Pengantar Mata Kuliah: Kebijakan dan Manajemen Mutu...
55
Pengantar Pengantar Mata Mata Kuliah Kuliah: Kebijakan Kebijakan dan dan Manajemen Manajemen Mutu Mutu (Safety and Quality) (Safety and Quality) Peminatan Peminatan HPM HPM-2017 2017 Adi Utarini ([email protected] ) Sekretaris: [email protected] ; Asisten:
Transcript of Pengantar Mata Kuliah: Kebijakan dan Manajemen Mutu...

PengantarPengantar MataMata KuliahKuliah::KebijakanKebijakan dandan ManajemenManajemen MutuMutu (Safety and Quality)(Safety and Quality)
PeminatanPeminatan HPMHPM--20172017
Adi Utarini ([email protected])Sekretaris: [email protected]; Asisten:
Tujuan pembelajaran umum:Menggunakan kerangka berpikir untuk
menganalisis masalah keselamatanpasien, kebijakan dan mutu pelayanan kesehatanserta mengidentifikasi intervensi perbaikankeselamatan pasien dan mutu pelayananMemahami sistem manajemen mutu dan memilih
pendekatan-piranti peningkatan mutuMenyusun program kegiatan untuk melakukan
perbaikan mutu yang berkesinambungan
Menggunakan kerangka berpikir untukmenganalisis masalah keselamatanpasien, kebijakan dan mutu pelayanan kesehatanserta mengidentifikasi intervensi perbaikankeselamatan pasien dan mutu pelayananMemahami sistem manajemen mutu dan memilih
pendekatan-piranti peningkatan mutuMenyusun program kegiatan untuk melakukan
perbaikan mutu yang berkesinambungan
Tujuan pembelajaran khusus Menganalisis masalah keselamatan pasien dan mutu
pelayanan menggunakan kerangka Berwick Melakukan analisis risiko dalam pemberian pelayanan
kesehatan Menganalisis kerangka kerja mutu dan indikator mutu
pelayanan kesehatan Memahami sistem manajemen mutu dalam pelayanan
kesehatan Merencanakan peningkatan mutu yang berkesinambungan
dalam pelayanan kesehatan Melakukan analisis kebijakan mutu dan fraud dalam era
jaminan kesehatan nasional
Menganalisis masalah keselamatan pasien dan mutupelayanan menggunakan kerangka Berwick
Melakukan analisis risiko dalam pemberian pelayanankesehatan
Menganalisis kerangka kerja mutu dan indikator mutupelayanan kesehatan
Memahami sistem manajemen mutu dalam pelayanankesehatan
Merencanakan peningkatan mutu yang berkesinambungandalam pelayanan kesehatan
Melakukan analisis kebijakan mutu dan fraud dalam erajaminan kesehatan nasional

Struktur Sesi Perkuliahan
Pasien dan masyarakat• Pengantar: Safety and Quality serta
Model Berwick• Pemberdayaan pasien dan
masyarakat
Sistem mikro pelayanan• Manajemen risiko dan safety• FMEA, RCA• Standar dan indikator mutu
Sistem makro organisasi• Sistem manajemen mutu• Kepemimpinan mutu• Komitmen dan budaya mutu• CQI, UR• Model-piranti QI dan metode statistik• Program Safety and Quality
Lingkungan• Kebijakan Kemenkes• Mutu dan fraud di era JKN• Kerangka kerja mutu• Kebijakan -regulasi layanan primer
dan sekunder• Akreditasi fasyankes

Evaluasi Mata Kuliah Penugasan: @ 10%
1. Menemukan artikel yang terkait dengan masalah safety danmutu pelayanan kesehatan: lessons learnt dan analisis denganKerangka Berwick (Individu)
2. Berpartisipasi dalam pembelajaran mutu yang diselenggarakanoleh pihak internasional (kelompok)
3. Menyusun rangkuman bab dalam buku (kelompok)4. Berpartisipasi menulis di website mutupelayanankesehatan
(individu)
Ujian: 60% Tengah semester: 20% (bentuk tertulis) Akhir semester: 40% (penugasan utama)
Presensi: Memenuhi 75% sebagai syarat mata kuliah
Penugasan: @ 10%1. Menemukan artikel yang terkait dengan masalah safety dan
mutu pelayanan kesehatan: lessons learnt dan analisis denganKerangka Berwick (Individu)
2. Berpartisipasi dalam pembelajaran mutu yang diselenggarakanoleh pihak internasional (kelompok)
3. Menyusun rangkuman bab dalam buku (kelompok)4. Berpartisipasi menulis di website mutupelayanankesehatan
(individu)
Ujian: 60% Tengah semester: 20% (bentuk tertulis) Akhir semester: 40% (penugasan utama)
Presensi: Memenuhi 75% sebagai syarat mata kuliah

How do you choose a “warung” ?

Which one is safer?


It was later revealed that a chain of errors before the surgery culminated inthe wrong leg being prepped for the procedure. While the surgeon's teamrealized in the middle of the procedure that they were operating on thewrong leg, it was already too late, and the leg was removed. As a result ofthe error, the surgeon's medical license was suspended for six months andhe was fined $10,000. University Community Hospital in Tampa, paid$900,000 to King and the surgeon involved in the case paid an additional$250,000 to King.
John Hawley had surgery in late January of 1998
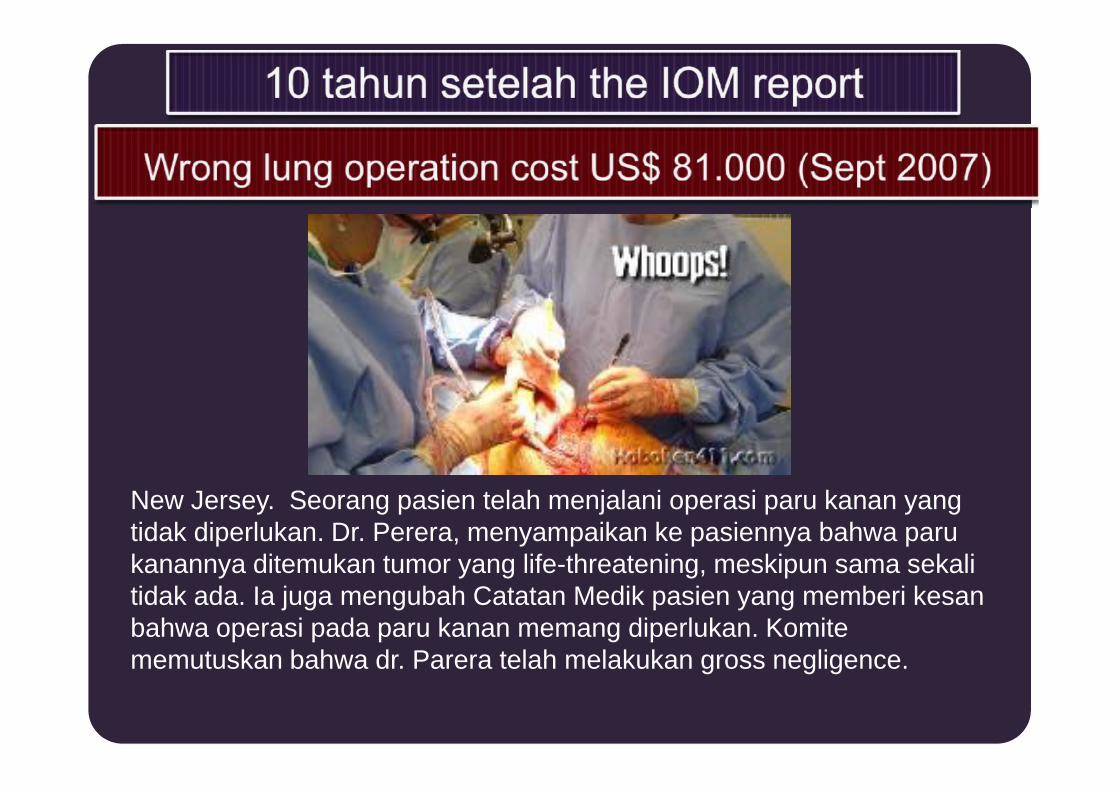
New Jersey. Seorang pasien telah menjalani operasi paru kanan yangtidak diperlukan. Dr. Perera, menyampaikan ke pasiennya bahwa parukanannya ditemukan tumor yang life-threatening, meskipun sama sekalitidak ada. Ia juga mengubah Catatan Medik pasien yang memberi kesanbahwa operasi pada paru kanan memang diperlukan. Komitememutuskan bahwa dr. Parera telah melakukan gross negligence.


Surgical site infections (SSI) di RS
Insidensi: 49,1%Insidensi: 49,1%
Widodo & Dwiprahasto, 2006
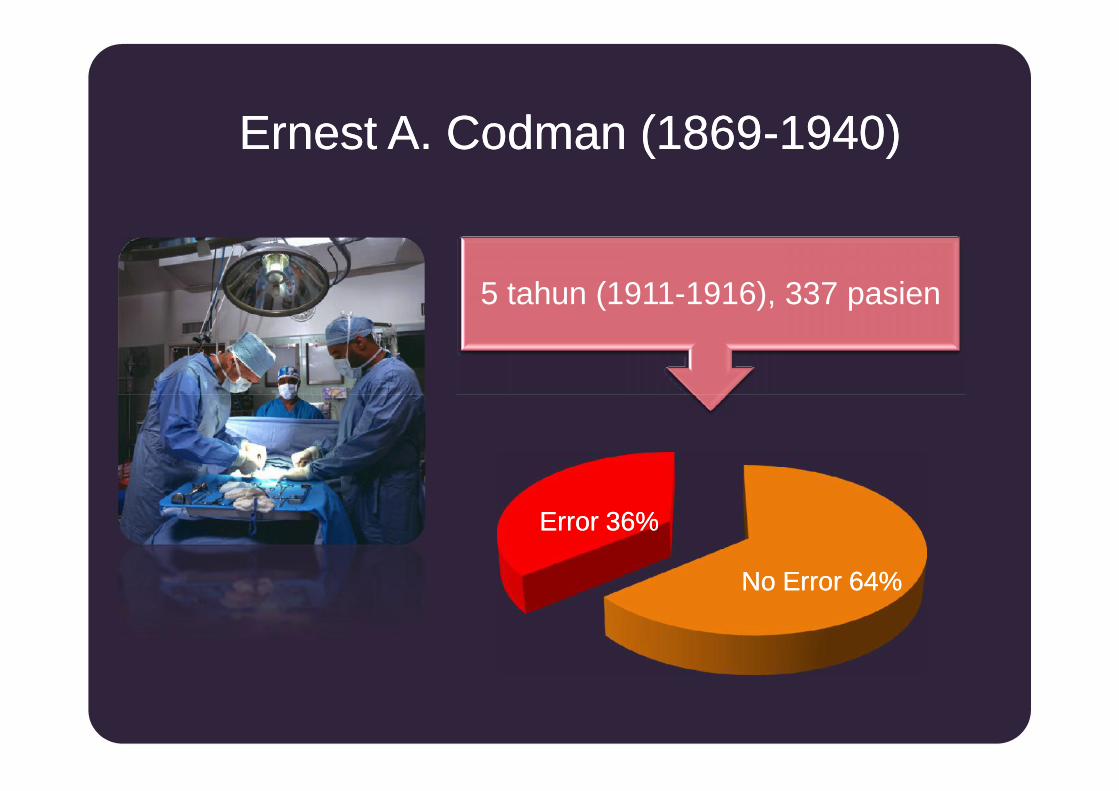
Ernest A. Codman (1869Ernest A. Codman (1869--1940)1940)
5 tahun (1911-1916), 337 pasien
Error 36%Error 36%
No Error 64%No Error 64%

Studi Prevalensi Kejadian yang Tidak Diharapkan
7,5
25
32
10,5
USA-2010
USA-2011
Amerika Latin
2010 – 2011
3,9
2,7
11,7
16,6
7,5
0 10 20 30 40
USA-1
USA-2
Inggris
Australia
Canada
%
1980 - 2005

Harvard School of Public HealthHarvard School of Public Health--SurveySurvey(2002)(2002)
1 dari 3 dokter mengaku1 dari 3 dokter mengaku
Pada keluarga atau pribadiPada keluarga atau pribadi
Pernah mengalami KTDPernah mengalami KTD

Patient safety, definition
• “the prevention of harm to patientsTheTheIOMIOM
• “freedom from accidental or preventableinjuries produced by medical care.
thetheAHRQAHRQ
• “freedom from accidental or preventableinjuries produced by medical care.
thetheAHRQAHRQEmphasis is placed on the system of care deliveryEmphasis is placed on the system of care delivery
thatthat
• (1) prevents errors;• (2) learns from the errors that do occur;• (3) is built on a culture of safety that involves health
care professionals, organizations, and patients.

The origins of the patient safety problem areclassified in terms of
typetype ofof errorerror
communicationcommunication patientpatientmanagementmanagement
clinicalclinicalperformanceperformancecommunicationcommunication
(failures between patient(failures between patientor patient proxyor patient proxy &&
practitioners, practitionerpractitioners, practitioner&& nonmedical staff, ornonmedical staff, oramong practitioners),among practitioners),
patientpatientmanagementmanagement
(improper(improperdelegation, failure indelegation, failure in
tracking, wrongtracking, wrongreferral, or wrongreferral, or wrong
use ofuse ofresources), andresources), and
clinicalclinicalperformanceperformance
(before, during,(before, during,and afterand after
intervention).intervention).

UUntowardntoward incidents, therapeutic misadventures, iatrogenicincidents, therapeutic misadventures, iatrogenicinjuries or other adverse occurrences directly associatedinjuries or other adverse occurrences directly associatedwith care or services provided within the jurisdiction of awith care or services provided within the jurisdiction of a
medical center, outpatient clinic or other facility.medical center, outpatient clinic or other facility.
May result from acts of commission or omissionMay result from acts of commission or omission(e.g., administration of the wrong medication, failure to(e.g., administration of the wrong medication, failure to
make a timely diagnosis or institute the appropriatemake a timely diagnosis or institute the appropriatetherapeutic intervention, adverse reactions or negativetherapeutic intervention, adverse reactions or negative
outcomes of treatment, etc.)outcomes of treatment, etc.)


Adverse drug eventsAdverse drug events in inin inppatientatient((ClassenClassen et al., 1997).et al., 1997).
Extra costExtra cost ProlongProlonghospitalizationhospitalization
IncreaseIncreasemortalitymortality
(Bates et al., 1997)
$8.4 million/year forteaching hospital
with 700-beds (Phillips, Christenfeld, andMcGlynn, 1998)
1983-1993: 2x fold(7.391 death 1993)

Failure of a plannedaction to be completed
as intended
ERROR, Definition (IOM, 1999)ERROR, Definition (IOM, 1999)
the use of a wrongplan to achieve an
aim
Errors include product, procedures, system
ERROR OF PLANNING ERROR OF EXECUTION
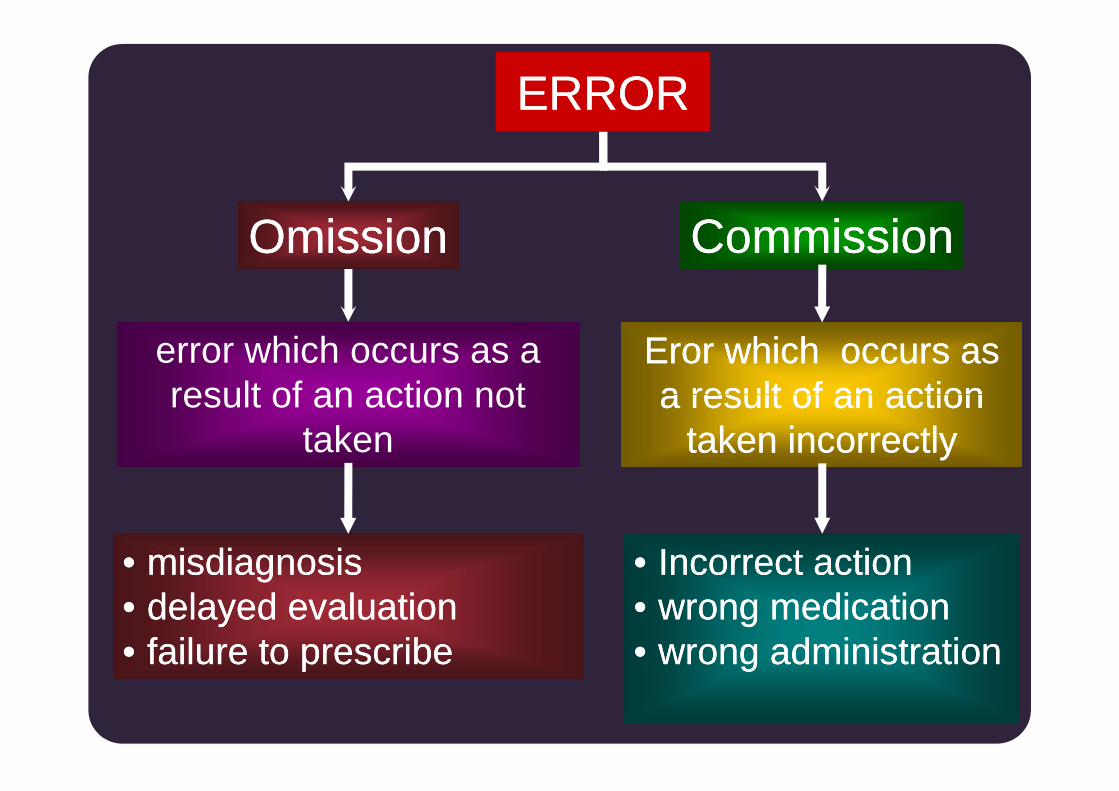
error which occurs as aresult of an action not
taken
OmissionOmission
Eror which occurs asEror which occurs asa result of an actiona result of an action
taken incorrectlytaken incorrectly
CommissionCommission
ERRORERROR
error which occurs as aresult of an action not
taken
Eror which occurs asEror which occurs asa result of an actiona result of an action
taken incorrectlytaken incorrectly
•• misdiagnosismisdiagnosis•• delayed evaluationdelayed evaluation•• failure to prescribefailure to prescribe
•• Incorrect actionIncorrect action•• wrong medicationwrong medication•• wrong administrationwrong administration


Severe
0s
Near Misses
Death1
Prevented/No harm incidents000s
Minor – Moderate00s

SLIPSLIP isis observeableobserveable,, LAPSE is notLAPSE is not
• turning the wrong knob on apiece of equipmentSlipSlip
• not being able to recallsomething from memoryLapseLapse
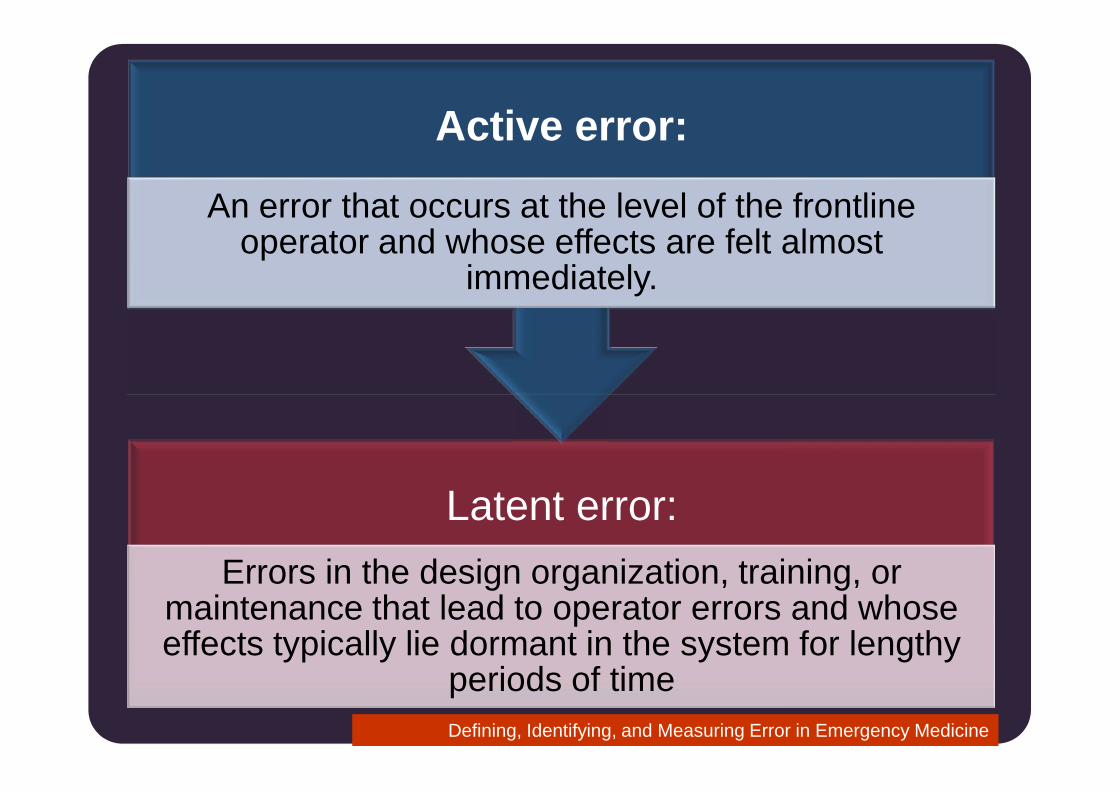
Active error:
An error that occurs at the level of the frontlineoperator and whose effects are felt almost
immediately.
Defining, Identifying, and Measuring Error in Emergency Medicine
Latent error:Errors in the design organization, training, or
maintenance that lead to operator errors and whoseeffects typically lie dormant in the system for lengthy
periods of time
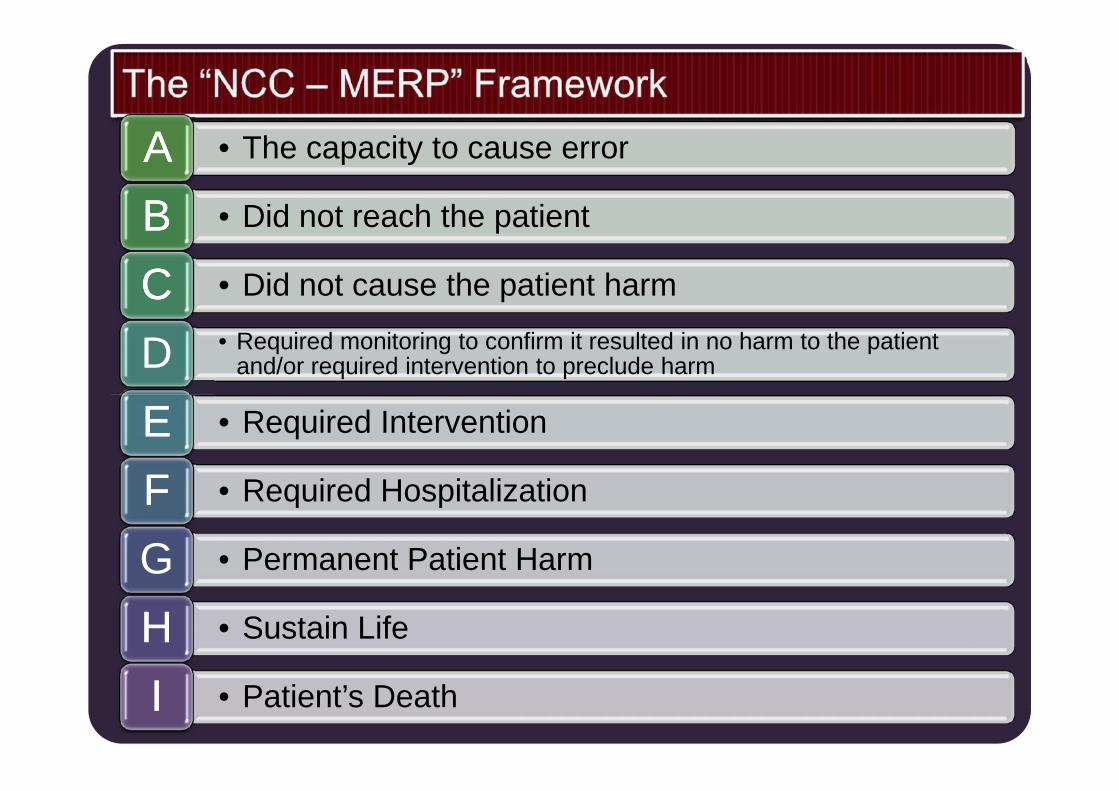
• The capacity to cause errorAA• Did not reach the patientBB• Did not cause the patient harmCC• Required monitoring to confirm it resulted in no harm to the patient
and/or required intervention to preclude harmD• Required InterventionEE • Required InterventionEE• Required HospitalizationFF• Permanent Patient HarmG• Sustain LifeHH• Patient’s DeathII



10
12
14
16
18 16,6
12,9
11 10,8
9
AustraliaAustralia New ZealandNew Zealand JapanJapan BritainBritain DenmarkDenmark CanadaCanada USAUSA
Adverse event in Health Care SystemAdverse event in Health Care System
%
0
2
4
6
8
10 97,5
3,7
The IOM, 1999

Multi-Causal Theory “Swiss Cheese” Diagram(Reason, 1991)
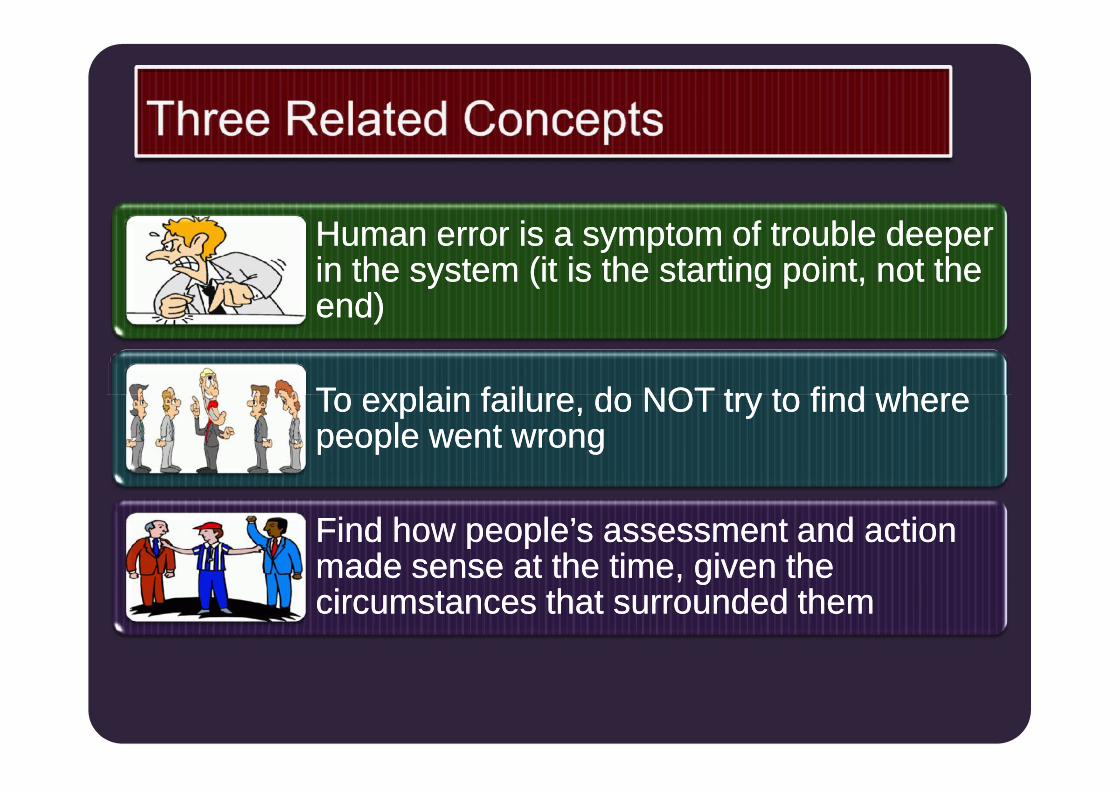
Human error is a symptom of trouble deeperHuman error is a symptom of trouble deeperin the system (it is the starting point, not thein the system (it is the starting point, not theend)end)
To explain failure, do NOT try to find whereTo explain failure, do NOT try to find wherepeople went wrongpeople went wrongTo explain failure, do NOT try to find whereTo explain failure, do NOT try to find wherepeople went wrongpeople went wrong
Find how people’s assessment and actionFind how people’s assessment and actionmade sense at the time, given themade sense at the time, given thecircumstances that surrounded themcircumstances that surrounded them

Freedom from accidental injuryFreedom from accidental injury
Patient safetyPatient safety
avoiding injuries or harm to patients from care that isavoiding injuries or harm to patients from care that isintended to help themintended to help them
Freedom from accidental injuryFreedom from accidental injury

1.1. Build aBuild a SAFETYSAFETY CULTURECULTURE
2.2. Build aBuild a ccomommmitmenitmentt && fofoccusus on patient safetyon patient safety
3.3. Develop integrated risk management programmeDevelop integrated risk management programme3.3. Develop integrated risk management programmeDevelop integrated risk management programme
4.4. DevelopDevelop record and report on patientrecord and report on patient safetysafety
5.5. Actively involve patients in communicatingActively involve patients in communicating safetysafety issuesissues
6.6. Learn from error and set up a more safety procedureLearn from error and set up a more safety procedure
7.7. Prevent injury or harm throughPrevent injury or harm through Patient SafetyPatient Safety programmeprogramme

oo Think SafetyThink Safety
oo Talk SafetyTalk Safety
oo Work SafetyWork Safety
oo BREATHE … SAFETYBREATHE … SAFETY
Jadi...............................
oo Think SafetyThink Safety
oo Talk SafetyTalk Safety
oo Work SafetyWork Safety
oo BREATHE … SAFETYBREATHE … SAFETY
… everyday… everyday
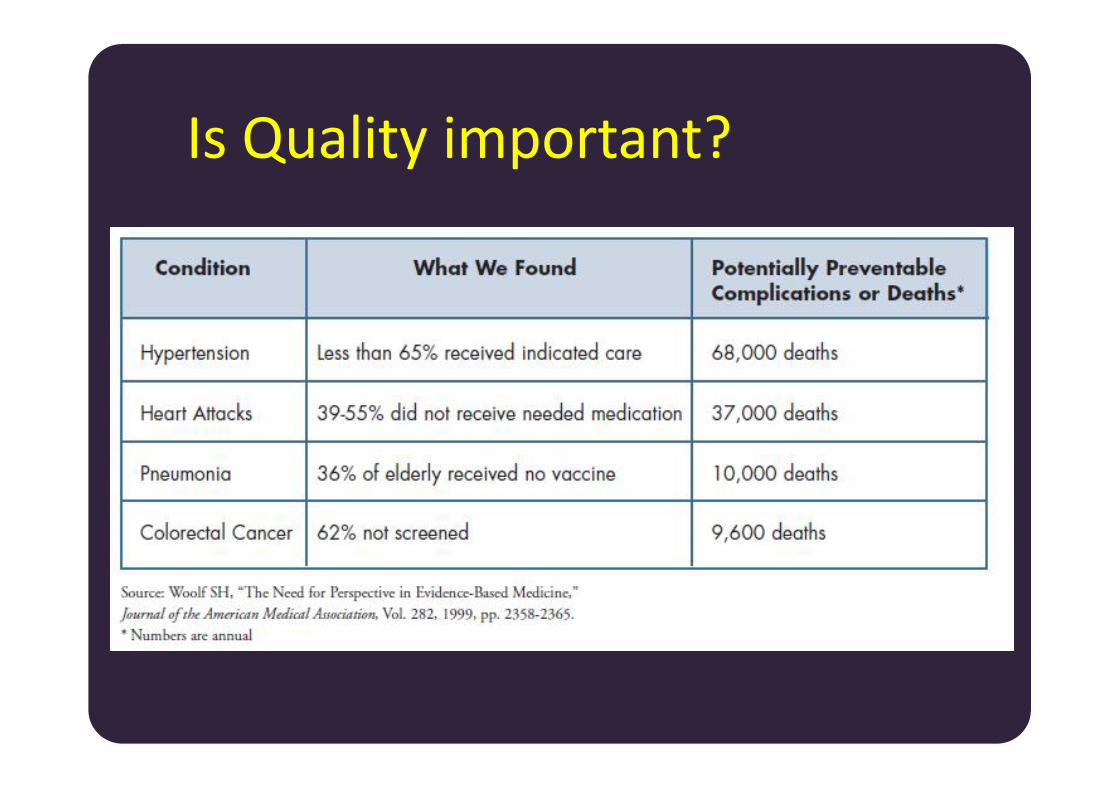
Is Quality important?
Is Quality important? In Hospital 6, less than 5% of TB suspects receive
sputum smear examination according to standards(Ref) In Medan, less than 20% of private practitioners
have heard of International Standards for TB Care(ISTC) (Ref) 1 dissatisfied patient will tell their experiences to
more than 3 persons “I have to sell the only piece of land I have for TB
treatment [which is free at the health centre]”
In Hospital 6, less than 5% of TB suspects receivesputum smear examination according to standards(Ref) In Medan, less than 20% of private practitioners
have heard of International Standards for TB Care(ISTC) (Ref) 1 dissatisfied patient will tell their experiences to
more than 3 persons “I have to sell the only piece of land I have for TB
treatment [which is free at the health centre]”

UU PraktekKedokteran
UUKesehatan
UUKonsumen
SJSN
Indikator SPMdll..
Perijinan
UU Rumah sakit
UUKesehatan
UUKonsumen
Permenkes
Akreditasi
The degree or grade of excellence
The Oxford English Dictionary (1988)
the degree to which health care services forindividuals and populations increase thelikelihood of desired health outcomes and areconsistent with current professionalknowledge.
Agency for health care research and quality
QUALITY: Definitions The degree or grade of excellence
The Oxford English Dictionary (1988)
the degree to which health care services forindividuals and populations increase thelikelihood of desired health outcomes and areconsistent with current professionalknowledge.
Agency for health care research and quality
QUALITY: DefinitionsCarrying out interventions correctlyaccording to pre-established standards andprocedures, with an aim of satisfying thecustomers of the health system andmaximizing results without generatinghealth risks or unnecessary costs.
Carrying out interventions correctlyaccording to pre-established standards andprocedures, with an aim of satisfying thecustomers of the health system andmaximizing results without generatinghealth risks or unnecessary costs.
Conformance to specification

QUALITY: Definitions
degree to which health services forindividuals and populations increase the
likelihood of desired health outcomes andare consistent with current
professional knowledge
IOM, 1990
degree to which health services forindividuals and populations increase the
likelihood of desired health outcomes andare consistent with current
professional knowledge
Definitions
National Association of Quality AssuranceProfessionals described quality as “the level ofexcellence produced and documented in theprocess of patient care, based on the bestknowledge available and achievable at a particularfacility.”
the Community Health Accreditation Programdefined quality as “the degree to which consumersprogress toward a desired outcome”
National Association of Quality AssuranceProfessionals described quality as “the level ofexcellence produced and documented in theprocess of patient care, based on the bestknowledge available and achievable at a particularfacility.”
the Community Health Accreditation Programdefined quality as “the degree to which consumersprogress toward a desired outcome”

QUALITY: Definitions
Conformance to standards …. Exceeding customer expectations ….Consists of
structure, process, outcomes
Conformance to standards …. Exceeding customer expectations ….Consists of
structure, process, outcomes

Defining Quality: Quality Dimensions:
Effectiveness Equity Efficiency Safety Access Patient
centeredness
Timeliness Consumer
engagement Community
engagement Technical
competence
Effectiveness Equity Efficiency Safety Access Patient
centeredness
Timeliness Consumer
engagement Community
engagement Technical
competence
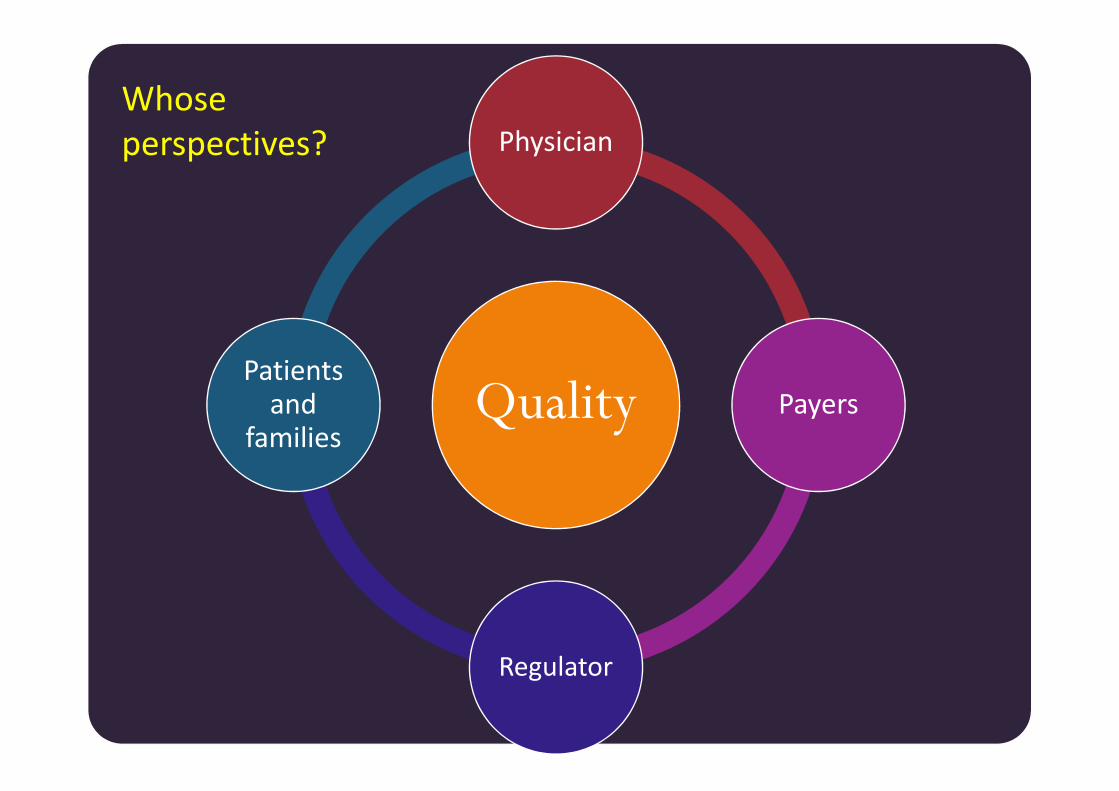
Quality
Physician
PayersPatients
andfamilies
Whoseperspectives?
Quality Payers
Regulator
Patientsand
families
1. Quality1. QualityAwarenessAwareness
2.2. QualityQualityMeasurementMeasurement
3. Quality3. QualityImprovementImprovement

Chain of effect in Improving HealthcareQuality (Berwick model, 2001)


Suara pasienSuara pasien
“Dua jam sebelum operasi sayatidak melihat adanya penandaoperasi pada ekstremitas yangakan dioperasi. Terdapatperbedaan informasi mengenaijenis tindakan anestesi antaradokter bedah dan dokteranestesi. Padahal pasien adalahdokter spesialis, dirawat di VVIP.Alhamdulillah operasi berhasilbaik dan pasien terhindari dariKTD”
“Dua jam sebelum operasi sayatidak melihat adanya penandaoperasi pada ekstremitas yangakan dioperasi. Terdapatperbedaan informasi mengenaijenis tindakan anestesi antaradokter bedah dan dokteranestesi. Padahal pasien adalahdokter spesialis, dirawat di VVIP.Alhamdulillah operasi berhasilbaik dan pasien terhindari dariKTD” Foto: Koleksi IHI

Penugasan 1: Individu (10%) Menemukan artikel (empirical research atau systematic
review) tentang safety dan quality di jurnal internasional Artikel harus berbeda antar mahasiswa Dari artikel tersebut ditulis: Artikel tersebut terkait dengan rantai peningkatan mutu
Berwick yang mana Apa pembelajaran penting atau hal menarik dari artikel tersebut
Deadline: Rabu, 1 Maret, dikumpulkan file menggunakanGamel (fasilitas Forum)
Menemukan artikel (empirical research atau systematicreview) tentang safety dan quality di jurnal internasional Artikel harus berbeda antar mahasiswa Dari artikel tersebut ditulis: Artikel tersebut terkait dengan rantai peningkatan mutu
Berwick yang mana Apa pembelajaran penting atau hal menarik dari artikel tersebut
Deadline: Rabu, 1 Maret, dikumpulkan file menggunakanGamel (fasilitas Forum)