13_Petunjuk Praktis Terapi Insulin Pada Pasien Diabetes Melitus
Upload
adi-aprihantaraCategory
view
91download
7Manajemen Diabetes Tipe 2 dengan Terapi Insulin
Manajemen Diabetes Tipe 2 dengan Terapi InsulinKeunggulan Lantus12Keuntungan Terapi InsulinPengobatan yang digunakan sejak lama, dengan pengalaman klinis yang lebih banyak Paling efektif menurunkan glukosa darah Dapat menurunkan kadar HbA1c pada keadaan apapunTidak ada dosis maksimum insulinEfek menguntungkan pada trigliserida dan HDLNathan DM, et al. Diabetes Care 2009;32 193-203.22Key PointsInsulin is the oldest of the currently available medications for the management of hyperglycemia in type 2 diabetes and has the most clinical experience. It is the most effective of diabetes medications in lowering glycemia: when used in adequate doses, it reliably decreases elevated HbA1c, and there appears to be no maximum dose beyond which a therapeutic effect will not occur.Insulin has also been shown to beneficially affect triglyceride and HDL cholesterol levels.
3Kekurangan terapi InsulinPeningkatan berat badan ~ 2-4 kg proportional to the correction of glycemia Predominantly the result of glycosuriaHypoglycemiaRates of severe hypoglycemia in patients with T2DM are low in treat-to-target clinical trials (compared to T1DM):Type 1 DM: 61 events per 100 patient-yearsType 2 DM: 1 to 3 events per 100 patient-yearsNathan DM, et al. Diabetes Care 2009;32 193-203.33Key PointsThe disadvantages of insulin therapy include weight gain of roughly 2 to 4 kilograms, which is probably proportional to the correction of glycemia and owing predominantly to the reduction of glycosuria. This weight gain could adversely affect cardiovascular health.Insulin therapy is also associated with hypoglycemia.Rates observed in clinical trails are much lower than in type 1 diabetes. In clinical trials aimed at normoglycemia and achieving a mean HbA1c of approximately 7%, severe hypoglycemic episodes (defined as requiring help from another person to treat) occurred at a rate of 61 per 100 patient-years in a type 1 diabetes trial (i.e. the DCCT intensive-therapy group), but occurred at a rate of just 1 to 3 per 100 patient-years in trials with type 2 diabetics.However, there is evidence that rates are much higher in the general population. Retrospective clinic-based surveys, and a prospective study of a population-based random sample of patients with type 2 diabetes revealed rates of hypoglycemia ranging from 28 to 73 per 100 patient-years.
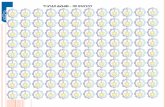
Gambaran skema kadar gula darah 24 jam dan profil insulin pada pasien tanpa diabetes
5
Indikasi Insulin DiniGula Darah Puasa (FPG) >250 mg/dL;Gula Darah Acak >300 mg/dL;HbA1C >10%;Ketonuria; atauGejala jelas diabetes polyuria, polydipsia, dan BB turun.[1,2]
1. Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care. 2006;29:1963-1972. Abstract 2. Hirsch IB, Bergenstal RM, Parkin CG, et al. A real-world approach to insulin therapy in primary care practice. Clin Diabetes. 2005;23:78-86.
Insulin mana yang digunakan?Memulai Terapi InsulinInsulin jangka panjang yang ideal?1 injeksi/hari mencakup 24 jamPeakless (tanpa puncak) Angka kejadian hipoglikemia rendah Kontrol gula darah yang baikKenaikan berat badan minimalDapat diprediksi Mudah digunakanDapat injeksi di berbagai tempatDapat diinjeksi pada waktu yang berbedaTidak perlu mencampur / cairan beningTingkat kepuasan dan penerimaan terapi yang baik8This slide lists the characteristics of the ideal long-acting insulinThe ideal long-acting insulin should safely provide a 24-hour peakless profile, thereby mimicking the normal physiological basal insulin profileThe ideal long-acting insulin should help patients achieve target A1C levels with:Low incidence of hypoglycaemiaPredictabilitySimple, once-daily injectionHigh treatment satisfaction and acceptance
Profil Farmakokinetik Insulin9
10
Memulai InsulinDosis inisiasi insulin berdasarkan berat badan 0.5 x berat badan (Kg)Dosis prandial = 20% dosis diberikan setiap kali makanDosis basal = 40% dosis diberikan saat malam / pagi hariPerkeni, 2011Contoh kasus:Pasien laki laki, berat badan 60 kgTotal dosis insulin = 0,5 x 60kg = 30 Unit / hariDosis prandial = 60% x 30 unit = 18 Unit / hari = 6 Unit / tiap kali makanDosis basal = 40% x 30 unit = 12 Unit / hariAplikasi pada pasienPasien laki laki, berat badan 60 kg.Hasil pemeriksaan dokterGDP 144 mg/dLHbA1c 9,2%Pasien mulai menggunakan insulin basal 12 Unit perhariDisuntikkan saat malam hari sebelum tidurPasien diberikan insulin glargine (Lantus)Target Gula darah puasa = 100mg/dL13Dosis Basal Insulin Multipel pada Detemir untuk mencapai efektivitas sama dengan Glargine sekali sehariLe Floch JP, et al. Diabetes Care. 2009;32:32-37Rosenstock J, et al. Diabetologia. 2008;51:408-416Robertson KJ, et al. Diabet Med. 2007;24:27-34Garg SK, et al. Diabetes Res Clin Pract. 2004;66:19-56
GLARGINEDETEMIR15
Perbandingan hargaTCBrandSediaanASKESHarga / IUHNA + VAT (Vial/Pen)NPHInsulatardVialRp.215,000Rp.215PenfillRp.85,000Rp.283HumulinVialRp.214,000Rp.214CartridgeRp.89,000Rp.297Long ActingLANTUSSoloSTARRp.110,000Rp.367LevemirFlexpenRp.112,000Rp.373Rp.85,000Rp.283PremixMixtardVialRp.215,000Rp.215PenfillRp.85,000Rp.283Humulin 30/70VialRp.214,000Rp.214CartridgeRp.89,000Rp.297Premix AnalogNovomixFlexpenRp.117,000Rp.390HumamixCartridgeRp.117,000Rp.390
17
18
TERIMA KASIH19
Copyright © 2022 FDOKUMEN