KONSTIPASI-KULIAH-4

of 62
-
Upload
erika-kusumawati -
Category
Documents
-
view
7 -
download
0
Transcript of KONSTIPASI-KULIAH-4
-
KONSTIPASI PADA ANAKAgus FirmansyahDepartemen Ilmu KesehatanAnak FKUI-RSCM, Jakarta
This presentation will probably involve audience discussion, which will create action items. Use PowerPoint to keep track of these action items during your presentation
In Slide Show, click on the right mouse buttonSelect Meeting MinderSelect the Action Items tabType in action items as they come upClick OK to dismiss this box
This will automatically create an Action Item slide at the end of your presentation with your points entered.
-
EpidemiologiDefekasi normal, pertanda anak sehatTinja terlalu keras, besar, nyeri, jarang3% kunjungan dokter anak10-15% kunjungan ahli gastro anak95% konstipasi fungsionalSeringkali awal penyebabnya sederhana
-
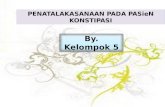
Pasien Konstipasi di PoliklinikGastroenterogi IKA-RSCM, Jakarta, 2003
-
Spesifikasi kasusKonstipasi akut ringan yang memerlu-kan penanganan yang memadaiKonstipasi yang memerlukan diagnosis etiologis dan tindakan segeraKonstipasi fungsional kronik yang memerlukan penanganan yang cermat dan memerlukan kesabaran
-
Batasan konstipasi (1)Kesulitan melakukan defekasi atau berkurangnya frekuensi defekasi tanpa melihat apakah tinjanya keras atau tidak (Rogers, 1997)Kesulitan defekasi yang terjadi tsb menimbulkan nyeri dan distres pada anak (Lewis & Muir, 1996)Frekuensi defekasi lebih jarang dan tinja lebih keras dari biasanya (Abel, 2001)
-
Batasan konstipasi (3)Ketidakmampuan mengevakuasi tinja secara sempurnaFrekuensi berhajat berkurang dari biasanyaTinja lebih keras dari biasanyaPalpasi abdomen teraba skibalaDengan atau tanpa enkopresis (Firmansyah, 1994)
-
Pola defekasi normalPada dewasa, 3 kali/hari sampai 3 kali/mingguBayi ASI > sering sp usia 4 bulan1-7 kali pada bayi (93%)Usia 4 tahun 1,2 kali dan 96% sudah sama dengan dewasaKonsistensi berbentuk (formed stool)
-
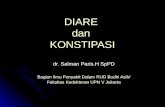
Frekuensi normal defekasi pada anak
-
Fisiologi defekasi (1)Regangan dinding rektumRefleks relaksasi SAIKontraksi SAE TOILETRelaksasi SAE dan m. PuborektalisKontraksi diafragma, dinding abdomen dan rektumSensor epitel: tinja cair, padat, gas
-
Fisiologi defekasi (2)Fungsi kolon: simpan dan keringkanMakan/minum sebagai stimulus defekasi (refleks gastrokolik)Asupan serat sebagai stool bulkingKurang minumMeningkatnya kehilangan cairanBerkurangnya aktivitas fisikStres dan perubahan aktivitas rutin
-
Tinja kerasFisura aniNyeri waktu defekasiWitholdingReabsorbsiTinja makin kerasMakin nyeriLingkaran setan: nyeri-witholding-skibala
-
Tinja keras & besarDistensi tinja kronikAmbang rangsangsensasi rektum Kemampuan sensor Panggilan defekasi (-)Lingkaran setan: distensi-sensasi
-
Etiologi konstipasi Neonatus dan bayiMeconium plugPenyakit HirscsprungFibrosis kistikMalformasi anorektal bawaanChronic idiopathic intestinal pseudo-obstruction syndromeEndokrin: hipotiroidAlergi susu sapiMetabolik: diabetes insipidus, RTARetensi tinjaPerubahan diet
-
Etiologi konstipasi Todler & umur 2-4 tahun
Fisura aniToilet refusalAlergi susu sapiPenyakit Hirschsprung segmen pendekPenyakit saraf: sentral atau muskular dengan hipotoniMedula spinalis: meningokel, tumor, tethered cord
-
Etiologi konstipasi Usia sekolah
Retensi tinjaKetersediaan toilet terbatasKeterbatasan kemampuan mengenali rangsang fisiologisPreokupasi dengan kegiatan lainTethered cord
-
Etiologi konstipasi Adolesen
Irritable bowel syndromeJejas medula spinalis (trauma, kecelakaan)DietAnoreksiaKehamilanLaxative abuse
-
Etiologi konstipasi Segala usia
Efek samping obat, perubahan diet, pascaoperasiRiwayat operasi anus-rektumRetensi tinja dan enkopresis akibat distensi tinja kronikPerubahan aktivitas fisik, dehidrasiHipotiroid
-
Etiologi konstipasi Alergi susu sapi
Konstipasi kronik yang sulit diatasi dengan diet tinggi serat dan laksatifAnak kurang dari 3 tahunEliminasi dan provokasi terbukti CMA (21 dari 27 kasus)Inflamasi (proktitis) menyebabkan nyeri pada defekasi Inflamasi menyebabkan gangguan motilitasIacono et al, 1995, Farias & Motta, 2003
-
Obat penyebab konstipasiAnestesi, analgesik narkotik, opiatAntikolinergik dan simpatomimetikAntikonvulsan dan diet ketogenikAntimotilitasAntipsikotik, antidepresanBarium pada pemeriksaan radiologisPenghambat kanal kalsium (misal verapamil) antidisritmiaMineral: Al, Ca, Pb. As, BiAntiinflamasi non-steroid
-
Gejala & tanda konstipasiFrekuensi defekasi berkurangNyeri dan distensi abdomenRiwayat tinja besar & kerasKecepiritPosisi tubuh, menyilangkan kedua kaki, berdansaTeraba skibala pada palpasi abdomenFisura ani, dilatasi ampula rekti
-
Pemeriksaan fisis pada konstipasi
AbdomenInspeksi anusColok duburPunggung dan spinaNeurologis
-
Red flags (1)Gagal tumbuhDistensi abdomenHilangnya lengkunglumbosakralPilonidal dimple covered by a tuft hairKelainan pigmentasi di garis tengah spina (lumbosakral)Agenesis sakrumBokong datar
-
Red flags (2)Letak anus di depanPatulous anusAmpula rekti kosong padahal teraba massa tinja pada palpasi abdomenTinja menyemprot bila telunjuk dicabut pada pemeriksaan colok dubur
-
Red flags (3)
Darah dalam tinjaKedutan anus hilangRefleks kremaster hilangTonus dan kekuatan otot ekstremitas bawah menurunFase relaksasi refleks tendon ekstre-mitas bawah hilang atau menurun
-
Komplikasi konstipasiNyeri: anus atau abdomenFisura aniEnkopresisEnuresisISK, obstruksi ureterProlapse rektumUlkus soliterSindrom stasis: bakteri tumbuhlampau, maldigesti, fermentasi, dekonyugasi asam empedu, steatore
-
Pemeriksaan penunjang
Foto polos abdomenPemeriksaan enema bariumBiopsi hisap rektumManometriPemeriksaan lain
-
Megakolon padaMorbus Hirschsprung
-
Daerah transisipada Morbus Hirschsprung
-
Tatalaksana konstipasi fungsionalEvakuasi tinja (Disimpaction)Terapi rumatan Intervensi diet Modifikasi prilaku Obat Pengamatan
-
Evakuasi tinja (disimpaction) (1)Harus dilakukan sebelum terapi rumatan per oral atau per rektal2-5 hari untuk evakuasi tinja yang lengkap/sempurnaFecal impactionMassa tinja (skibala) pada palpasi abdomenRektum yang dilatasi dan penuh tinja pada colok duburTinja yang berlebihan dalam kolon pada foto polos abdomen
-
Evakuasi tinja (disimpaction) (2)Per oralMineral oil 15-30 ml/tahun umur, maksimum 240 ml/hari, tidak pada bayiLarutan PEG 20 ml/kg/jam (maks 1000 ml/jam) via pipa nasogastrik 4 jam/hariPer rektumEnema fosfat hipertonik 3 ml/kg, 2 kali sehari, maksimum 6 enemaEnema garam fisiologis (600-1000 ml)Mineral oil 120 mlPada bayi: enema gliserin 2-5 ml
-
Terapi rumatanTujuan: mencegah kekambuhanBeberapa bulan, beberapa kasus sampai adolesenCatatan harianTerapi rumatan Intervensi diet Modifikasi prilaku Obat Pengamatan
-
Banyak minum
-
Kurangi asupan susu
-
Banyak makan buah & sayuran
-
Dietary fiberKebutuhan anak: 5 + (umur th) gramKonstipasi: 10 + (umur th) gram
At least two servings of fruit each dayAt least three servings of vegetables each dayWhole-wheat bread instead of white breadHigh-fiber cereals like bran cereal, shreded wheat, whole-grain cereal, and oatmealAmerican Family Physician Association
-
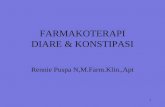
Kandungan serat
-
Synthetic bulking forming productPowderCitrucelEffer-sylliumFiberallMetamucil
GranulesPerdiem FiberSerutan ToastedWaferFiberallMetamucil
TabletFiberallFiber con
-
Pispot yang menarik
-
Buku cerita anak
-
Return to Web version
Toilet Training Your ChildWhen should I start toilet training my child?Do not start toilet training until both you and your child are ready. You are ready when you are able to devote the time and energy necessary to encourage your child on a daily basis for at least 3 months.Your child is ready when he or she can signal that the diaper is wet or soiled, or when your child is able to say that he or she would like to go to the potty. This usually occurs when a child is 18 to 24 months of age. However, it is not uncommon for a child to still be in diapers at 2 and a half to 3 years of age.How should I prepare my child for toilet training? Allow your child to be present when you go to the bathroom and make your child feel comfortable in the bathroom. Allow your child to see urine and bowel movements in the toilet. Let your child play with flushing the toilet.Before toilet training your child, place a potty chair in your child's normal living and play area so that your child will become familiar with the potty. Consider placing a potty chair on each floor of the house if you live in a multilevel home. Allow your child to observe, touch and become familiar with the potty chair.Tell your child that the potty chair is his or her own chair. Allow your child to sit fully clothed on the potty chair, as if it were a regular chair. Allow your child to leave the potty chair at any time. Do not force your child to spend time sitting on the chair.After your child has become used to the potty chair and sits on it regularly with his or her clothes on, try having your child sit on the potty without wearing pants and a diaper. Let your child become comfortable with sitting on the potty without wearing pants and a diaper.The next step is to show your child how the potty chair is used. Place stool from a dirty diaper into the potty chair. Allow your child to observe the transfer of the bowel movement from the potty chair into the toilet. Let your child flush the toilet and watch the bowel movement disappear down the toilet.How do I teach my child to use the toilet?After your child has become comfortable with flushing the toilet and sitting on the potty chair, you may begin teaching your child to go to the bathroom. Keep your child in loose, easily removable pants.Place your child on the potty chair whenever he or she signals the need to go to the bathroom. Your child's facial expression may change when he or she feels the need to urinate or to have a bowel movement. Your child may stop any activity he or she is engaged in when he or she feels the need to go to the bathroom.Most children have a bowel movement once a day, usually within an hour after eating. Most children urinate within an hour after having a large drink.In addition to watching for signals that your child needs to urinate or have a bowel movement, place your child on the potty at regular intervals. This may be as often as every 1-1/2 to 2 hours.Stay with your child when he or she is on the potty chair. Reading or talking to your child when he or she is sitting on the potty may help your child relax. Praise your child when he or she goes to the bathroom in the potty chair, but do not express disappointment if your child does not urinate or have a bowel movement in the potty. Be patient with your child.Once your child has learned to use the potty chair, your child can begin using an over-the-toilet seat and a step-up stool.How long will it take to toilet train my child? It may take up to 3 months. It is important for you to be patient and supportive. Do not punish your child when he or she has an accident.If your child is not toilet trained within 3 months, consult your family doctor. The most likely reason your child has not learned to use the potty is that your child is not yet ready for toilet training.Reviewed/Updated: 9/00 Created: 1996This handout provides a general overview on this topic and may not apply to everyone. To find out if this handout applies to you and to get more information on this subject, talk to your family doctor. Copyright 1996-2000American Academy of Family Physicians Permission is granted to print and photocopy this material for nonprofit educational uses. Written permission is required for all other uses, including electronic uses. Home | Privacy Policy | Contact Us | About This Site | What's New
-
Obat untuk terapi rumatanLaktulosa (larutan 70%): 1-3 ml/kg/hariSorbitol (larutan 70%): 1-3 ml/kg/hariMineral oil : 1-3 ml/kg/hariMagnesium hidroksida (400mg/ml): 1-3 ml/kg/hariCisapride: 0,2 mg/kg/kali 3-4 kali/hariKombinasi
-
Obat pencaharPer oral atau per rektal
Laksatif osmotikLubrikanLaksatif stimulanPelunak tinja
-
Laksatif osmotik (1)Menimbulkan efek osmotik pada kolon dan kemudian merangsang peristaltikLaktulosa (1-3 ml/kg/hari PO 2 dosis)Sorbitol (1-3 ml/kg/hari PO 2 dosis)Magnesium hidroksida (1-3 ml/kg/hari PO 2 dosis)
-
Laksatif osmotik (2)
Magnesium sitrat (1-3 ml/kg/hari PO 4 dosis)Sodium fosfat (6 ml/kg/hari PR 2 dosis)Polietilen glikol =PEG (5-10 ml/kg/hari PO 2 dosis)
-
Lubrikan (pelicin)Melunakkan tinja dan mengurangi absorpsi air dalam saluran cernaMineral oil (1-3 ml/kg/hari PO 2 dosis; tidak dianjurkan pada bayi)Lebih palatabel bila dingin atau dicampur dengan jus buah
-
Laksatif stimulanMeningkatkan aktivitas peristaltik saluran cernaSenna (2,5-5 ml/kali 2 kali sehari; tidak dianjurkan pada anak < 2 tahun)Bisakodil (0,5-1 supositori/kali PR; 1/3 tablet (5 mg)/kali PO)
-
Pelunak tinjaKorporasi air dan lemak dalam tinja sehingga tinja menjadi lunakNa dokusat (20-60 mg/hari PO 2 dosis)
-
Terapi bedahHanya bila terapi medis yang optimal tidak berhasilAppendicostomyCecostomySigmoidostomyAntegrade colonic enemasCreates a conduit to the cecum that can be used to administer daily colonic irrigations
-
Catatan harianTidak ada buangair besar
-
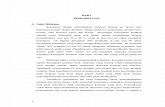
KonstipasiAnamnesis & pemeriksaan fisisPsedokonstipasiTidakYaLama konstipasiAkutKronikInfeksiObatKarenaobatYaTidakInfeksivirusTidakYaDiet?FaktordietNyeridefekasiFisura aniBenda asingBotulismeObstruksiYaOnset sebelum toilet trainingYaTidakTerdapat tinja di ampula rektiSarafEndokrinFungsionalMHMekoniumMassa pelvisAtresiaPsikiatrikFungsionalMHTidakYaTidakYaYaTidakTidakAlgoritme pendekatandiagnosis konstipasi
-
EBM dan konstipasi (1)Melakukan anamnesis dan pemeriksaan fisis yang lengkap dan cermat ternyata cukup untuk mendiagnosis konstipasi fungsional pada banyak kasusPada bayi, evakuasi feses dapat dilakukan dengan supositoria gliserin. Enema harus dihindariMineral oil dan laksatif stimulan tidak dianjurkan pada bayi
-
EBM dan konstipasi (2)Pada anak, mineral oil dan MgOH, laktulosa dan sorbitol (laksatif osmotik) merupakan obat yang aman dan efektifCisapride telah terbukti bermanfaat sebagai laksatif pada beberapa penelitian dan dapat digunakan pada kasus tertentuLarutan elektrolit polietilen glikol (PEG), diberikan dalam dosis rendah dalam waktu lama, mungkin merupakan alternatif pengobatan efektif pada konstipasi yang sulit diatasi
-
Kesimpulan (1)
Konstipasi sering ditemuan pada anak, baik yang akut maupun kronikSebagian besar (95 %) konstipasi pada anak merupakan konstipasi fungsionalPada sebagian besar kasus, anamnesis dan pemeriksaan fisis saja sudah cukup memadai untuk menatalaksana anak dengan konstipasi
-
Kesimpulan (2)
Hanya pada sebagian kecil kasus, yang diduga penyebabnya organik, pemeriksaan penunjang diperlukan untuk memastikan penyebabnyaTatalaksana konstipasi tdd evakuasi tinja dan terapi rumatan, yang tdd obat, modifikasi prilaku, edukasi dan konsultasiTerapi memerlukan waktu lama (berbulan-bulan) dan memerlukan kerjasama yang baik dengan orangtua
-
Buang air besar lancarpertanda anak sehat
-
TERIMA KASIH