Kasus Ujian Tahap i (Endang Sw)
15
Nama: Endang Sri Wahyuni, Tahap I, Mei 2013 KASUS UJIAN TAHAP I Seorang laki-laki 30 thaun di bawa ke RSDK, dimana anda jaga tahap I, keluarga menjelaskan selesai berkelahi tertusuk di perut 4 jam yang lalu. Muntah dan berak darah disangkal. Tensi 110/85, nadi 104 x/mnt, RR 30 x/mnt, tidak Nampak anemis, terdapat luka robek di bibir atas 1 cm, sudah tidak berdarah, thoraks pernafasan dan auskultasi simetri kanan dan kiri. Abdomen datar, luka di region epigastrium 3 cm sisi kiri linea mediana, 4 cm di atas umbulikus, panjang luka 1 cm, lebar 3 mm, tidak keluar darah maupun organ intra abdominal, palpasi nyeri tekan ringan sekitar luka yang lain supel, defence muskuler (-), pekak hepar (+), peristaltic (+), RT: tidak k olaps, tinja (+) warna kuning. 1. Kesimpulan tentang tensi dan nadi pada pasien ini pasca trauma adalah Tensi 110/85mmHg Nadi 104 x/mnt Rr 30 x/mnt Pada pasien ini hemodinamik stabil MAP = [(2 x diastolic) + systolic] / 3 (2X85)+110/3= 93,33 HEMODINAMIK STABIL MAP > 80 Nadi < 120 Urine > 50cc/jam Tidak ada tanda-tanda klinis syok
-
Upload
amsir-limbong -
Category
Documents
-
view
219 -
download
0
Transcript of Kasus Ujian Tahap i (Endang Sw)

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 1/15
Nama: Endang Sri Wahyuni, Tahap I, Mei 2013
KASUS UJIAN TAHAP I
Seorang laki-laki 30 thaun di bawa ke RSDK, dimana anda jaga tahap I, keluarga
menjelaskan selesai berkelahi tertusuk di perut 4 jam yang lalu. Muntah dan berak
darah disangkal. Tensi 110/85, nadi 104 x/mnt, RR 30 x/mnt, tidak Nampak
anemis, terdapat luka robek di bibir atas 1 cm, sudah tidak berdarah, thoraks
pernafasan dan auskultasi simetri kanan dan kiri. Abdomen datar, luka di region
epigastrium 3 cm sisi kiri linea mediana, 4 cm di atas umbulikus, panjang luka 1
cm, lebar 3 mm, tidak keluar darah maupun organ intra abdominal, palpasi nyeri
tekan ringan sekitar luka yang lain supel, defence muskuler (-), pekak hepar (+),
peristaltic (+), RT: tidak kolaps, tinja (+) warna kuning.
1. Kesimpulan tentang tensi dan nadi pada pasien ini pasca trauma adalah
Tensi 110/85mmHg
Nadi 104 x/mnt
Rr 30 x/mnt
Pada pasien ini hemodinamik stabil
MAP = [(2 x diastolic) + systolic] / 3 (2X85)+110/3= 93,33
HEMODINAMIK STABIL
MAP > 80
Nadi < 120
Urine > 50cc/jam
Tidak ada tanda-tanda klinis syok

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 2/15
2.Diagnosis banding pada kasus ini
Trauma tusuk abdomen hemodinamik stabil dd/ gasterDuodenum
Ileum
Colon transversum
Usulan : cek darah lengkap, O2 masker 10 lt, pasang DC
USG abdomen / MSCT Scan abdomen
Sumber:
NORTON
Modalitas penunjang pada trauma abdomen
1. DPL
1000 cc Nacl dimasukkan lewat kateter lavase
Di indikasikan pd pasien dengan syok, cedera organ serius, tidak sadar Positif 100.000 sel/mm3 (T. Tumpul)
1000 – 50.000 sel /mm2 (T. Tembus)
2. CT Scan
Sensitifitas dan spesifisitas tinggi pada T. Tumpul staging solid
organ
Memungkinkan untuk manajemen non-operative pada kasus2 tertentu
(CT Scan serial)
Kerugian kemungkinan miss dalam deteksi cairan intraperitoneal
yang minimal pada T. Tumpul

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 3/15
3. USG
FAST 4 lokasi hepatic dan spleenic gutter, perivesika/pelvis dan
perikardium4. Laparoskopi Diagnostik
Indikasi evaluasi pada tangensial gun shot wound dan assessment
pada kemungkinan cedera diafragma
Major diagnostic modalitas dalam Trauma Abdomen
1. DPL
2. CT Scan Abdomen (Kontras IV dan kontras per rektum/colon – Double
contrast)
3. USG
4. Diagnostic laparoscopy (DL)
(Feliciano, David V.; Mattox, Kenneth L.; Moore, Ernest E. Trauma, 6th Editio
Copyright ©2008 McGraw-Hill)
2. Melihat lokasi luka tusuk dan cara memegang pisau, jelaskan lapisan
dinding perut yang bias robek dan organ apa saja yang bias mengalami
kerusakan luka di region epigastrium 3 cm sisi kiri linea mediana, 4 cm di
atas umbulikuS
Organ yg bias terkena adalah gaster, duodenum
Lapisan-lapisan dinding perut1.Stratum superficialis:
Cutis
Subcutis(fascia abdominalis superficialis)

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 4/15
-lamina superficialis
-lamina profunda
2.stratum intermediusFascia abdominalis
Otot-otot dinding perut
Aponerosis otot dinding perut
3.stratum profunda/lapisan dalam
Fascia transversalis
Panniculus adiposus preperitonealis/ preperitoneal fat
Peritoneum parietale
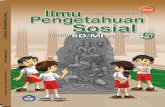
FAST menunjukkan black strip line tipis antara ginjal kiri dan lien serta
hypoechoic disertai enhancement di belakangnya di luar vesica urinaria yang terisi
penuh.
4.Kesimpulan tentang hasil FAST: Ada cairan bebas dalam rongga intraperitonium
5.apa kasus ini memerlukan foto thorax
Perlu, karena Pada pasien luka tusuk di atas umbilicus, patut dicurigai cedera
thoracoabdominal dengan rontgen foto thorax tegak bermanfaat
untuk menyingkirkan hemo atau pneumothorax, ataupun untuk mengetahui adanya
udara bebas intraperitoneal
6.apakah sdh ada indikasi laparotomi?
Sudah, karena adanya cairan bebas dalam intraperitonium yang berarti adanya
darah, artinya luka tusuk sudah melewati peritoneum

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 5/15

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 6/15

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 7/15
Nilailah respon penderita terhadap pemberian cairan awal
Nilai perfusi organ ( nadi, warna kulit, kesadaran dan produksi urin ) serta awasi
tanda-tanda syokPemberian cairan selanjutnya berdasarkan respon terhadap pemberian cairan awal.
Respon cepat
Pemberian cairan diperlambat sampai kecepatan maintenance
Tidak ada indikasi bolus cairan tambahan yang lain atau pemberian darah
Pemeriksaan darah dan cross-match tetap dikerjakan
Konsultasikan pada ahli bedah karena intervensi operatif mungkin masih
diperlukan
Respon Sementara
Pemberian cairan tetap dilanjutkan, ditambah dengan pemberian darah
Respon terhadap pemberian darah menentukan tindakan operatif
Tanpa respon Perlu tindakan operatif sangat segera( operasi laparotomi)
( Advanced Trauma Life support for doctor, student course manual eighth
edition 2008)
Resusitasi dan vital organ support
- Menilai keadaan umum dan tanda vital pasien
-
Pasang CVC untuk menilai CVP- Pasang oksimetri untuk menilai saturasi O2 dan HR
- Pasang DC untuk memantau fungsi ginjal dan melihat produksi
urine

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 8/15
- Cek lab elektrolit
- Kemudian prinsip penanganan pertama sesuai ABCDAir way diharapkan diperoleh air way yang paten sebelum beralih ke
terapi selanjutnya
Breathing dinilai frekuensi nafasnya, irama nafasnya
Circulation penerapan EGDT ( Early Goal Direct Treatment ) dengan
menerapkan EGDT.
Fluid chalange dengan menggunakan cairan kristaloid 1000cc
atau 300-500 cc koloid pada 30 menit pertama.
Target dalam 6 jam adalah:
- Central Venous Pressure 8-12 mm Hg (12-15 in ventilator pts)
- Mean arterial pressure > 65 mm Hg
- Urine output > 0.5 mL/kg/jam
- ScvO 2 or SvO 2 ≥ 70% atau mixed venous ≥ 65%

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 9/15
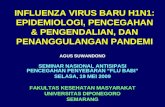
Kursus Perioperatif, Acute Care Surgery,Kolegium Bedah Indonesia, 2010Protocol for Early Goal-Directed Therapy
Supplement O2Endotracheal intubations
Mechanical ventilation
Central venous andarterial catheterization
Sedation, Paralysis(if intubated), or both
CVP
MAP
ScvO2
Crystalloid
Colloid
< 8 mmHg
Vasoactive agents< 65 mmHg
> 90 mmHg
8 – 12 mmHg
65 – 90 mmHg
≥ 70%
Goalachieved
Transfusion of RCuntil Ht ≥ 30%
≥ 70%
< 70%
Inotropic agents
Hospital admission YesNo
< 70%
Ket:Target pertama adalah CVP mencapai 8-12 mmhg. Jika dari 8 mmHg maka dapat
dilakukan terapi dengan kristaloid ataupun dengan koloid.
Jika target pertama sudah tercapai maka lanjut ke target ke dua yaitu MAP 65-
90mmHg. Jika belum tercapai dapat diberikan vasoactive agent.
Kemudian jika sudah tercapai target yang kedua maka masuk ke target yang ke 3, yaitu ScvO2
≥70. Jika belum sesuai maka dapat diberika transfusi atau pemberian inotropik

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 10/15
The choice of resuscitation fluid depends on the condition of the patient. The use
of a warmed balanced salt solution such as Ringer's lactate is considered safe andeffective. A bolus of 2 L is given to the adult patient with hypotension,
and 20 mL/kg to the child. If a hemodynamically normal state is restored, the
Ringer's lactate solution can be continued.
If the patient remains unstable a second bolus is utilized while blood is being
obtained. If the patient's vital signs have not returned to normal after 1 to 2 boluses,
blood should be administered. If the need is urgent, type-specific blood may be
used. When this is not available, low-titer type O-positive blood for men or O-
negative blood for women is acceptable.
The patient who needs uncross-matched blood usually needs to be in the operating
room (Feliciano, David V.; Mattox, Kenneth L.; Moore, Ernest E. Trauma, 6th
Editio Copyright ©2008 McGraw-Hill)
9. Bilamana pasien ini supel, tetapi muntah darah apa yg anda duga?Tindakandiagnostic yang dilakukan dan tindakan pengobatan yang dilakukan?
Jawab: ada perdarahan gaster, dilakukan endoscopy.
10. Metode Saftan dalam pengelolaan luka tusuk abdomen adakah pengelolaan
untuk itu?
Jawab: In 1960, Shaftan developed an approach of selective conservatism for
penetrating abdominal injury and revolutionized abdominal stab wound
management .[3]

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 11/15
Investigators in this field continue to study various protocols and investigative
tools. Despite impressive advances in investigative techniques, the optimal method
to determine the need for laparotomy has yet to be definitively established.
The objective is to reduce the number of patients with trivial or no intraperitoneal
injury who are subjected to laparotomy. However, a high degree of diagnostic
accuracy must be maintained to limit the frequency of missed injury. A reduction
in unnecessary hospitalization is also targeted.
In asymptomatic patients with stab wounds to the anterior abdomen, the following
2 methods are widely used to help determine the need for laparotomy:
Abdominal stab wound exploration (subsequent diagnostic peritoneal lavage
[DPL], serial clinical evaluation, or both are used to further assess patients in
whom an exploration cannot definitively exclude peritoneal penetration.)
Serial clinical evaluation
Other modalities that have been studied include DPL alone, CT, laparoscopy, and
ultrasonography .[4, 5] These strategies of selection for laparotomy are explored in
greater detail below.
Abdominal stab wound exploration forms part of a strategy developed by surgeons
to allow a more selective approach. It is a safe, rapid, and cost-effective tool in the
management of asymptomatic patients who present with an anterior abdominal
stab wound .[6, 7]
This approach has no place in the treatment of patients who areunstable, who have peritonitis, or who have evisceration.
Patients with peritonitis and those who are hemodynamically unstable should
undergo mandatory laparotomy. The authors advocate abdominal stab wound

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 12/15
exploration in asymptomatic patients who present with an anterior abdominal stab
wound. An exploration with negative findings is reliable and highly sensitive . [8, 9]
More than 25% of anterior abdominal stab wounds do not penetrate the peritoneal
cavity .[7, 10, 11]
A wound exploration that demonstrates an intact posterior rectusfascia (superior to the arcuate line) or transversalis fascia (inferior to the arcuate
line) allows the safe discharge of these patients from the emergency department .[12]
(abdominal stab wound exploration,jurnal)
11. Kalau pasien ini perdarahan, pada Hb berapa mutlak diperlukan transfuse
darah?jelaskan,jenis darah apa yang diberikan? Mengapa demikian?
Bila Hb <7, diberikan PRC sesuai dengan hasil kebutuhan koreksinya, karena
yang kurang adalah sel darah merah maka diberikan PRC
Volume resuscitation of the trauma patient requires repletion of oxygen-carrying
capacity with red blood cell transfusion
and restoration of intravascular volume to replace extracellular losses. However,
blood transfusion carries inherent risksincluding transfusion reaction, infection, and systemic immunosuppression.
Several reports have attempted to clarify
what levels of hemoglobin (Hgb) and hematocrit are appropriate in critically ill
patients. A prospective, randomized trial
demonstrated that Hgb levels as low as 7.0 to 9.0 g/dL did not increase mortality in
critically ill patients compared to a
group transfused to Hgb levels of 10.0 to 12.0 g/Dl
In summary, the decision to transfuse erythrocytes must be individualized to the
patient. The healthy 30-year-old patient

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 13/15
with euvolemia without ongoing blood loss and a hemoglobin of 7 g/dL is less
likely to benefit from transfusion than the
70-year-old patient with hypovolemia with ongoing hemorrhage and a hemoglobin
of 9 g/dL.It is the clinician's responsibility to combine the available clinical, laboratory, and
physiologic data as previously described to make rational
transfusion decisions.
In general, the adage "the sicker the patient, the higher the hemoglobin" provides
the surgeon and
intensivist the rationale to consider transfusion.
(Feliciano, David V.; Mattox, Kenneth L.; Moore, Ernest E. Trauma, 6th Editio
Copyright ©2008 McGraw-Hill)
12. Kalau setelah 2 minggu setelah dipulangkan pasien sesak nafas mendadak dan
paru-paru kiri bawah timpani pada perkusinya apa kecurigaan anda.
Bagaimana memastikan diagnosis dan apa tindakan lanjutnya?
Jawab:
Kecurigaan trauma pada diafragma.
Memastikan diagnosis dengan foto rontgen thorax AP/Lat atau CT scan
Tindak lanjutnya cito laparotomi.
Diaphragmatic rupture can result from blunt or penetrating trauma and occurs in
about 5% of cases of severe blunt trauma to the trunk.Diagnostic techniques
include X-ray, computed tomography , and surgical techniques such as
laparotomy . Diagnosis is often difficult because signs may not show up on X-ray,
or signs that do show up appear similar to other conditions. Signs and symptoms
included chest and abdominal pain, difficulty breathing, and decreased lung
sounds. When a tear is discovered, surgery is needed to repair it.

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 14/15
(Feliciano, David V.; Mattox, Kenneth L.; Moore, Ernest E. Trauma, 6th Editio
Copyright ©2008 McGraw-Hill)

8/13/2019 Kasus Ujian Tahap i (Endang Sw)
http://slidepdf.com/reader/full/kasus-ujian-tahap-i-endang-sw 15/15





![Embriotomi [Dr. Endang]](https://static.fdokumen.com/doc/165x107/55cf989b550346d03398a034/embriotomi-dr-endang.jpg)