Managing Risk of Acs

of 44
-
Upload
vivin-yulvina -
Category
Documents
-
view
225 -
download
0
Transcript of Managing Risk of Acs
-
8/12/2019 Managing Risk of Acs
1/44
1
CURRICULUM VITAEDr. Muhammad Aminuddin SpJP K)-FIHA
Nama : Dr.Muhammad Aminuddin SpJP(K)-FIHAJabatan : Ka Dept/SMF Kardiologi dan kedokteran vaskuler
FK Unair / RSUD Dr Soetomo Surabaya
Alamat Kantor : Dept/SMF Kardiologi dan kedokteran
Vaskuler FK Unair-RSU Dr. Sutomo Surabaya
Jln. Mayjen Prof. Dr. Mustopo 6-8 SurabayaAlamat rumah : Jl. Manyar Kertoarjo I/7, Surabaya
Pendidikan :
- Dokter FK Universitas Airlangga : Th.1980
-Spesialis Ilmu Penyakit Jantung & Pembuluh Darah : Th. 1994
-Course in Cardiology : Osaka, Jepang th 2000Riwayat Jabatan :
- SPS Bag /SMF Kardiologi dan Kedokteran Vaskluler FK Unair
/RSUD Dr. Soetomo
Surabaya(2006 2011)
- Ka Dept/SMF Kardiolgi dan kedokteran vaskuler FK Unair /RSUDDr Soetomo Surabaya ( 20011 Sekarang)
-
8/12/2019 Managing Risk of Acs
2/44
Managing Risk of Patients withAcute Coronary Syndome:
What Should We Do?
Dr. M. Aminudin, SpJP (K) FIHADepartemen /Kardiologi dan Kedokteran
VaskulerRSU. Dr. Soetomo / FK-UNAIR
Surabaya
-
8/12/2019 Managing Risk of Acs
3/44
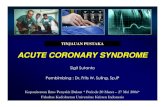
ACUTE CORONARY SYNDROME
No ST Elevation ST Elevation
Unstable Angina NQMI
NSTEMI
Classification of ACS
QMI
ECG
Manangement
HistoryPhysical Exam
-
8/12/2019 Managing Risk of Acs
4/44
Character of myocardial ischemia
-
8/12/2019 Managing Risk of Acs
5/44
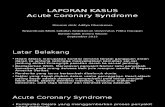
Vulnerable Plaque
Platelet cascadeThrombus formationVasospasm
Plaque rupture(55-80%)
ExertionBP, HR
Vasoconstriction
Pathophysiology
Acute MI
Complete occlusion
Unstable angina
Non-Q MI
Incomplete occlusionDistal embolization
Healingplaque
Spontaneous lysis
-
8/12/2019 Managing Risk of Acs
6/44
Platelet cascade
-
8/12/2019 Managing Risk of Acs
7/44
Thrombus formation
Factor
VII
Factor
XaProthrombin
Thrombin
(II)Fibrinogen
Fibrin
Promotes:
n Tissue factorsnAdhesive molecules
n Smooth muscle
n Leukocyte activation
n Platelet aggregation
n Release reaction
-
8/12/2019 Managing Risk of Acs
8/44
Vasospasm
Endothelium as an organ 1 to 6 x 1013cells monolayer
weighs 1 kg
covers 6 tennis courts
Modulator of vascular tone nitric oxide (NO)
prostaglandin I2 (PGI2,prostacycline)
Endothelin-1
TXA2
Regulator of hemostasis antithrombotic
prothrombotic
AnticoagulantGAGs/AT III
TFPI
Thrombomodulin
Profibrinolytict-PA
u-PA
Binding sites forplasminogenPA receptorsPlatelet inhibitoryPGI2(prostacycline)
Nitric oxideADPase
Carbon monoxide
ProcoagulantTissue factor
Binding sites forcoagulation factorsand fibrinAntifibrinolyticPAI
TAFIPlatelet activatingvWF
PAF
FibronectinEndothelin-1
TXA2
AntithromboticVasodilation ProthromboticVasoconstriction
-
8/12/2019 Managing Risk of Acs
9/44
Risk Factors for Cardiovascular
Disease Modifiable Smoking Dyslipidaemia
raised LDL cholesterol
low HDL cholesterol raised triglycerides
Raised blood pressure Diabetes mellitus Obesity Dietary factors Thrombogenic factors Lack of exercise Excess alcohol consumption
Non-modifiable Personal history
of CHD Family history
of CHD Age Gender
-
8/12/2019 Managing Risk of Acs
10/44
Major Risk Factors Additional Risk Factor
Cigarette smoking Small LDLparticle
Elevated blood pressure Ethnic characteristic
Elevated LDL & Total Cholesterol Psychososial factors
Low HDL Elevated TG
Diabetes mellitus Glucose intolerance
Obesity (abdominal obesity) Elevated homocysteine
Inactivity Elevated lipoprotein (a)
Family history of premature CAD Prothrombotic factor (fibrinogen)
Advancing age Inflamatory marker (CRP)
Grundy SM, et al. Assessment of cardiovascular risk by use of multiple-risk-factor assessment
equations. Circulation. 1999;100:148192.
Grundy SM, et al. Definition of metabolic syndrome. Circulation. 2004;109:433 8.
Risk Factor Assesment According to AHA
-
8/12/2019 Managing Risk of Acs
11/44
Principle ofACS management
Revascularization Medical
Balloon
CABG Medication for ischemia
Modified risk factors
Treatment of complicationFactor of revascularization
decrease area infarctionprevent LV dysfunctiondecrease mortality
TIME IS MUSCLE ANDMUSCLE IS TIME
Timing of symptoms Timing of treatments
Patient condition
Medical limitation Instrument limitation
Personal limitation
-
8/12/2019 Managing Risk of Acs
12/44
Principle of ACS management
ACS
AspirinNitrates
MoBeta blockersACEIAntithrombinClopidogrelGPII/IIIa
Early InvasivePrimary PCIFacilitate PCIRescue PCICABG
Early ConservativeFibrinolytic drugs
Risk stratification
HemodynamicstabilizationMedicalVentilatorIABPPace maker
Elective CAG+/- PCI or CABG
Adjuvant Rx
http://images.google.co.th/imgres?imgurl=http://www.heartcenteronline.com/myheartdr/images/article/Intra_Aortic.jpg&imgrefurl=http://www.heartcenteronline.com/myheartdr/common/articles.cfm?ARTID=431&h=310&w=302&sz=28&tbnid=op5-J7BhJRYJ:&tbnh=111&tbnw=109&shttp://images.google.co.th/imgres?imgurl=http://www.anesth.hama-med.ac.jp/Anedepartment/m-blease-respirator-da6.jpg&imgrefurl=http://www.anesth.hama-med.ac.jp/Anedepartment/museum.asp&h=574&w=370&sz=54&tbnid=zmVgbhEtYy8J:&tbnh=131&tbnw=85&start=36&prev=/images -
8/12/2019 Managing Risk of Acs
13/44
Medication of ACS
Fibrinolytic agents
Antinthrombotic agentsAnti-platelet therapy
aspirin, ticlopidine, clopidogrel, GP IIb/IIIainhibitors
Anti-coagulant therapy
heparin, low molecular weight heparin(LMWH)
Antiischemic agentsActivity, Oxygen
Morphine, Nitrates, Beta blockers
Others:ACEIs, ARBs, Statins, Fibrates
-
8/12/2019 Managing Risk of Acs
14/44
Indication of invasive management
Early and possible to invasive Rx.
Contraindication of fibrinolytic drugs
Consent from patient and relative
ComplicatedAMI
Cardiogenic shock
VSD, MR
Electrical instability
-
8/12/2019 Managing Risk of Acs
15/44
Percutaneous coronary angioplasty
-
8/12/2019 Managing Risk of Acs
16/44
Primary PCI and Lytic Therapy
Death Reinfarction Death Reinfarction30 days 6 months
** *
Grines CL. Circulation 1999
-
8/12/2019 Managing Risk of Acs
17/44
Risk & Benefit of PCI
Benefit Reduce
Mortality (Death, MI) Nonfatal MI
Reinfarction Rehospitalization
Effect in short and longterm outcome
Risk of PCI
Death 0-2% MI 3-5% Emergency CABG 3-7%
Stroke 0-1%
Limitation LM disease Diffuse disease 3 VV disease Personal resource
Interventionist Cath-lab nurse ED staff Team of primary
care Open24 hrs Policy
-
8/12/2019 Managing Risk of Acs
18/44
Indication ofPrimary PCI
Angina within 3 hrs and expectedDTBDTN less than 1 hr
Angina after 3 hrs
Severe CHF within 12 hrs of angina (I) or12-24 hrs of angina(IIa)
Shock within 36 hrs of angina (I) andrecommend PCI within 18 hrs ofshock
-
8/12/2019 Managing Risk of Acs
19/44
Non-Primary PCI
Rescue PCI Shock with in 36 hrs of
MI (PCI within 36 hrs ofshock)
Pt age < 75 yrs (I) Pt age 75 yrs (IIa)
Severe CHF and onset ofsymptoms within 12 hrs
Symptoms 12-24 hrs(IIa) with Hemodynamic or electrical
instability
Persistent ischemia
PCI after Fibrinolysis Recurrent of ischemia
(Fail fibrinolysis)
Cardiogenic shock or
hemodynamic instability Serious CHF (IIa)
Poor LVEF ( 40%) orserious ventricular
arrhythmia (IIa) Routine PCI after
fibrinolysis (IIb)
-
8/12/2019 Managing Risk of Acs
20/44
Coronary Arterial Bypass Graft
-
8/12/2019 Managing Risk of Acs
21/44
Indication for CABG
Fail or contraindication toPCI or Fibrinolytic drugs
Lesion is not suitable to PCI LM disease Triple disease
Complicated AMI acute severe MR
Rupture LV, VSD
-
8/12/2019 Managing Risk of Acs
22/44
Risk Factor Modification
Smoking Cessation 2.5 increased mortality riskreduced if quit
Diet modification
Low fat, low cholesterol
Hypertension Poorly controlled BP increases mortality risk
Diabetes Tight control, metformin if obese
Cardiac rehab (with exercise) Mortality benefits, Quality of Life
-
8/12/2019 Managing Risk of Acs
23/44
Secondary Prevention
Aspirin Continue indefinitely
Benefits established to 27 months (death,
non-fatal MI/stroke - ARR 4%)
Betablockers
Continue indefinitely
Long-term mortality benefits shown [BHAT, ISIS-1]
Titrate dose (according to BP) to HR of60bpm
-
8/12/2019 Managing Risk of Acs
24/44
Secondary Prevention (continued)
ACE Inhibitors LVF patientsmortality reduction at 1 to 5 yrs
Patients without LVF reduction in mortality,
MI, stroke (often initiated months after MI)[HOPE]
Lipid therapy Statins have shown long-term mortality
benefits Targets
LDL < 70 mg/dl
-
8/12/2019 Managing Risk of Acs
25/44
Medications Post-surgicalIntervention
CABG (Coronary Artery Bypass Graft)
anti-anginal medications usually ceased
continue secondary prevention medications
PTCA (Percutaneous Transluminal
Coronary Angioplasty) + Stent Insertion continue clopidogrel and higher dose
(300mg) aspirin daily for 9 month post-stentthen low dose aspirin indefinitely[CLASSICS]
-
8/12/2019 Managing Risk of Acs
26/44
Therapeutic Life Style Changes
Nutrient Recommended intakeTotal fat 25-35% of total calories
Saturated fate < 7% of total calories
Polyunsaturated fat Up to 10% of total calories
Monounsaturated fat Up to 20% of total calories
Carbohydrates 50-60% of total calories
Fiber 20-30 g/day
Cholesterol < 200 mg/day
Protein 15% of total calories
-
8/12/2019 Managing Risk of Acs
27/44
Therapy Dose (g/day) Effect
Dietary soluble fiber 2-8 LDL-C 5-10%
Soy protein 20-30 LDL-C 5-7%
Stanol esters 1.5-4 LDL-C 10-15%
DietaryAdjuncts: Efficacy at ReducingLDL-C
Jones PJ. Curr Atheroscler Rep1999;1:230-235
Lichtenstein AH. Curr Atheroscler Rep1999;1:210-214
Rambjor GS et al. Lipids1996;31:S45-S49
Ripsin CM et al. JAMA1992;267:3317-3325
-
8/12/2019 Managing Risk of Acs
28/44
Therapeutic Life Style Changes
Other l i fe sty le changes inc lude:
Weight reduction specially in overweight
patients (reduce 10% in the first 6 months)
Increase physical activity
Smoking cessation
-
8/12/2019 Managing Risk of Acs
29/44
Drug Therapy for Dyslipidemia
Bile acid resins
Ezetimibe
Niacin
Statins
Fibric acid derivatives
Fish oil
Postmenopausal drug therapy
-
8/12/2019 Managing Risk of Acs
30/44
Drugs of Choice for Dyslipidemia
Elevated LDL & TG values:
Drug of choice: Statin
Combination: statin + niacin; statin +ezetimibe; or statin + resin
It decreases LDL & TG but requirehigher doses for TG
For many patients with mixedhyperlipidemia can use a moderate doseof statin (to avoid side effects of higherdoses) with combination of either niacin,
resin, ezetimibe or fibrates
-
8/12/2019 Managing Risk of Acs
31/44
Drugs of Choice for Dyslipidemia
Normal LDL value but Low HDL:
Drug of choice: Niacin or fibratesIf patient have normal LDL OR
patient within LDL goal on statintherapy but still HDL high add niacin
or fibrates
-
8/12/2019 Managing Risk of Acs
32/44
Drugs of Choice for Dyslipidemia
Elevated TGs value:
Drug of choice: Fibrates & niacin
Can add fish oil If only TG level is high
-
8/12/2019 Managing Risk of Acs
33/44
4. Plaque rupture,cholesterol content,inflammation (hs-CRP)(statins)
3. Platelet adhesion/activation/aggregation(aspirin, clopidogrel,
GP IIb/IIIa inhibitors)
2. Activation of clotting
cascadethrombin(heparin/LMWH)
1. Downstream from thrombusmyocardial ischaemia/necrosis(-blockers, nitrates etc)
Platelet
GP IIb/IIIa
receptor
FibrinogenThrombin
Fibrin
clot
Pathophysiology of ACS and potentialpharmacological interventions
-
8/12/2019 Managing Risk of Acs
34/44
Statins*LDL-C reduction
Reduction in
chylomicron and
VLDL remnants,
IDL, LDL-C
Restore endothelialfunction
Maintain SMC function
Anti-inflammatory effects
Decreased thrombosis
Lumen
Lipid
core
Macrophages
Smooth
muscle
cells
Potential mechanisms of benefit ofstatins in ACS
*Statins differ
significantly
in terms of these
effects/mechanisms
-
8/12/2019 Managing Risk of Acs
35/44
LDL-Rmediated
hepatic uptake ofLDL and VLDL
remnants
Serum VLDL remnants
Serum LDL-C
Cholesterol
synthesis
LDL receptor
(BE receptor)
synthesis
Intracellular
Cholesterol
Apo B
Apo E
Apo B
Systemic CirculationHepatocyteThe reduction in hepatic cholesterol synthesis lowers intracellular
cholesterol, which stimulates upregulation of the LDL receptor and
increases uptake of non-HDL particles from the systemic circulation
LDL
Serum IDL
VLDLR
VLDL
ATORVASTATIN : HMG-CoA Reductase Inhibitor
Mechanism of Action
-
8/12/2019 Managing Risk of Acs
36/44
Main Effects of Statins
Effects on lipids: Reduce LDL-C, TC and TG
Increase HDL-C
Pleiotropic effects: Improve or restore endothelial function
Enhance the stability of atherosclerotic plaques
Decrease oxidative stress
Decrease vascular inflammation
Anti-thrombotic effects
Takemoto M, Liao JK.Arterioscler Thromb Vasc Biol2001;21:1712-1719.
-
8/12/2019 Managing Risk of Acs
37/44
Risk factor LDL-C
0 1 < 160 mg/dl2 < 130 mg/dl
CHD and CHD riskequivalent < 100 mg/dlVery high risk 70 mg/dl
NCEP-ATP III Report. JAMA 2001;285:2486-2497
Grundy SM, et al. NCEP Report. Circulation 2004;110:227-239
TARGET LIPID
LDL-C: Primary target of therapy
Total cholesterol < 200 mg/dlHDL-C > 40 mg/dlTriglyceride < 150mg/dl
-
8/12/2019 Managing Risk of Acs
38/44
The percentage reduction or elevation of
the various lipid fractions with the different drugs
Drug LDL HDL TG
Resins 15-35% -/4 % -/
HMG-CoA reductase 25-40% 5-10% 15-20%Inhibitors
Fibrates 10-25% 10-15% 50%
Nicotinic acid 15-35% 10-25% 50%
(from Chia reproduced with perm
-
8/12/2019 Managing Risk of Acs
39/44
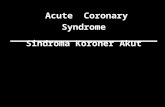
Statin Efficacy : LDL-C Reduction
*Simvastatin 80 mg not available at time of study.
**Significantly greater than mg-equivalent doses of
comparative agents (P .01).Significantly less than atorvastatin 10 mg (P .02).Significantly less than atorvastatin 20 mg (P .01).
Jones P, et al, for the CURVES Investigators.Am J Cardiol. 1998;81:582-587.
Atorvastatin
Simvastatin*
Pravastatin
Lovastatin
Fluvastatin
0 -60-50-40-30-20-10
10 mg (n = 73)
20 mg (n = 51)
40 mg (n = 61)
10 mg (n = 70)
20 mg (n = 49)
40 mg (n = 61)
10 mg (n = 14)
20 mg (n = 41)
40 mg (n = 25)
20 mg (n = 16)
40 mg (n = 16)
40 mg (n = 12)
20 mg (n = 12)
-38%**
-46%**
-51%**
-28%
-35%
-41%
-19%
-24%
-34%
-29%
-31%
-17%
-23%
80 mg (n = 10) -54%
80 mg (n = 11) -48%
% LDL-C reduction
-
8/12/2019 Managing Risk of Acs
40/44
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
Atorvastatin Experience : Clinical Safety Data
Digestive 4 8 9Body as a whole 5 5 6Musculoskeletal 1 3 4Nervous 2 3 3
Skin and appendages 1 2 2Metabolic/Nutritional 1 1 1Special senses < 1 1 < 1Urogenital 1 1 1Cardiovascular 2 1 1
Bodysystem
Placebon = 1789
Atorvastatin(all doses)n = 9416
All otherstatins combined
n = 5290
(%)
Treatment-Associated AEs 1% of Patients
(%) (%)
-
8/12/2019 Managing Risk of Acs
41/44
Atorvastatin Experience :
Clinical Safety Data
ALT/AST elevations > 3x ULN :
0.5% of patients treated with atorvastatin 10 to 80mg experienced ALT/AST elevations > 3x ULN.
Myalgia
Incidence of myalgia across all the atorvastatin
doses was low (1.9%) and directly comparable tothe incidence of myalgia observed in patients
receiving other statins combined.
Source: Pfizer Inc. Data on file. Review of 44 completed clinical trials.
-
8/12/2019 Managing Risk of Acs
42/44
Conclusions CHD is leading cause of mortality and was
responsible for approximately 30% of deaths
Principle management of ACS include
Revascularization Medical
Balloon
CABG
Medication for ischemia
Modified risk factors
Treatment of complication
-
8/12/2019 Managing Risk of Acs
43/44
Risk Factors for CVD include Dyslipidemia
LDL C is the mayor lipid risk factor fordevelopment and progression of CVD
LDL C reduction has been shown toimprove cardio vascular mortality andmorbidity
Statin are now clearly established as firstline drug for treatment patient withhypercholesterolaemia
Atorvastatin was proven to be effectiveand save
-
8/12/2019 Managing Risk of Acs
44/44