaginal sonographic examination
provides a sensitiv ity and a specificity respectively of 100 and
7 5%, for a thickness cut-off of 3.5 mm, and a positive and negative
predictive values of 60.7 % and 100% respectively .
CONCLUSIONS: The transvaginal sonographic evaluation of the
lower uterine segment improves therefore the obstetrical
decision-making regarding the trial of labor in women with
prev ious cesarean section.
T ohoku J Exp Med. 1997 Sep;183(1):55-65.
Ultrasonographic evaluation of lower uterine segm ent to
predict the integrity and quality of cesarean scar during
pregnancy : a prospective study .
Qureshi B, Inafuku K, Oshima K, Masamoto H, Kanazawa K.
Department of Obstetrics and Gy necology , School of Medicine,
University of the Ry uky us, Okinawa, Japan.
A prospective randomized study was conducted to measure the
serial thickness of the lower uterine segment (LUS) by
transvaginal ultrasonography in a control group of 80 women
having no history of uterine surgery and in a study group of 43
women having a history of prev ious cesarean section (C/S). In the
study group, more than 2 mm of thickness of the LUS was
considered as good healing and less than 2 mm of thickness as
poor healing. After serial sonographic examination, the women
with good healing were given trial for labor unless an obstetrical
indication for C/S existed. The appearance of the LUS during
surgery was compared with antenatal ultrasonographic
assessment by direct inspection. Twenty two (7 9%) of 28 women
with a well healed scar had trial labor with the result that 46% had

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
19/23thevbacer.blogspot.com/2011_01_01_archive.html
a successful vaginal birth without any uterine rupture of
dehiscence. Eight women with poor healing all had elective C/S.
Seven women with a 2 mm LUS thickness were indiv idually
categorized for delivery mode. Two of those women delivered
vaginally . The LUS was found to be thin to translucent in these
later two groups. Two mm or less as a criterion for poor healing
had the sensitiv ity and specificity of 86.7 % and 100%
respectively . The positive predictive value was 100% and the
negative predictive value was 86.7 %. Ultrasonographic evaluation
is effective in predicting the quality of a uterine scar and in
differentiating the risk group of probable uterine rupture from the
non risk group.
J Clin Ultrasound. 1996 Sep;24(7 ):355-7 .
Sonographic evaluation of the wall thickness of the lower
uterine segm ent in patients with previous cesarean
section.
Tanik A, Ustun C, Cil E, Arslan A.
Radiology Department, 19 May is University , Samsun, Turkey .
In pregnant women with a history of cesarean section, wall
thickness of the lower uterine segment may help determine the
risk and safety of vaginal delivery . Determination of wall thickness
may help identify the potential risk of uterine rupture in pregnant
women who do not wish to have another cesarean section or who
are not eligible for surgery due to other sy stemic disorders. In this
study , 50 pregnant women with prev ious cesarean sections were
evaluated with ultrasound preoperatively , and measurements of
the lower uterine segment wall thickness were compared with
intraoperative assessment of uterine thinning. These findings
correlated highly with each other (sensitiv ity : 100%; specificity :
82% positive predictive value: 87 %; negative predictive value:
100%), suggesting the reliability and safety of ultrasound in
evaluating uterine wall thickness.
Zhonghua Fu Chan Ke Za Zhi. 1994 Aug;29(8):458-60,
508-9.
Detection of uterine scar defect during pregnancy by
ultrasonics.
Y ang TZ, Li WZ.
Second Affiliated Hospital, West China University of Medical
Science, Chengdu.
B ty pe ultrasonography was used to observe the formation of
lower uterine segment in 7 1 primigrav ide and the status of lower

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
20/23thevbacer.blogspot.com/2011_01_01_archive.html
uterine segment scar in 31 multiparae with prev ious cesarean
section (CS), from the 33 to 41 gestational week. Results showed
that the lower uterine segments was formed in all 102 cases after
the 33rd week. Compared with the primigrav ide, the lower uterine
segment in the CS group was longer, thinner and not as wide after
the 37 th gestational week. Defective scars of the lower uterine
segment were found in 7 cases of the CS group and 2 of them were
diagnosed as threatened dehiscence owing to the fetal sac
protruding from the scar site. Condition of all these cases were
confirmed during operation. The present study suggested that B
ultrasonic scar can be a helpful and noninvasive method for
detecting scar defect in the lower uterine segment following CS.
Lancet. 1996 Feb 3;347 (8997 ):281-4.
Ultrasonographic m easurem ent of lower uterine
segm ent to assess risk of defects of scarred uterus.
Rozenberg P, Goffinet F, Phillippe HJ, Nisand I.
Department of Obstetrics and Gy naecology , Centre Hospitalier
Intercommunal, Leon Touhladjian, Poissy , France.
BACKGROUND: Ultrasonography has been used to examine the
scarred uterus in women who have had prev ious caesarean
sections in an attempt to assess the risk of rupture of the scar
during subsequent labour. The predictive value of such
measurements has not been adequately assessed, however. We
aimed to evaluate the usefulness of sonographic measurement of
the lower uterine segment before labour in predicting the risk of
intrapartum uterine rupture.
METHODS: In this prospective observational study , the
obstetricians were not told the ultrasonographic findings and did
not use them to make decisions about ty pe of delivery . Eligible
patients were those with prev ious caesarean sections booked for
delivery at our hospital. 642 patients underwent ultrasound
examination at 36-38 weeks' gestation, and were allocated to four
groups according to the thickness of the lower uterine segment.
Ultrasonographic findings were compared with those of phy sical
examination at delivery .
FINDINGS: The overall frequency of defective scars was 4.0% (15
ruptures, 10 dehiscences). The frequency of defects rose as the
thickness of the lower uterine segment decreased: there were no
defects among 27 8 women with measurements greater than 4.5
mm, three (2%) among 17 7 women with values of 3.6-4.5 mm, 14
(10%) among 136 women with values of 2.6-3.5 mm, and eight

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
21/23thevbacer.blogspot.com/2011_01_01_archive.html
(16%) among 51 women with values of 1 .6-2.5 mm. With a cut-off
value of 3.5 mm, the sensitiv ity of ultrasonographic measurement
was 88.0%, the specificity 7 3.2%, positive predictive value 11 .8%,
and negative predictive value 99.3%.
INTERPRETATION: Our results show that the risk of a defective
scar is directly related to the degree of thinning of the lower
uterine segment at around 37 weeks of pregnancy . The high
negative predictive value of the method may encourage
obstetricians in hospitals where routine repeat elective caesarean
is the norm to offer a trial of labour to patients with a thickness
value of 3.5 mm or greater.
Arch Gy necol Obstet. 1991;248(3):129-38.
Ultrasound exam ination of caesarean section scars
during pregnancy .
Fukuda M, Shimizu T, Ihara Y , Fukuda K, Natsuy ama E, Mochizuki
M.
Fukuda Ladies Clinic, Ako, Japan.
Two hundred and sixteen transverse caesarean section scars were
examined sonographically near term by a conventional method
(17 5 scars) and a new method (41 scars). The new method
consisted of obtaining a transabdominal longitudinal scan by the
conventional method and also by a 3M conductor, a
transabdominal frontal scan to give a surface v iew of the scar, and
transperineal and transvaginal longitudinal scans. The new
method was used from 16 weeks of gestation onwards. Of 41 scars
scanned by the new method, 31 showed good healing, being more
than 2 mm in thickness throughout; 10 scars showed poor healing
with a thickness of less than 2 mm and loss of continuity . Of 31
patients with good healing, 8 delivered vaginally and the
remaining 23 patients had repeat caesarean sections for other
obstetric indications. All patients with ultrasound ev idence of
poor healing had repeat caesarean sections. At operation the
thickness of the lower uterine segment was measured with
ophthalmic calipers. There were 4 false negative results (4/83:
4.8%) and 1 false positive result (1/43: 2.3%) with conventional
ultrasound and no false positives or false negatives with the new
method.
Arch Gy necol Obstet. 1988;243(4):221-4.
Exam ination of previous caesarean section scars by
ultrasound.
Fukuda M, Fukuda K, Mochizuki M.

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
22/23thevbacer.blogspot.com/2011_01_01_archive.html
Fukuda Ladies Clinic, Ako, Japan.
We examined 84 lower segment caesarean section scars by
ultrasonography near term. Seventy scars showed good healing
with a thickness of the lower uterine segment of more than 3 mm;
14 scars showed poor healing with a thickness of less than 2 mm
and loss of continuity . Among 7 0 patients with good healing, 24
patients delivered vaginally but the remaining 46 patients have
had repeat caesarean sections for other obstetric indications.
Intraoperative findings in these 46 patients were as follows: Grade
I (no thinning of the lower uterine segment), 42; Grade II
(thinning and loss of continuity of the lower uterine segment but
fetal hair not v isible), 4; Grade III (thinning of the lower uterine
segment and fetal hair v isible), 0. Fourteen patients with poor
healing had repeat caesarean sections. Intraoperative findings in
these 14 patients were as follows: Grade I, 0; Grade II, 9; Grade
III, 5. These results indicate that ultrasound examination detect
thinning of the lower uterine segment and may help to determine
management.
Obstet Gy necol. 1988 Jan;7 1(1):112-20.
Ultrasound diagnosis of defects in the scarred lower
uterine segm ent during pregnancy .
Michaels WH, Thompson HO, Boutt A, Schreiber FR, Michaels SL,
Karo J.
Department of Obstetrics and Gy necology , Prov idence Hospital,
Southfield, Michigan.
A prospective study was begun using ultrasound to diagnose
defects in the lower uterine segment. Seventy patients were
examined and delivered by cesarean section, including 58 at risk
because of prev ious cesarean section and 12 nulliparous controls
not at risk. Of the at-risk patients, 12 had confirmed defects, for an
incidence of 20.7 %. All the controls were normal. The false-
positive rate for at-risk patients was 7 .1%, and the positive and
negative predictive values were 92.3 and 100%, respectively . For
the diagnosed cases, the sonographic lower uterine segment
seemed to form earlier (P less than .01) and was thinner (P less
than .01) than that in the negative cases or the controls. Although
our study design was observational and did not allow us to test the
performance of the lower uterine segment when a defect was
found, we discuss the use of a three-stage classification sy stem to
assist in identify ing sonographically detected defects in a future
trial of labor protocol. We conclude that sonographic surveillance
is a reliable and practical means of evaluating the lower uterine

7/5/12 VBAC Uterine Scar Measurement Info: January 2011
23/23thevbacer.blogspot.com/2011_01_01_archive.html
Newer Posts
segment after conception and before labor or delivery .
POSTED BY LEIGHA AT 11:32 AM NO COM M ENTS:
Home
Subscribe to: Posts (Atom)