
Presentasi Kasus Bayi Sehat
8
CASE PRESENTATION & CLINICAL GUIDELINE APRIL 20 BAYI SEHAT DR ADOLFINA VITRIA Consultant: CASE A. PATIENT’S IDENTITY Name : GOF Sex : Female Age : 26 month Height : 81 cm Weight : 10 kg Marital status : Single Occupation : - Pregnancy status* : - Address : Bantul Examination date : 15 April 2013 B. ANAMNESIS 1. CHIEF COMPLAINT : Datang ke Posyandu untuk penimbangan rutin 2. CURRENT HISTORY : Anak tidak dalam kondisi sakit. Pola makan saat ini cukup baik (makan besar : pagi, siang, sore; camilan : kadang sebelum makan siang, kadang saat sore hari; buah : selang-seling dengan camilan). Saat ini anak sudah dapat berjalan dengan lancar bahkan sudah berlari, dapat berdiri dengan satu kaki kira-kira 1 detik. Sudah dapat bermain-main sendiri, mencoret-coret. Sudah dapat diajak berkomunikasi meski kata-kata yang diucapkannya terkadang sulit dimengerti tapi sudah spesifik. Anak tampak aktif sulit untuk diajak duduk lama. 3. PAST HISTORY : Riwayat kelahiran : lahir secara caesar terencana saat cukup bulan (kurang 2 minggu dari HPL) karena kata dokter tidak mau masuk panggul Riwayat imunisasi : mendapatkan imunisasi dasar lengkap : Hepatitis B saat lahir, usia 2, 3 dan 4 bulan; BCG: saat usia 1 bulan; Polio saat usia 2,3,4 dan 10 bulan; DPT: saat usia 2,3, dan 4 bulan; Campak : saat usia 10 bulan. Riwayat perkembangan : menurut ibu masih sesuai dengan anak lain, hanya anak terlihat lebih banyak gerak dan sulit tidur. Merangkak usia 8 bulan. Berdiri usia 15 bulan. Riwayat sakit : anak tidak pernah mondok di rumah sakit. Beberapa kali sakit demam kadang disertai batuk, pilek. Dapat sembuh setelah berobat ke Puskesmas. Tidak ada riwayat kejang saat demam. 4. SYSTEM a. Cerebrospinal : None b. Cardiovascular : None c. Respiratory : Dyspnoe -, cough -, d. Gastrointestinal : Nauseous -, vomiting-, dyspepsia-. e. Urogenital : Urine clear, polyuria-, dysuria-. f. Musculoskeletal : None g. Integument : Lymph nodes : none h. Eye : none
-
Upload
fina-adolfina -
Category
Documents
-
view
224 -
download
0
Transcript of Presentasi Kasus Bayi Sehat
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 1/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 1
APRIL 20
BAYI SEHATDR ADOLFINA VITRIA
Consultant:
CASE
A. PATIENT’S IDENTITY
Name : GOF
Sex : Female
Age : 26 month
Height : 81 cm
Weight : 10 kg
Marital status : Single
Occupation : -
Pregnancy status* : -
Address : Bantul
Examination date : 15 April 2013
B. ANAMNESIS
1. CHIEF COMPLAINT : Datang ke Posyandu untuk penimbangan rutin
2. CURRENT HISTORY :
Anak tidak dalam kondisi sakit. Pola makan saat ini cukup baik (makan besar : pagi,
siang, sore; camilan : kadang sebelum makan siang, kadang saat sore hari; buah :
selang-seling dengan camilan). Saat ini anak sudah dapat berjalan dengan lancarbahkan sudah berlari, dapat berdiri dengan satu kaki kira-kira 1 detik. Sudah dapat
bermain-main sendiri, mencoret-coret. Sudah dapat diajak berkomunikasi meski
kata-kata yang diucapkannya terkadang sulit dimengerti tapi sudah spesifik. Anak
tampak aktif sulit untuk diajak duduk lama.
3. PAST HISTORY :
Riwayat kelahiran : lahir secara caesar terencana saat cukup bulan (kurang 2
minggu dari HPL) karena kata dokter tidak mau masuk panggul
Riwayat imunisasi : mendapatkan imunisasi dasar lengkap : Hepatitis B saat lahir,
usia 2, 3 dan 4 bulan; BCG: saat usia 1 bulan; Polio saat usia 2,3,4 dan 10 bulan; DPT:
saat usia 2,3, dan 4 bulan; Campak : saat usia 10 bulan.Riwayat perkembangan : menurut ibu masih sesuai dengan anak lain, hanya anak
terlihat lebih banyak gerak dan sulit tidur. Merangkak usia 8 bulan. Berdiri usia 15
bulan.
Riwayat sakit : anak tidak pernah mondok di rumah sakit. Beberapa kali sakit
demam kadang disertai batuk, pilek. Dapat sembuh setelah berobat ke Puskesmas.
Tidak ada riwayat kejang saat demam.
4. SYSTEM
a. Cerebrospinal : None
b. Cardiovascular : None
c. Respiratory : Dyspnoe -, cough -,
d. Gastrointestinal : Nauseous -, vomiting-, dyspepsia-.
e. Urogenital : Urine clear, polyuria-, dysuria-.
f. Musculoskeletal : None
g. Integument : Lymph nodes : none
h. Eye : none
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 2/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 2
APRIL 20
i. ENT : None
5. FAMILY ILLNESS HISTORY :
Riwayat darah tinggi dalam keluarga : kakek dari pihak ayah
Tidak ada riwayat sakit gula. Tidak ada riwayat sakit jantung. Tidak ada riwayat
sakit asma. Tidak ada riwayat sakit berat pada keluarga.
Riwayat alergi : ayah (biduren), tante (biduren) dan kakek (dari garis keturunan
ayah)
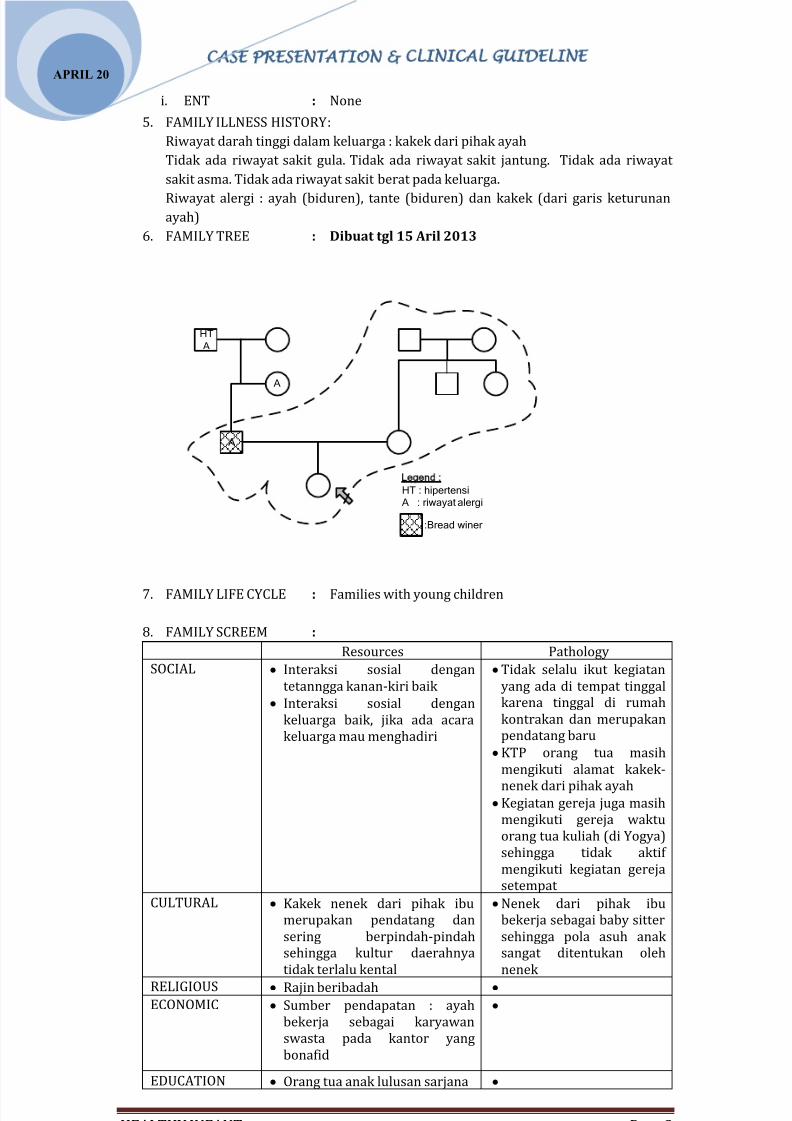
6. FAMILY TREE : Dibuat tgl 15 Aril 2013
HT
A
A
A
Legend :
HT:hipertensi
A:riwayatalergi
:Breadwiner
7. FAMILY LIFE CYCLE : Families with young children
8. FAMILY SCREEM :
Resources Pathology
SOCIAL Interaksi sosial dengan
tetanngga kanan-kiri baik
Interaksi sosial dengan
keluarga baik, jika ada acara
keluarga mau menghadiri
Tidak selalu ikut kegiatan
yang ada di tempat tinggal
karena tinggal di rumah
kontrakan dan merupakan
pendatang baru
KTP orang tua masih
mengikuti alamat kakek-
nenek dari pihak ayah Kegiatan gereja juga masih
mengikuti gereja waktu
orang tua kuliah (di Yogya)
sehingga tidak aktif
mengikuti kegiatan gereja
setempat
CULTURAL Kakek nenek dari pihak ibu
merupakan pendatang dan
sering berpindah-pindah
sehingga kultur daerahnya
tidak terlalu kental
Nenek dari pihak ibu
bekerja sebagai baby sitter
sehingga pola asuh anak
sangat ditentukan oleh
nenek
RELIGIOUS Rajin beribadah ECONOMIC Sumber pendapatan : ayah
bekerja sebagai karyawan
swasta pada kantor yang
bonafid
EDUCATION Orang tua anak lulusan sarjana
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 3/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 3
APRIL 20
MEDICAL Ayah ikut dalam jamsostek,
beitu juga ibu dan anak
Tetapi lebih sering datang ke
Puskesmas
Jika berobat ke Puskesmas
tidak dapat menggunakan
Jamsostek
C. PHYSICAL EXAMINATION
1. General Appearance : Sehat, aktif bergerak
2. Vital Signs
BP
RR
HR
T
:
:
:
:
-
30, regular
80, regular, strong.
36.5 0t
3. Nutritional status
Weight/Age
Height/Age
:
:
:
BB : 10, TB 81, umur 26 bulan
Sesuai umur
Sesuai umur
4. Head : symmetric, haematoma -, conj : not pale
Neck : lymph node : -, JVP: normal, thyroid: not
palpable/,
Thorax : Symmetric, , no retraction
Cardiac : Ictus cordis :normal, S1-S2, murmur : negative,
HR: 67/mnt, regular, pulse strong
Pulmonary : Symmetric, , sonor +/+.no wheezing/rales
Abdomen : protuberance, tympani, tenderness : neg,
peristaltic + normal.
Extremity : Simetrik, hangat, kekuatan baik,
D. ADJUNCT EXAMINATIONS
1. Blood test : -
2. Urinalysis : -
3. Stool examination : -
4. Rontgen : -
5. Other examination : Menilai konsentrasi anak : anak masih dapat
forkus pada satu hal selama kurang lebih 3
menit. Anak diajak bicara masih
memperhatikan yang mengajak bicara
E. DIAGNOSIS (HOLISTIC DIAGNOSIS)
Bayi sehat, dengan pertumbuhan dan perkembangan sesuai umur pada keluarga baru.
F. THERAPY
-
G. PATIENT EDUCATION AND COUNSELING
EDUCATION : -
COUNSELING :
Mengatakan kepada orangtua anak bahwa pertumbuhan dan perkembangan anak
sudah sesuai umum. Pola makan juga sudah baik, meskipun akan lebih baik jika
buah diberikan setiap hari.
Terkait dengan banyaknya aktivitas anak, masih dalam batas normal.
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 4/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 4
APRIL 20
Mengatakan kepada orang tua untuk terus memantau perkembangan anak di
Posyandu
H. MONITORING :
Pengukuran pertumbuhan anak dan memantau perkembangan anak setiap bulan di
Posyandu
I. PROGNOSIS : baik
J. SHORT TERM PLAN: -
K. LONG - TERM PLAN:
a. Targets and Commitments of Care-Plan: untuk selalu datang ke Posyandu
b. Family Empowerment: keluarga harus selalu memperhatikan pertumbuhan dan
perkembangan anak
L. FIVE LEVEL OF PREVENTION :
PRIMARY PREVENTION
HEALTH PROMOTION : Pemberian makanan 4 sehat 5 sempurna
Makan besar 3 kali. Diantaranya buah dan
camilan.
SPESICIF PROTECTION : -
SECONDARY PREVENTION :
EARLY DIAGNOSIS &
PROMPT TREATMENT :
Segera ke puskesmas jika anak sakit atau
ibu merasa ada gangguan tumbang
DISABILITY LIMITATION : -
TERTIARY PREVENTION : -
DISCUSSION
Self Raising Questions
1. Q : apa kriteria untuk anak hiperaktif?
2. Q :apa sajakah yang perlu diperiksa pada anak sehat?
3. Q :untuk memantau perkembangan anak paling mudah dan cepat menggunakan
kriteria apa?
4. Q : kapan dokter umum merujuk pada dokter spesialis terkait dengan
kemungkinan hiperaktif?
5. Q : kapan dokter umum merujuk pada dokter spesialis terkait dengan gizi
buruk?
6.
Q : kapan dokter umum merujuk pada dokter spesialis terkait denganketerlambatan perkembangan?
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 5/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 5
APRIL 20
CLINICAL GUIDELINE
HEALTH SUPERVISION: 2 YEARS
1. ALLOANAMNESIS WITH PARENTS
THIS KIND OF QUESTIONS :
How are you?
How are things going in your family?
Do you have any questions or concerns about your child?
What do you and your partner enjoy most about him/her? What seems to be
most difficult?
Have there been any major changes or stresses in your family since your last
visit?
How is your child toilet training progressing?
What are your child sleeping habits? Eating habits?
Do you think your child hears all right? Sees all right?
Does your child eat nonfood substances such as clay, dirt, or paint chips?
What language(s) does your family speak at home?
Is your child fastened securely in a safety seat in the back seat every time he rides
in the car?
Are you happy with your child care arrangements?
Do both parents and all caregivers agree on disciplinary style and setting limits?
How are you dealing with setting limits for your child and disciplining her?
How do you deal with tantrums?
Do you ever get so angry with your child that you are worried about what you
might do next?
Do you know how to reduce your child’s risk of exposure to lead hazards if you
live in an older home or one that has been renovated recently?
Have you ever been in a relationship where you have been hurt, threatened, or
treated badly?
Have you ever been worried that someone was going to hurt your child? Has your
child ever been abused?
Do you feel safe in your neighborhood?
2. DEVELOPMENTAL SURVEILLANCE AND MILESTONES
ASK THIS KIND OF QUESTIONS
Do you have any specific concerns about your child development or behavior?
How does your child communicate what he wants?
o Vocalizes and gestures
o Speaks words (rapidly expanding vocabulary)
o Uses phrases of two or three words
o Speaks intelligibly to strangers (25 percent of the time)
What do you think your child understands?
o Names of family members
o Names of familiar objects, including those in pictures
o Names of seven body parts
o Simple instructions without gestured cues (“sit down”)
How does your child get from one place to another?
o Walks, climbs, runs
o Goes up and down stairs (one step at a time)
o How does Lincoln act around family members?
o Responsive or withdrawn
o Affectionate or hostile/aggressive
7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 6/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 6
APRIL 20
o Cooperative or defiant
o Dependent or self-reliant
o Anxious when separated from parents
How does your child react to strangers?
o Outgoing or slow to warm up
o Cautious/resistant o How does Lincoln act around other children?
o Interactive or withdrawn/resistant
o Friendly or hostile/aggressive (hitting, biting)
To what extent has your child developed independence in eating and dressing?
o Uses cup, spoon, and fork
o Helps to dress himself
o Tell me about your child s typical play.
o Plays with favorite toys (describe how used)
o Listens to stories
o Engages in simple fantasy playo Engages in parallel play with peers
o Has manual dexterity
3. OBSERVATION OF PARENT-CHILD
Interaction
How do the parent and child communicate? (Parents vary in their awareness of
language
milestones and the ability to report this information.)
What words do they use?
What is the tone of the interaction and the feeling conveyed?
Does the parent teach the child the name of a person or object during the visit?
How does the parent discipline or restrain the child? Does the parent seem positive
when speaking about the child?
4. PHYSICAL EXAMINATION
a. Measure the child’s length or height and weight, and calculate body mass index
(BMI).
Plot these on the growth charts (see BUKU KIA)
Share the information with the family.
b. As part of the complete physical examination, the following should be particularly
noted:
• Early childhood caries (baby bottle tooth decay), developmental dental
anomalies, malocclusion, pathologic conditions, or dental injuries
• Excessive injuries or bruising that may indicate inadequate supervision or
possible abuse
• Other evidence of possible neglect or abuse
c. Additional Screening Procedures
Vision: Examine eyes; assess for strabismus.
Hearing: Conduct initial hearing screening if not previously done; otherwise,
assess for possible hearing loss, with follow-up screening as needed
Lead exposure: Assess risk of lead exposure and screen as needed
Anemia: Assess risk of anemia and screen as needed
Hyperlipidemia: Assess risk of hyperlipidemia
Tuberculosis: Administer tuberculin test (PPD) if child meets any of the
following risk criteria: Exposure to tuberculosis, Radiographic or clinical

7/23/2019 Presentasi Kasus Bayi Sehat
http://slidepdf.com/reader/full/presentasi-kasus-bayi-sehat 7/7
CASE PRESENTATION & CLINICAL GUIDELINE
HEALTHY INFANT Page 7
APRIL 20
findings, Homelessness, HIV infection, or living with person who has HIV, Other
medical risk factors
5. IMMUNIZATIONS
For 2 years: MMR, Tiphoid, Hepatitis A
REFERENCES “
M. Joycelyn Elders, M.D. EARLY CHILDHOOD 1-4 YEARS. BRIGHT FUTURES GUIDELINES
FOR HEALTH SUPERVISION OF INFANTS, CHILDREN, AND ADOLESCENTS.
www.brightfuture.aap.org pada tanggal 17 April 2013











![Standart Materi Presentasi Opp Pt Melia Sehat Sejahtera Terbaru [Repaired] Fix](https://static.fdokumen.com/doc/165x107/5493dba9ac7959222e8b49d4/standart-materi-presentasi-opp-pt-melia-sehat-sejahtera-terbaru-repaired-fix.jpg)








