Kuliah Kanker Paru-2
39
-
Upload
mungunator -
Category
Documents
-
view
89 -
download
9
description
Kuliah Kanker Paru 2
Transcript of Kuliah Kanker Paru-2
-
KANKER PARU Adalah tumor ganas primer yang berasal dari saluran nafas (Bronkhus)
-
EPIDEMIOLOGI KANKERThousandsLungBreastColon/rectumStomachLiverProstateCervix uteriOesophagusBladderNon-Hodgkins lymphomaOral cavityLeukaemiaPancreasOvaryKidneyMaleFemale12001000800600400200Parkin et al 2001Worldwide in 2000IncidenceMortality020040060080010001200
-
KANKER PARUKanker paru merupakan penyebab utama kematian akibat keganasan, dengan sekitar 1.1 juta kematian per tahun di dunia.Sekitar 80% kanker paru merupakan jenis kanker paru bukan sel kecil/NSCLC (histologis)Kebanyakan pasien datang dalam keadaan stadium lanjutKemoterapi merupakan pengobatan utama.Gejala penyakit sering berat, dan sulit ditanganiFerlay et al 2000; Cersosimo 2002; Massarelli et al 2003
-
KANKER PARUPenyebab utama kematian akibat kanker85% - 95% berhubungan dg kebiasaan merokokPe konsumsi rokok Pe kematian akibat tumor paruBerasal dari umumnya sel saluran napasBiasanya datang ke dokter terlambatGol risiko tinggi :Usia > 40 thnPerokok beratBatuk
-
FAKTOR RESIKOFaktor resiko kanker paru meliputi: -perokok, baik aktif maupun pasif -lingkungan sekitar kita, baik lingkungan kerja maupun tempat tinggal (seperti gas radon, asbes, arsenik)-individual (seperti riwayat keluarga kanker paru)
-
Faktor penyebab terdiri dari :A .Faktor EnviromentRokok : Polynuclear aromatik hydrokarbon, Nitroamines, Aromatic amines, Zat organic dan non organic lainnya.Non Rokok : Polusi udara, Asbestos, Chromium, Arsenic, Bis (chloromethyl) ether (BMCE), Radon.B. Faktor Genetik.
-
TIPE KANKER PARUNSCLC (Non Small Cell Lung Cancer)Sekitar 80% dari semua kanker paruNon Small Cell Lung Cancer terdiri dari beberapa tipe, terutama : - Adenokarsinoma- Karsinoma sel skuamos- Karsinoma sel besarSCLC (Small Cell Lung Cancer)Sekitar 20% dari semua kanker paruKlasifikasi berdasarkan sel :- Karsinoma sel kecil- Karsinoma sel campur besar/kecil- Karsinoma kombinasi sel kecil
-
Non Small Cell Lung Carcinoma (Karsinoma Paru Bukan Sel Kecil) :1. Adenokarsinoma paru > insidens 40 % dari kasus NSCLC. > secara foto thoraks mirip dengan gambaran pneumonia atau pneumonialike appereance. > salah satu sub typenya : Bronkhoalveolar karsinoma (5% dari kasus adeno ca paru ) > berasal dari epithelium bronkhus atau kelenjar mukus dibawah sel epithelium.
-
> massa terletak lebih ke perifer atau dekat pleura. > dapat membuat scar atau disebut scarcar- cinoma, jarang membentuk cavity. > masa pertumbuhan/pembelahan 21 minggu > metastase ke pleura, adrenal glands , lymp node, tulang dan juga ke otak (jarang).
-
Bronkhoalveolar karsinoma (BAC) : > sering dihubungkan dengan Intertitial lung disease, parenchymal scaring dan exogenous lipoid carcinoma. > Ada 2 type : * Mucinous : 80% dari kasus BAC. ^ berasal dari columnar mucous containing cell ^ prognosa buruk .
-
* Nonmucinous : ^ berasal dari type II pneumocytes atau clara cell. ^ prognosa baik.
-
II. Squamous cell carcinoma / Epidermoid carcinoma paru : > insidens 20 30 % kasus NSCLC. > terletak lebih lebih ke sentral. > berasal dari sel squmous, sehingga terka- dang dapat didiagnosa dengan sitologi spu- tum. > metastase ke arah cabang bronkhus utama dan menyumbat lumen bronkhus---atelek- tase.
-
>sering membentuk kavitas. > masa pertumbuhan / pembelahan sel 12 minggu.
-
III. Large cell : > 5 % dari kasus NSCLC. > berasal dari epithel cell di daerah peripher bronkhus dan lebih dekat ke daerah sub- pleura. > bertumbuh sangat cepat. > prognosa kurang baik.
-
DIAGNOSIS KANKER PARUPhysical examinationDetect signsVisualise and sample mediastinal lymph nodesDetect position, size, number of tumoursDetect chest wall invasion, mediastinal lymphodenopathy, distant metastasesLymph node stagingDetect changes in hormone production, and haematological manifestations of lung cancerPrecise location of tumour, obtain biopsyChest X-rayCT scanPET scanLaboratory analysisBronchoscopyMediastinoscopyFNACytologyNCCN Guidelines 2000FNA, fine-needle aspirate; CT, computed tomography; PET, positron emission tomography
-
PROSEDUR DIAGNOSAKlinis : anamnese + PDIFoto Thoraks PA& lateral.ICT Scan thoraksITrans thorakal lung biopsiIBronkhoskopi (gold diagnostik).+ trans bronkhial lung biopsi
-
A. GEJALA KLINIS :l. Gejala Intrapulmonal:Batuk.Nyeri dada.Sesak nafas.
-
ll. Gejala Intratorakal Ekstrapulmo:Sindroma Horner : > Endopthalmus. > Miosis. > Ptosis.Sindrma Vena Cava Superior : > Pembengkakan pada lengan, wajah, leher. > Kolateral vena pada dinding.
-
Parese atau paralise diapragma-- n.frenikus.Parese atau paralise chorda vokalis -> n.recurrent.Disfagia-> oesophagusEfusi pleura penyebaran pada pembuluh getah bening regional intra torakal.
-
lll. Gejala Ekstratorakal non metastase:Manifestasi neuromuskular berupa neurophatia karsinomatosa : miopatia, neuropatia perifer, enchepalopatia.Manifestasi endokrine : > Sindroma Cushing. > Hiperparatiroid dengan hiperkalsemia. > Hiponatremia akibat sekresi ADH. > Hipoglikemia akibat sekresi insulin yang berlebih.
-
Manifestasi pada jaringan ikat dan tulang.Manifestasi vaskuler dan haematologi : anemia, purpura, migratori, trombopeblitis.
-
lV. Gejala Ekstratorakal Metastase : Gejala tergantung ke daerah metastase. Metastase ke : > Tulang. > Otak. > Pleura. > Paru kontralateral/ ipsolateral. > Hepar. > Kelenjar adrenal
-
GEJALA UTAMA KANKER PARUHollen et al 1999
-
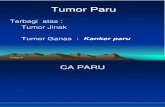
B. FOTO THORAKS :Foto Thoraks memberikan manifestasi antara lain :- Massa radiopaque di paru- Massa + obstruksi jalan nafas dengan gambaran atelektase - Massa + gambaran Pneumonia.- Pembesaran kelenjar para hilar : terutama pada oat sel - Kavitasi : terjadi 2 10 % kasus.- Tumor pancoast : terdapat gambaran massa didaerah superior atau apeks lobus superior - Efusi pleura Gambaran massa bisa terlihat bila besar tumor sudah diatas 2 cm.
-
Massa lobus inferior sinistra foto PA
-
C. CT SCAN THORAKS : Pada gambaran CT Scan Thoraks akan terlihat > letak massa tumor > ukuran massa tumor. > keterlibatan kelenjar. > metastase ke daerah paru lainnya atau ke rongga thoraks.
-
D. Bronkhoskopi : > melihat keterlibatan saluran nafas mulai laring----bronkhus. > melihat letak massa secara visual langsung. > mengambil sample jaringan dengan biopsi , atau sikatan bronchus melakukan BAL untuk pemeriksaan sitologi.
-
E. PEMERIKSAAN LAINNYA :TTLB : trans thoracal lung biopsy, bila letak tumor didaerah perifer dapat dilakukan pengambilan jaringan massa melalui dinding dada.Tumor marker : > CEA. > SCC. > Cypra 21-1.
-
STAGING/ STADIUM.Pendrajatan atau steging/stadium NSCLC ditentukan dengan International Staging System for Lung Cancer 1997 berdasarkan TMN T : adalah tumor N : adalah keterlibatan KGB M : adalah menunjukkan metastase.
-
STADIUM KANKER PARULymph nodesBrokus utamaContralateral lymph nodeMetastase ke organ jauh Invasif pada dinding dada
-
PRESENTASI STADIUMKANKER PARU NSCLC (80%)21%Stage III60%Stage IV10%Stage I9%Stage IIStadium lanjut (III & IV) : ~ 80%80% jenis NSCLC/Kanker paru bukan sel kecil
-
Sebelum dilakukan pengobatan Kanker paru biasanya ada 2 hal yang dipertimbangkan :Status performance : penilaian keadaan umum penderita , Karnofsky > 70.Laboratorium : > HB . 10 gr% > Leukosit < 9000. > ureum darah < 50, creatinine < 1,0 > creatinine clearence 24 jam > 70.
-
Bagaimana pengobatankanker paru .
-
PENGOBATAN KANKER PARUPengobatan kanker paru saat ini :- Bedah- Kemoterapi - Radioterapi- Target terapiPengobatan tergantung pada stadium penyakit.
-
PENGOBATAN STADIUM AWALKANKER PARUStadium I & IIHanya 20% dari jumlah kasus, kebanyakan sudah pada tahap lanjut atau stadium akhir.Terapi utama berupa operasi dengan atau tanpa radioterapi dan kemoterapi. Angka kekambuhan sekitar 50%
-
PENGOBATAN STADIUM LANJUT KANKER PARUStadium III & IVAngka harapan hidup 1 tahun : 15-20%Pengobatan pada stadium ini:- Bedah (IIIa)- Kemoterapi- Kemoterapi + radioterapi- Terapi biologi/target terapi- Penanganan paliatif
-
KEMOTERAPISebelum 1995 :- Etoposide/Teniposide- Vinblastine/Vindesine- Mitomycin-C- Ifosfamide- DoxorubicinEfek samping beratDiberikan secara kombinasi
Sesudah 1995 :- Vinorelbine- Paclitaxel/Docetaxel- GemcitabineEfek samping lebih sedikitRespon terapi lebih baik
-
PENGOBATAN KANKER PARUObat kanker paru sekarang lebih baik dibanding obat generasi sebelumnya.Selain efikasi yang baik, dokter akan memilihAPA YANG TERBAIK BAGI PASIEN dalam hal toksisitas / efek samping dan kualitas hidup pasien.
-
Kualitas hidup yang baik akan memberikan semangat baru untuk mereka dan keluarga
-
SMALL CELL LUNG CARCINOMA( KARSINOMA PARU SEL KECIL ) Kasus SCLC hanya 10- 20 % dari kasus Kanker paru. > 90% kasus pada perokok, pekerja tambang, industri asbes dan radon. > letak massa tumor di sentral. > penyebaran secara dini dan cepat ke daerah
-
bronkhial, hilus dan lympnode mediastinum dan otak. > prognosa kurang baik.
-
STAGING/ STADIUMBerbeda dengan NSCLC , stage SCLC :Limited stage : massa tumor terbatas pada paru serta kelenjar sekitar.(LS)Extensive stage : massa tumor sudah mulai keluar dari paru dan bermetastase ke organ lainnya.(ES)
-
PENGOBATAN
Biasanya SCLC terdiagnosa setelah stadium ES sehingga pengobatannya biasanya hanya palliative.
-
TARGET TERAPI
-
TARGET TERAPIDefinisi :Terapi yang menggunakan obat atau substansi lain untuk mengidentifikasikan dan menyerang sel kanker tertentu (target) tanpa mempengaruhi sel-sel normal. TARGET : Protein tertentu/khusus pada sel kanker.
-
Kenapa TARGET TERAPI ??
-
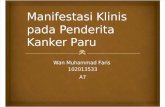
NSCLC response rates decrease with subsequent regimens of chemotherapyObjective response rate (%)Massarelli et al 2003Line of therapy20.916.32.30.02.3
-
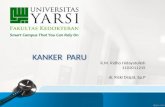
Months after start of 3rd- or 4th-line therapySurvival probability061218240.00.20.40.60.81.00.10.30.50.70.9Median survival4 months 1-year survival5.5%n=433rd- and 4th-line chemotherapy is of limited benefit in NSCLCMassarelli et al 2003
-
PENGOBATAN KANKER PARUKalangan medis membutuhkan pengobatan kanker paru yang efektif dan dapat ditoleransi dengan baik. Respon terhadap pengobatan makin berkurang dengan berlanjutnya lini pengobatan pada kemoterapi (lini 2, lini 3)Bila jenis kemoterapi ditambah maka efek samping/toksik >>>Sangat diperlukan terapi kanker paru yang efektif, aman dan efek samping minimal kualitas hidup >>
-
**Each year 1.2 million people worldwide are diagnosed with lung cancer and there are 1.1 million deaths as a result of this disease. The incidence of lung cancer is greater in men than in women, with men accounting for ~73% of new cases and deaths.1There are two major histopathological types of lung cancer: small-cell lung cancer and NSCLC; approximately 80% of lung cancer cases are accounted for by NSCLC. Disease-related symptoms are often severe, debilitating and difficult to manage,2 and include dyspnoea, cough, haemoptysis, pain, fatigue and weight loss.A retrospective analysis of the outcome of advanced NSCLC patients who had received at least two chemotherapy regimens found that the median survival time from the start of the last treatment (either 3rd or 4th line) was 4 months.3
ReferencesFerlay J et al. GLOBOCAN 2000: Cancer incidence, mortality and prevalence worldwide, version 1.0. IARC CancerBase No. 5 [online]. Available at: http://www-dep.iarc.fr/globocan/globocan.htmlCersosimo RJ. Am J Health Syst Pharm 2002; 59: 611-642.Massarelli E et al. Lung Cancer 2003; 39: 55-61.*Small-cell lung cancer (SCLC) accounts for ~20% of all lung cancer cases.1Cellular classificationsmall-cell carcinomamixed small-cell/large-cell carcinomacombined small-cell carcinoma (SCLC combined with neoplastic squamous and/or glandular components).Without treatment, SCLC has the most aggressive clinical course of any type of pulmonary tumour (median survival from diagnosis of 2-4 months) but is much more responsive to chemotherapy and radiotherapy than other tumour types.2Owing to the tendency to disseminate early, SCLC is treated as a systemic disease, with chemotherapy as the cornerstone of treatment. Despite being initially chemosensitive, these carcinomas acquire drug resistance during the course of the disease. ReferencesZchbauer-Mller S, et al. Ann Oncol 1999; 10 (Suppl 6): 83-91.PDQ Treatment Guidelines 2000.*Current standard guidelines indicate that diagnosis may be made by bronchoscopy or cytology via a fine-needle aspirate. During the initial evaluation, all patients should have their history taken and undergo physical examination, chest X-ray and chest computed tomography (CT) scans (including the adrenal glands), liver CT scan or abdominal ultrasound. Other evaluations include a complete blood count, liver function tests, measurements of electrolytes, calcium, blood urea nitrogen, and creatinine, as well as a baseline ECG. Bone scans and/or brain CT scans may be appropriate in some patients.1The extent of the tumour, the involvement of the lymph nodes, and chest wall or mediastinal invasion can be determined with similar efficacy using either CT or magnetic resonance imaging (MRI). CT is used more commonly, although MRI may be preferable in specific situations, for example in evaluating superior sulcus tumours.2Positron emission tomography with radiolabelled fluoro-2-deoxyglucose combined with CT was significantly more accurate than CT alone in identifying lymph node involvement in NSCLC.3
ReferencesNCCN Guidelines 2000.Webb WR, et al. Radiology 1991; 178: 705-713.Vansteenkiste JF, et al. J Clin Oncol 1998; 16: 2142-2149.
*1. Hollen PJ, et al. Support Care Cancer 1999; 7: 140-148.673878681754118131521*StageStage0StageIAT1 N0 M0 StageBT2 N1 M0/T3 N0 M0 StageBT4 N M0/T N3 M0 StageT N M1*Non-Small Cell Lung Cancer: Stages at PresentationNSCLC patients typically present with advanced disease. Approximately one third of NSCLC patients present with early localized disease amenable to surgical treatment. **In a retrospective meta-analysis, examination of over 700 patients records identified 43 patients with advanced NSCLC who had received 3rd- or 4th-line chemotherapy after two prior regimens that included platinum and docetaxel, given concurrently or sequentially.1Response rates to chemotherapy decreased with increasing numbers of chemotherapy regimens used.1Survival after 3rd- or 4th-line therapy is poor.1
ReferenceMassarelli E et al. Lung Cancer 2003; 39: 55-61.*Median progression-free and overall survival times were 2.2 and 4.0 months, respectively, following the start of the last treatment (either 3rd or 4th line); the 1-year survival rate was 5.5%.1
ReferenceMassarelli E et al. Lung Cancer 2003; 39: 55-61.*