Hirschsprung’s Disease
22
Hirschsprung’s Disease Refleksi Kasus
-
Upload
jejepurple -
Category
Documents
-
view
43 -
download
1
description
HD
Transcript of Hirschsprung’s Disease
Hirschsprung’s DiseaseRefleksi Kasus
Laporan Kasus Identitas Pasien
Nama : By. Ny. C Umur : 12 hari (lahir tanggal 19/1/2013) Jenis Kelamin : Laki-laki
Identitas Ibu: Nama : Ny. C Umur : 33 tahun Pekerjaan : IRT Pendidikan : SMA Agama : Islam Alamat : Jl. Bung Tomo Rt. 9 no. 97
Identitas Ayah Nama : Tn. A Umur : 43 tahun Pekerjaan : Swasta Pendidikan : SMA Agama : Islam Alamat : Jl. Bung Tomo Rt. 9 no. 97
Keluhan Utama : Muntah-muntah berwarna hijau kehitaman
TelaahPasien mengalami muntah-muntah sejak umur
2 hari, muntah sedikit-sedikit berwarna hijau kehitaman. Pasien juga tidak mau menyusu dan mengalami perut kembung sejak usia 6 hari. Pasien sejak lahir tidak pernah BAB. Saat lahir pasien langsung menangis.
Riwayat PersalinanPasien lahir spontan dengan Apgar Score 8/9
ditolong oleh bidan. Berat badan lahir 2200 gram. Usia kehamilan 39-40 minggu.
Riwayat Antenatal CareDi Bidan sebanyak 3 kali.
Pemeriksaan FisikKeadaan umum : Sakit beratTanda vital : Nadi : 155 x/i RR : 54 x/i T : 36,7 K/L : Anemis (-) Ikterik (-) Drooling (-) Sianosis (-)
Mongoloid face (+)Thorax
Cor : Murmur sistolik (+) gallop (-)Pulmo : Suara nafas vesikuler, rhonki (-) wheezing (-)
AbdomenInspeksi : Cembung, venektasi (+), penonjolan massa (-),
dam contour (-), dam steifung (-)Palpasi : Soefl, devans muskuler (-)Perkusi : TimpaniAuskultasi : BU (+) kesan meningkat, metalic sound (-)
GenitaliaPenis skrotum dalam batas normal, testis (+/+)
EkstremitasAkral hangat, edema (-)
Rectal ToucheSfingter ani menjepit kuat, mukosa licin,
massa (-),



LaboratoriumHb : 19 Leukosit : 11.290Trombosit : 154.000Hct : 50.3%
Na: 132K: 4,2Cl : 109
DiagnosisSuspect Hirschsprung Disease
PenatalaksanaanPuasaOGT dialirkanInfus Aminofusin paed dan lipofundinRencana pemeriksaan colon in loop dengan
water soluble kontrasKlisma NaCl 0,9% 20-40 ccBebas klisma 1x24 jam sebelum colon in loopCek T3 T4 TSH
Tinjauan PustakaDefinition
Hirschsprung disease is a developmental disorder of the enteric nervous system that is characterized by the absence of ganglion cells in the myenteric and submucosal plexuses of the distal intestine.
EpidemiologyThe incidence of Hirschsprung disease is
approximately one in 5,000 live born infants. 4:1 favoring males over females. Asian children seem to have the highest incidence at almost 3 per 5000 live births.
EtiologyCellular and molecular abnormalities in the
development of the enteric nervous system, along with incomplete migration of the neural crest cells, are a major part of the cause of HD.
Neural crest-derived neuroblasts appear in the developing esophagus at about 5 weeks’ gestation in the human fetus. These cells then migrate in both a cranial and caudal direction into the rest of the developing gut between 5 and 12 weeks’ gestation.
Pathophysiologylack of propagation is associated with the
absence of ganglion cells in the myenteric and submucosal plexus. The cause of the spasm in the aganglionic bowel is unclear. Cholinergic hyperenervation, inadequate distribution of nitric oxide synthetase, and abnormalities of the interstitial cells of Cajal have all been reported to be associated with HD
The majority (75%) of patients with HD have ganglion cells down to the level of the rectosigmoid colon
Long-segment HD, which describes aganglionosis of the descending colon, splenic flexure, or transverse colon, occurs in approximately 15% of patients.
total colon aganglionosis, which occurs in 5% to 7% of patients.
DiagnosisFor the neonate with a clinical picture and
plain radiographs suggesting distal neonatal bowel obstruction, the first step in the diagnostic pathway should be a water-soluble contrast enema.
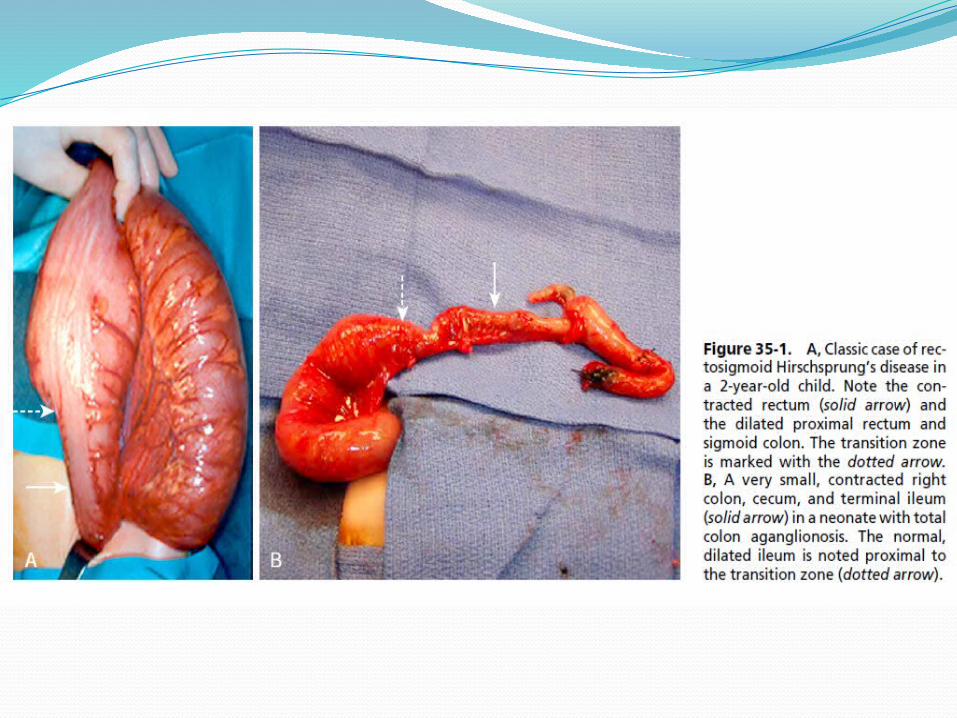
The pathognomonic finding of Hirschsprung disease on contrast enema is a transition zone between normal and aganglionic bowel

TherapyThe first priority is resuscitation, particularly
in neonates with intestinal obstruction or enterocolitis
Children with enterocolitis should undergo active colonic decompression using digital rectal stimulation and saline rectal irrigations (10–20 mL/kg every 6–8 h)
The goals of surgical management for Hirschsprung disease are to remove the aganglionic bowel and reconstruct the intestinal tract by bringing the normally innervated bowel down to the anus while preserving normal sphincter function.
Most children can be treated with a one-stage pull-through procedure, although a stoma may still be appropriate for those with severe enterocolitis, malnutrition, massive colonic distention, inadequate pathology support, or long-segment disease.