hamil, depresi
8
Association of glucocorticoid and type 1 corticotropin-releasing hormone receptors gene variants and risk for depression during pregnancy and post-partum Neelam Engineer a , Lucy Darwin b , Deole Nishigandh a , Kandala Ngianga-Bakwin c , Steve C. Smith b , Dimitris K. Grammatopoulos b, c, * a Dept of Obstetrics and Gynaecology, UHCW NHS Trust, Coventry, UK b Dept of Clinical Biochemistry, UHCW NHS Trust, Coventry, UK c Division of Metabolic and Vascular Heallth, Warwick Medical School, University of Warwick, Coventry, UK article info Article history: Received 29 December 2012 Received in revised form 27 March 2013 Accepted 6 May 2013 Keywords: HPA axis Postnatal depression CRH receptor GR Variant abstract Women with postnatal depression (PND) appear to have abnormal hypothalamic pituitary adrenal (HPA) axis responses to stress, which might involve a genetic variability component. We investigated associ- ation of genetic variants in the glucocorticoid receptor (GR, NR3C1) and corticotropin releasing hormone receptor 1 (CRHR1) genes with increased risk for PND. Two hundred pregnant women were recruited prospectively and PND risk was assessed by the Edinburgh Postnatal Depression Scale (EPDS) during pregnancy and again 2e8 weeks post-natally (CW-GAPND study). The BclI and ER22/23EK single nucleotide polymorphisms (SNPs) of the GR and the haplotype-tagged rs1876828, rs242939 and rs242941 SNPs of the CRHR1 associated with genetic risk to depressive disorders were genotyped. A cut- off score of 10 was used to detect increased risk of PND. Association analysis was carried out in 140 patients that completed the study protocol. The BclI and rs242939 SNPs were over-represented in women with postnatal EPDS score 10 with significant allele association (p ¼ 0.011 and <0.001, respectively) and risk ratios of 2.9 (95% CI: 1.2e6.9) for BclI, 4.9 (2e12) for rs242939 and 5.48 (2.13 e14.10) for both. The rs242939 SNP was also associated with increased EPDS values during pregnancy. Moreover, the G-G-T haplotype of the CRHR1 was significantly over-represented in patients with high EPDS scores, with risk ratio of 3.22 (95% CI: 1.91e5.42). This is the first evidence that specific SNPs of genes involved in ‘stress’ responses might contribute in the genetics of high-risk for depression during pregnancy and postpartum. Ó 2013 Elsevier Ltd. All rights reserved. 1. Introduction In Western countries postnatal depression (PND) affects approximately 1 in 7 women, whereas in non-Western populations prevalence ranges between 5 and 60% (O’Hara and Swain, 1996; Cooper et al., 1999; Klainin and Arthur, 2009). If left untreated, PND has profound consequences on the quality of family life, social functioning as well as in the long-term emotional and cognitive development of the baby (Grace et al., 2003; Payne, 2007). Most importantly, severe forms of PND, such as puerperal psychosis, which affects 0.1e0.2% of new mothers, are linked to suicide and infanticide (Spinelli, 2009). Despite detailed prevalence statistics, high probabilities of re- experience with future pregnancies, and well documented conse- quences of the disorder, PND remains difficult to identify. Routine assessment for either prenatal depression or PND is not universal. Screening guidelines for PND assessment across healthcare in- stitutions are inconsistent. As a result fewer than half of PND cases are detected by primary healthcare professionals in routine clinical practice (Hearn et al., 1998) and in the UK screening policies rely on opportunistic case finding. The Edinburgh Postnatal Depression Scale (EPDS) which detects high levels of PND symptoms, is a widely used screening tool, however, it cannot be used for prospective identification of women at risk and is not considered to be cost- effective (Paulden et al., 2009). Clearly, PND management and out- comes would benefit substantially from early identification of women at risk and clinically effective treatments available. There is also inconclusive data about the long-term outcome of PND patients; most cases last around 3 months and resolve spontaneously without * Corresponding author. Warwick Medical School, The University of Warwick, Gibbet Hill Road, Coventry, CV4 7AL, UK. Tel.: þ44 2476 968661; fax: þ44 2476 574637. E-mail address: [email protected] (D.K. Grammatopoulos). Contents lists available at SciVerse ScienceDirect Journal of Psychiatric Research journal homepage: www.elsevier.com/locate/psychires 0022-3956/$ e see front matter Ó 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jpsychires.2013.05.003 Journal of Psychiatric Research 47 (2013) 1166e1173
-
Upload
aripinsyarifudin -
Category
Documents
-
view
247 -
download
0
Transcript of hamil, depresi

at SciVerse ScienceDirect
Journal of Psychiatric Research 47 (2013) 1166e1173
Contents lists available
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
Association of glucocorticoid and type 1 corticotropin-releasinghormone receptors gene variants and risk for depression duringpregnancy and post-partum
Neelam Engineer a, Lucy Darwin b, Deole Nishigandh a, Kandala Ngianga-Bakwin c,Steve C. Smith b, Dimitris K. Grammatopoulos b,c,*
aDept of Obstetrics and Gynaecology, UHCW NHS Trust, Coventry, UKbDept of Clinical Biochemistry, UHCW NHS Trust, Coventry, UKcDivision of Metabolic and Vascular Heallth, Warwick Medical School, University of Warwick, Coventry, UK
a r t i c l e i n f o
Article history:Received 29 December 2012Received in revised form27 March 2013Accepted 6 May 2013
Keywords:HPA axisPostnatal depressionCRH receptorGRVariant
* Corresponding author. Warwick Medical School,Gibbet Hill Road, Coventry, CV4 7AL, UK. Tel.: þ44574637.
E-mail address: [email protected]
0022-3956/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.jpsychires.2013.05.003
a b s t r a c t
Women with postnatal depression (PND) appear to have abnormal hypothalamic pituitary adrenal (HPA)axis responses to stress, which might involve a genetic variability component. We investigated associ-ation of genetic variants in the glucocorticoid receptor (GR, NR3C1) and corticotropin releasing hormonereceptor 1 (CRHR1) genes with increased risk for PND. Two hundred pregnant women were recruitedprospectively and PND risk was assessed by the Edinburgh Postnatal Depression Scale (EPDS) duringpregnancy and again 2e8 weeks post-natally (CW-GAPND study). The BclI and ER22/23EK singlenucleotide polymorphisms (SNPs) of the GR and the haplotype-tagged rs1876828, rs242939 andrs242941 SNPs of the CRHR1 associated with genetic risk to depressive disorders were genotyped. A cut-off score of 10 was used to detect increased risk of PND. Association analysis was carried out in 140patients that completed the study protocol. The BclI and rs242939 SNPs were over-represented inwomen with postnatal EPDS score �10 with significant allele association (p ¼ 0.011 and <0.001,respectively) and risk ratios of 2.9 (95% CI: 1.2e6.9) for BclI, 4.9 (2e12) for rs242939 and 5.48 (2.13e14.10) for both. The rs242939 SNP was also associated with increased EPDS values during pregnancy.Moreover, the G-G-T haplotype of the CRHR1 was significantly over-represented in patients with highEPDS scores, with risk ratio of 3.22 (95% CI: 1.91e5.42). This is the first evidence that specific SNPs ofgenes involved in ‘stress’ responses might contribute in the genetics of high-risk for depression duringpregnancy and postpartum.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
In Western countries postnatal depression (PND) affectsapproximately 1 in 7 women, whereas in non-Western populationsprevalence ranges between 5 and 60% (O’Hara and Swain, 1996;Cooper et al., 1999; Klainin and Arthur, 2009). If left untreated, PNDhas profound consequences on the quality of family life, socialfunctioning as well as in the long-term emotional and cognitivedevelopment of the baby (Grace et al., 2003; Payne, 2007). Mostimportantly, severe forms of PND, such as puerperal psychosis,which affects 0.1e0.2% of new mothers, are linked to suicide andinfanticide (Spinelli, 2009).
The University of Warwick,2476 968661; fax: þ44 2476
(D.K. Grammatopoulos).
All rights reserved.
Despite detailed prevalence statistics, high probabilities of re-experience with future pregnancies, and well documented conse-quences of the disorder, PND remains difficult to identify. Routineassessment for either prenatal depression or PND is not universal.Screening guidelines for PND assessment across healthcare in-stitutions are inconsistent. As a result fewer than half of PND casesare detected by primary healthcare professionals in routine clinicalpractice (Hearn et al., 1998) and in the UK screening policies rely onopportunistic case finding. The Edinburgh Postnatal DepressionScale (EPDS)which detects high levels of PND symptoms, is awidelyused screening tool, however, it cannot be used for prospectiveidentification of women at risk and is not considered to be cost-effective (Paulden et al., 2009). Clearly, PND management and out-comes would benefit substantially from early identification ofwomen at risk and clinically effective treatments available. There isalso inconclusivedata about the long-termoutcomeof PNDpatients;most cases last around3months and resolve spontaneouslywithout

N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e1173 1167
treatment. However, several studies demonstrated the presenceof depression, with over 50% lasting over 6 months and some stillbeing present up to 24 months postpartum (Goodman, 2004).
Several psychosocial risk factors for PND have been identified:the strongest predictors are past history of depression and psy-chological disturbance during pregnancy, as well as poor maritalrelationship and low social support, and stressful life events(O’Hara and Swain, 1996). A family history of depression is anotherrisk factor for PND (Murphy-Eberenz et al., 2006), in agreementwith the view that depressive illnesses are associated withhigh heritability, although individual episodes are frequently trig-gered by stressful life events. The later implicates stress-drivenhormonal responses in disease pathogenesis (Spijker & vanRossum, 2009). The maternal hypothalamic-pituitary-adrenal(HPA) axis undergoes gradual changes during pregnancy becauseof an increasing production of placental corticotrophin-releasinghormone (CRH) (Chrousos et al., 1998). The abrupt withdrawal ofplacental CRH at birth results in a re-equilibration of the maternalHPA axis in the days post-delivery. Indeed, women with PNDappear to have abnormal hypothalamic pituitary adrenal (HPA) axisresponses to stress, possibly due to enhanced sensitivity to gonadalsteroids during pregnancy (Magiakou et al., 1996; Bloch et al.,2005). It has been hypothesized that in women with symptoms ofpostpartum “blues” or depression, the HPA axis function fails toreturn to normal post-delivery and exhibits blunted adrenocorti-cotropic hormone (ACTH) responses to CRH challenge at 6 and 12weeks postpartum suggesting prolonged HPA suppression(Magiakou et al., 1996; Rich-Edwards et al., 2008). Recent studies(O’Keane et al., 2011) investigating hormonal changes in the HPAaxis in the days after delivery in relation to daily mood changessuggest that postpartum ’blues’ positively correlated with ACTH;and negatively correlated with oestriol levels during the post-partum days, and with the reduction in CRH concentrations frompregnancy. These findings support the hypothesis that the ’reac-tivation’ of hypothalamic ACTH secretagogue peptides may beinvolved in the aetiology of the disease.
Impaired signalling of key molecules of the HPA axis such as theglucocorticoid receptor (GR) and corticotrophin releasing hormonereceptor type 1 (CRH-R1) has been implicated in the pathogenesisof various depressive disorders including PND (Wisner and Stowe,1997; Kammerer et al., 2006; Brummelte and Galea, 2010). HPAdysfunction has been identified in a wide spectrum of postpartumpsychiatric disorders; for example it has been shown that increasedcirculating ACTH levels but not CRH or cortisol, are associated withthe presence of postpartum thoughts of harming the infant (Labadet al., 2011). Measurement of maternal circulating CRH levels atmid-pregnancy has been proposed as a specific biomarker ofmaternal depression (Rich-Edwards et al., 2008) and this wassupported by other studies suggested that the activity of the HPAaxis during pregnancy is associated with maternal HPA respon-siveness to stress postpartum (Meinlschmidt et al., 2010). However,recent studies yielded contradictory results with positive or noassociation with either prenatal or postpartum depression (Yimet al., 2009; Meltzer-Brody et al., 2011).
The functional anomalies of the HPA axis in depressive disordersappear to include an inherited component due to genetic variability(Spijker & van Rossum, 2009). The genetic contribution to PND andpostpartum psychosis is strongly supported by family and twinstudies and genome-wide linkage analysis in conditions such asbipolar disorder and history of mood or anxiety disorder (Jones andCraddock, 2001; Forty et al., 2006; Jones et al., 2007; Kumar et al.,2007; Payne, 2007; Friedman, 2009; Mahon et al., 2009). Whilethere has been much interest in the identification of genesresponsible for psychiatric illness, there remains a paucity of in-formation relating to molecular markers and detection of PND risk.
The objective of our study was to investigate association be-tween genetic variations (single nucleotide polymorphisms-SNPs)in the GR and CRHR1 genes, previously shown significant correla-tion with depression (Liu et al., 2006; Claes, 2009; Spijker & vanRossum, 2009), and increased risk for PND as determined by araised EPDS score. To address this, a prospective cohort study wasdesigned involving a secondary care University Hospital setting. Toour knowledge, this represents the first prospective investigation ofgenetic variation of genes involved in HPA activity and PND risk.
2. Materials and methods
2.1. Patients-study design
For the Coventry and Warwickshire Genetic Risk for PostNatalDepression (CW-GAPND) study, 200 Caucasian women wererecruited during antenatal clinic visits. The study focused on Cau-casians to ensure ethnic background homogeneity of the cohortsince ethnicity-related differences in PND prevalence have beenreported (O’Hara and Swain, 1996; Patel et al., 2002). Symptomswere assessed using the Edinburgh Postnatal Depression Scale(EPDS) questionnaire, which was completed upon the hospital visitbetween 20 and 28 weeks gestation (mean 25.4�1.9) and again 2e8 weeks post-delivery (mean 4.6 � 2.1). The choice of this time-period was based on previous studies suggesting that incidenceof PND peaks at around 4e6 weeks (Cox et al., 1993; Evans et al.,2001; Verkerk et al., 2003). From the 200 women invited toparticipate, questionnaires were obtained from 140 subjects for areturn rate of 70%. There was no significant difference in the socio-demographic characteristics (educational qualification, maritalstatus, employment, support from partner, subsequent pregnancy)of responders and non-responders. Following current clinicalpractice, there was no follow-up of women who returned EPDSscores below the cut-off of 10.
Recruited patients were assessed for risk factors such as familyhistory (first degree) of depression, personal history of depression,and depressive symptomatology at recruitment using the EPDS,however, there was no stratification to high or low-risk groups inaccordance with current clinical practice. According to standardclinical practice all women were assessed for presence of anaemia(by full blood count and haemoglobin measurement) and thyroiddisease (by TSH measurement) and women with abnormal resultswere excluded from the study. Womenwith a history of depressionbefore pregnancy are especially vulnerable to depressive symptomsduring or after pregnancy (Rich-Edwards et al., 2006). Therefore, inorder to ensure pregnancy-specific and exclude non-pregnancyrelated depressive illness, women with pre-existing mental ill-nesses or on antidepressant medications or any other medicationsthat can influence risk of developing PND were excluded from thestudy. A cut-off EPDS score of 10 was used for the identification ofhigh-risk patients for PND. This reported performance character-istics at this cut-off point is: sensitivity of 0.81 and specificity of0.86 for detection of both major and minor depression and asensitivity of 0.917 and specificity of 0.77 for major depression only(Hewitt et al., 2009). The study was approved by the local ethicscommittee and informed consent was obtained from all subjects.
Similar to previous studies (Fasching et al., 2012; Mehta et al.,2012), the CW-GAPND study protocol included antenatal use ofthe EPDS questionnaire to assess depressive symptoms duringpregnancy between 20 and 28 weeks gestation. Several studiesvalidated the use of EPDS as a pre-screening tool for depressionduring pregnancy especially in the research setting (Rubertssonet al., 2011; Milgrom et al., 2008) although, it is not currentlyused in routine antenatal care in the UK. In this study it was usedexclusively as a research instrument to screen for symptoms of PND
N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e11731168
at antenatal clinics and thus identify presence of pregnancy-relatedunderlying risk.
2.2. Genomic DNA extraction
5mL of peripheral venous bloodwas collected from each subjectin an EDTA tube. Genomic DNA was extracted using the QIAampDNA Mini Kit (Qiagen, UK). The quality of the DNAwas determinedby spectrophotometric analysis using the A260/A280 ratio. Typicallyvalues of intact, high-purity DNA were approximately 1.7e1.8. Incontrast, extracted DNA with ratios below 1.6 or above 2.0 indi-cating possible DNA contamination were excluded.
2.3. SNP selection and genotyping
The glucocorticoid receptor SNPs genotyped were the BclI andER22/23EK (dbSNP NCBI identifiers rs41423247 and rs6190respectively) whereas the 3 CRHR1 SNPs were the rs1876828,rs242939 and rs242941. These were selected from previous reportsthat demonstrated an association with depressive disorders (Liuet al., 2006; van Rossum et al., 2006; Spijker & van Rossum,2009). Genotyping was performed using allele-specific PCR andmelting curve analysis on the LightCycler (Roche Diagnostics Ltd,Burgess Hill, UK). Primers and probes were designed and syn-thesised by TIB MolBiol (Berlin, Germany). The amplificationmixture included 5 mL of genomic DNA as templatewith LightCyclerFastStart DNA Master HybProbe mastermix, primers and probes.LightCycler parameters for PCR and melting curve analysis con-sisted of an initial denaturation step of 95 �C for 10 min followed by
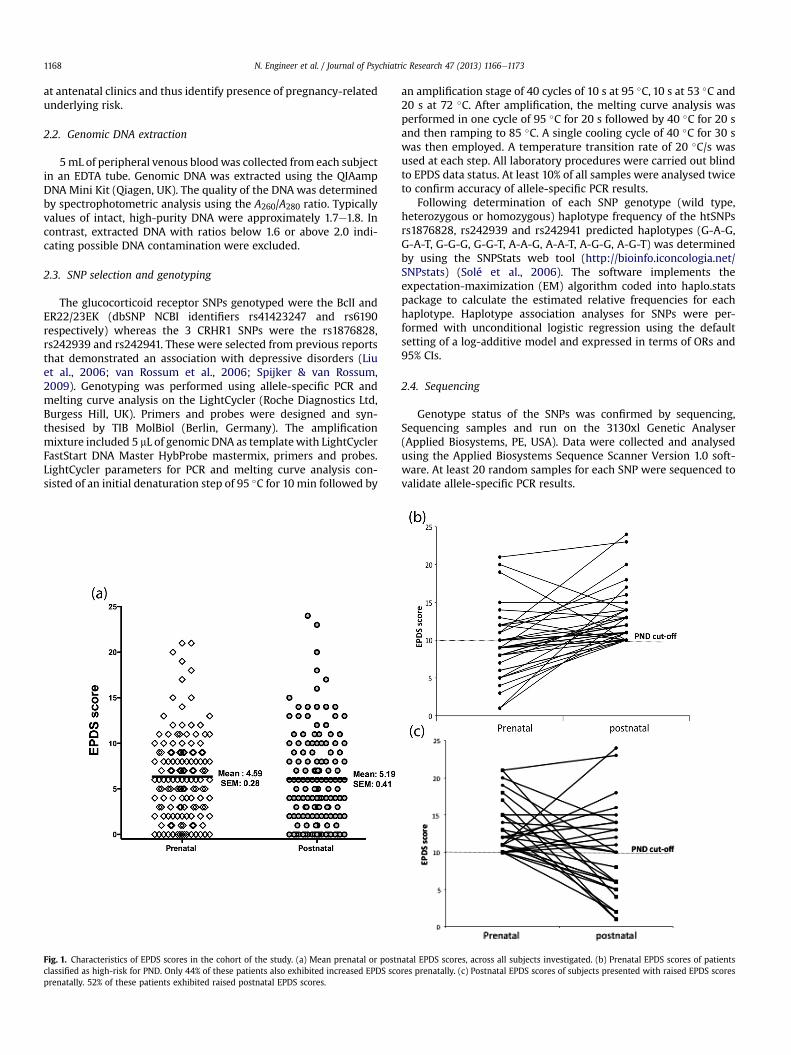
Fig. 1. Characteristics of EPDS scores in the cohort of the study. (a) Mean prenatal or postnclassified as high-risk for PND. Only 44% of these patients also exhibited increased EPDS scoprenatally. 52% of these patients exhibited raised postnatal EPDS scores.
an amplification stage of 40 cycles of 10 s at 95 �C, 10 s at 53 �C and20 s at 72 �C. After amplification, the melting curve analysis wasperformed in one cycle of 95 �C for 20 s followed by 40 �C for 20 sand then ramping to 85 �C. A single cooling cycle of 40 �C for 30 swas then employed. A temperature transition rate of 20 �C/s wasused at each step. All laboratory procedures were carried out blindto EPDS data status. At least 10% of all samples were analysed twiceto confirm accuracy of allele-specific PCR results.
Following determination of each SNP genotype (wild type,heterozygous or homozygous) haplotype frequency of the htSNPsrs1876828, rs242939 and rs242941 predicted haplotypes (G-A-G,G-A-T, G-G-G, G-G-T, A-A-G, A-A-T, A-G-G, A-G-T) was determinedby using the SNPStats web tool (http://bioinfo.iconcologia.net/SNPstats) (Solé et al., 2006). The software implements theexpectation-maximization (EM) algorithm coded into haplo.statspackage to calculate the estimated relative frequencies for eachhaplotype. Haplotype association analyses for SNPs were per-formed with unconditional logistic regression using the defaultsetting of a log-additive model and expressed in terms of ORs and95% CIs.
2.4. Sequencing
Genotype status of the SNPs was confirmed by sequencing,Sequencing samples and run on the 3130xl Genetic Analyser(Applied Biosystems, PE, USA). Data were collected and analysedusing the Applied Biosystems Sequence Scanner Version 1.0 soft-ware. At least 20 random samples for each SNP were sequenced tovalidate allele-specific PCR results.
atal EPDS scores, across all subjects investigated. (b) Prenatal EPDS scores of patientsres prenatally. (c) Postnatal EPDS scores of subjects presented with raised EPDS scores
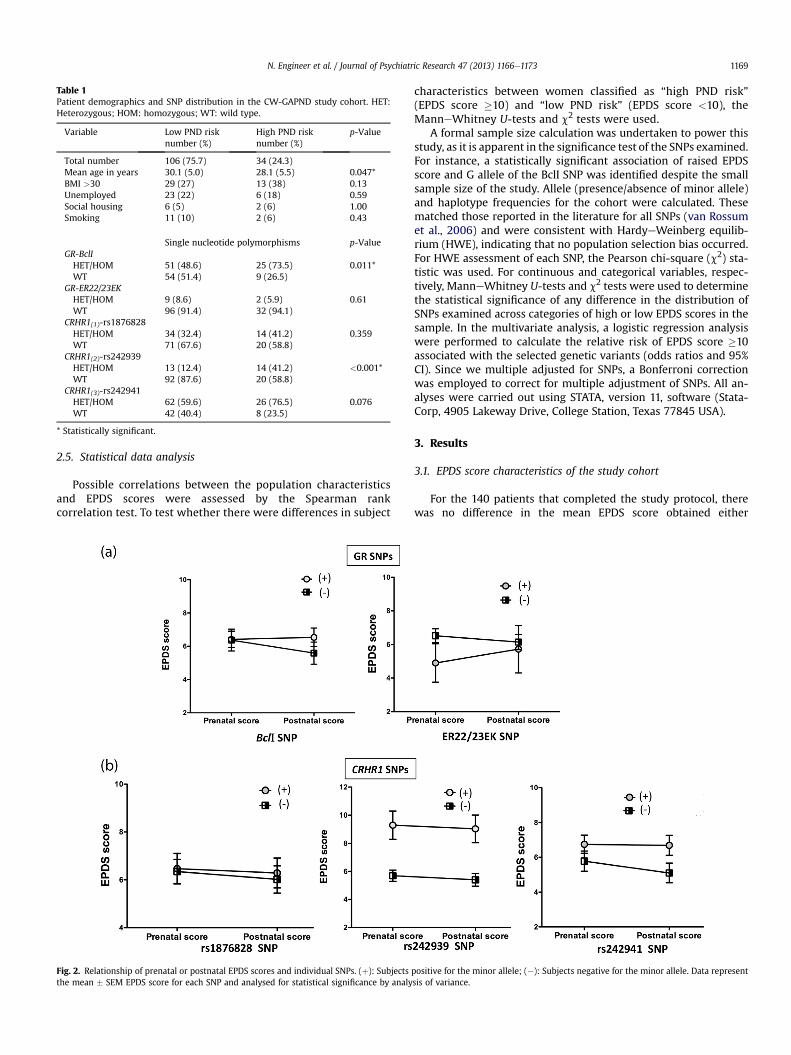
Table 1Patient demographics and SNP distribution in the CW-GAPND study cohort. HET:Heterozygous; HOM: homozygous; WT: wild type.
Variable Low PND risknumber (%)
High PND risknumber (%)
p-Value
Total number 106 (75.7) 34 (24.3)Mean age in years 30.1 (5.0) 28.1 (5.5) 0.047*BMI >30 29 (27) 13 (38) 0.13Unemployed 23 (22) 6 (18) 0.59Social housing 6 (5) 2 (6) 1.00Smoking 11 (10) 2 (6) 0.43
Single nucleotide polymorphisms p-ValueGR-BclIHET/HOM 51 (48.6) 25 (73.5) 0.011*WT 54 (51.4) 9 (26.5)
GR-ER22/23EKHET/HOM 9 (8.6) 2 (5.9) 0.61WT 96 (91.4) 32 (94.1)
CRHR1(1)-rs1876828HET/HOM 34 (32.4) 14 (41.2) 0.359WT 71 (67.6) 20 (58.8)
CRHR1(2)-rs242939HET/HOM 13 (12.4) 14 (41.2) <0.001*WT 92 (87.6) 20 (58.8)
CRHR1(3)-rs242941HET/HOM 62 (59.6) 26 (76.5) 0.076WT 42 (40.4) 8 (23.5)
* Statistically significant.
N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e1173 1169
2.5. Statistical data analysis
Possible correlations between the population characteristicsand EPDS scores were assessed by the Spearman rankcorrelation test. To test whether there were differences in subject
Fig. 2. Relationship of prenatal or postnatal EPDS scores and individual SNPs. (þ): Subjectsthe mean � SEM EPDS score for each SNP and analysed for statistical significance by analy
characteristics between women classified as “high PND risk”(EPDS score �10) and “low PND risk” (EPDS score <10), theManneWhitney U-tests and c2 tests were used.
A formal sample size calculation was undertaken to power thisstudy, as it is apparent in the significance test of the SNPs examined.For instance, a statistically significant association of raised EPDSscore and G allele of the BclI SNP was identified despite the smallsample size of the study. Allele (presence/absence of minor allele)and haplotype frequencies for the cohort were calculated. Thesematched those reported in the literature for all SNPs (van Rossumet al., 2006) and were consistent with HardyeWeinberg equilib-rium (HWE), indicating that no population selection bias occurred.For HWE assessment of each SNP, the Pearson chi-square (c2) sta-tistic was used. For continuous and categorical variables, respec-tively, ManneWhitney U-tests and c2 tests were used to determinethe statistical significance of any difference in the distribution ofSNPs examined across categories of high or low EPDS scores in thesample. In the multivariate analysis, a logistic regression analysiswere performed to calculate the relative risk of EPDS score �10associated with the selected genetic variants (odds ratios and 95%CI). Since we multiple adjusted for SNPs, a Bonferroni correctionwas employed to correct for multiple adjustment of SNPs. All an-alyses were carried out using STATA, version 11, software (Stata-Corp, 4905 Lakeway Drive, College Station, Texas 77845 USA).
3. Results
3.1. EPDS score characteristics of the study cohort
For the 140 patients that completed the study protocol, therewas no difference in the mean EPDS score obtained either
positive for the minor allele; (�): Subjects negative for the minor allele. Data representsis of variance.
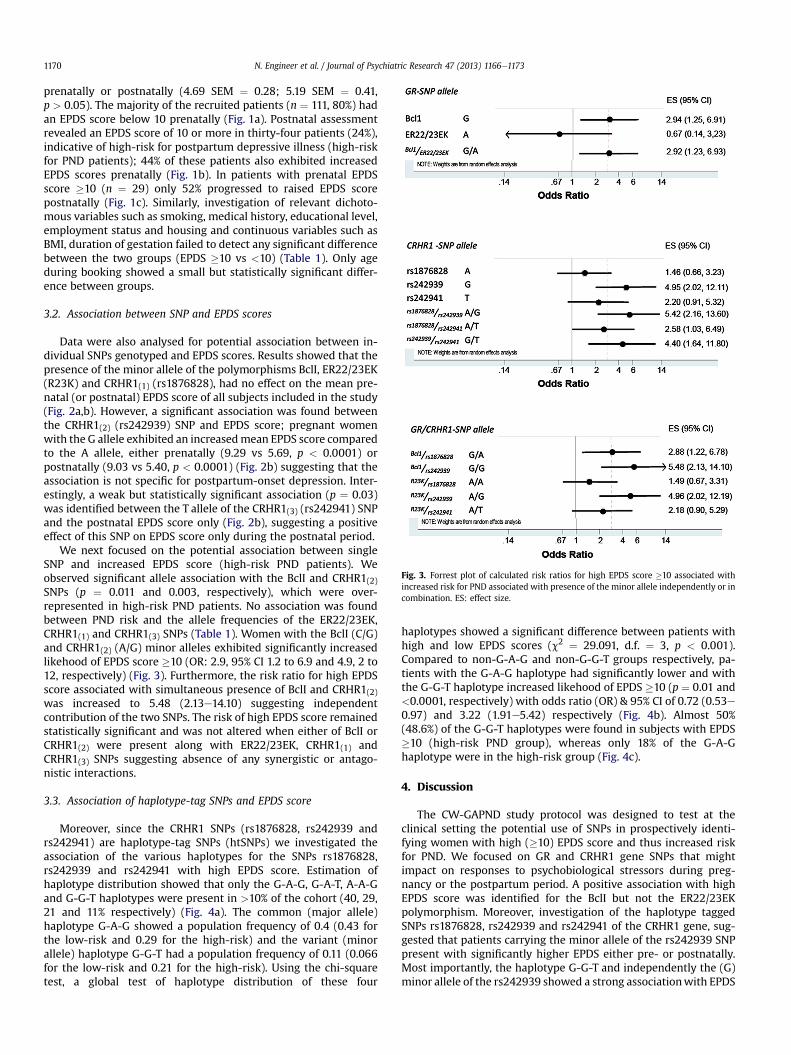
Fig. 3. Forrest plot of calculated risk ratios for high EPDS score �10 associated withincreased risk for PND associated with presence of the minor allele independently or incombination. ES: effect size.
N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e11731170
prenatally or postnatally (4.69 SEM ¼ 0.28; 5.19 SEM ¼ 0.41,p > 0.05). The majority of the recruited patients (n ¼ 111, 80%) hadan EPDS score below 10 prenatally (Fig. 1a). Postnatal assessmentrevealed an EPDS score of 10 or more in thirty-four patients (24%),indicative of high-risk for postpartum depressive illness (high-riskfor PND patients); 44% of these patients also exhibited increasedEPDS scores prenatally (Fig. 1b). In patients with prenatal EPDSscore �10 (n ¼ 29) only 52% progressed to raised EPDS scorepostnatally (Fig. 1c). Similarly, investigation of relevant dichoto-mous variables such as smoking, medical history, educational level,employment status and housing and continuous variables such asBMI, duration of gestation failed to detect any significant differencebetween the two groups (EPDS �10 vs <10) (Table 1). Only ageduring booking showed a small but statistically significant differ-ence between groups.
3.2. Association between SNP and EPDS scores
Data were also analysed for potential association between in-dividual SNPs genotyped and EPDS scores. Results showed that thepresence of the minor allele of the polymorphisms BclI, ER22/23EK(R23K) and CRHR1(1) (rs1876828), had no effect on the mean pre-natal (or postnatal) EPDS score of all subjects included in the study(Fig. 2a,b). However, a significant association was found betweenthe CRHR1(2) (rs242939) SNP and EPDS score; pregnant womenwith the G allele exhibited an increasedmean EPDS score comparedto the A allele, either prenatally (9.29 vs 5.69, p < 0.0001) orpostnatally (9.03 vs 5.40, p < 0.0001) (Fig. 2b) suggesting that theassociation is not specific for postpartum-onset depression. Inter-estingly, a weak but statistically significant association (p ¼ 0.03)was identified between the T allele of the CRHR1(3) (rs242941) SNPand the postnatal EPDS score only (Fig. 2b), suggesting a positiveeffect of this SNP on EPDS score only during the postnatal period.
We next focused on the potential association between singleSNP and increased EPDS score (high-risk PND patients). Weobserved significant allele association with the BclI and CRHR1(2)SNPs (p ¼ 0.011 and 0.003, respectively), which were over-represented in high-risk PND patients. No association was foundbetween PND risk and the allele frequencies of the ER22/23EK,CRHR1(1) and CRHR1(3) SNPs (Table 1). Women with the BclI (C/G)and CRHR1(2) (A/G) minor alleles exhibited significantly increasedlikehood of EPDS score �10 (OR: 2.9, 95% CI 1.2 to 6.9 and 4.9, 2 to12, respectively) (Fig. 3). Furthermore, the risk ratio for high EPDSscore associated with simultaneous presence of BclI and CRHR1(2)was increased to 5.48 (2.13e14.10) suggesting independentcontribution of the two SNPs. The risk of high EPDS score remainedstatistically significant and was not altered when either of BclI orCRHR1(2) were present along with ER22/23EK, CRHR1(1) andCRHR1(3) SNPs suggesting absence of any synergistic or antago-nistic interactions.
3.3. Association of haplotype-tag SNPs and EPDS score
Moreover, since the CRHR1 SNPs (rs1876828, rs242939 andrs242941) are haplotype-tag SNPs (htSNPs) we investigated theassociation of the various haplotypes for the SNPs rs1876828,rs242939 and rs242941 with high EPDS score. Estimation ofhaplotype distribution showed that only the G-A-G, G-A-T, A-A-Gand G-G-T haplotypes were present in >10% of the cohort (40, 29,21 and 11% respectively) (Fig. 4a). The common (major allele)haplotype G-A-G showed a population frequency of 0.4 (0.43 forthe low-risk and 0.29 for the high-risk) and the variant (minorallele) haplotype G-G-T had a population frequency of 0.11 (0.066for the low-risk and 0.21 for the high-risk). Using the chi-squaretest, a global test of haplotype distribution of these four
haplotypes showed a significant difference between patients withhigh and low EPDS scores (c2 ¼ 29.091, d.f. ¼ 3, p < 0.001).Compared to non-G-A-G and non-G-G-T groups respectively, pa-tients with the G-A-G haplotype had significantly lower and withthe G-G-T haplotype increased likehood of EPDS �10 (p ¼ 0.01 and<0.0001, respectively) with odds ratio (OR) & 95% CI of 0.72 (0.53e0.97) and 3.22 (1.91e5.42) respectively (Fig. 4b). Almost 50%(48.6%) of the G-G-T haplotypes were found in subjects with EPDS�10 (high-risk PND group), whereas only 18% of the G-A-Ghaplotype were in the high-risk group (Fig. 4c).
4. Discussion
The CW-GAPND study protocol was designed to test at theclinical setting the potential use of SNPs in prospectively identi-fying women with high (�10) EPDS score and thus increased riskfor PND. We focused on GR and CRHR1 gene SNPs that mightimpact on responses to psychobiological stressors during preg-nancy or the postpartum period. A positive association with highEPDS score was identified for the BclI but not the ER22/23EKpolymorphism. Moreover, investigation of the haplotype taggedSNPs rs1876828, rs242939 and rs242941 of the CRHR1 gene, sug-gested that patients carrying the minor allele of the rs242939 SNPpresent with significantly higher EPDS either pre- or postnatally.Most importantly, the haplotype G-G-T and independently the (G)minor allele of the rs242939 showed a strong associationwith EPDS
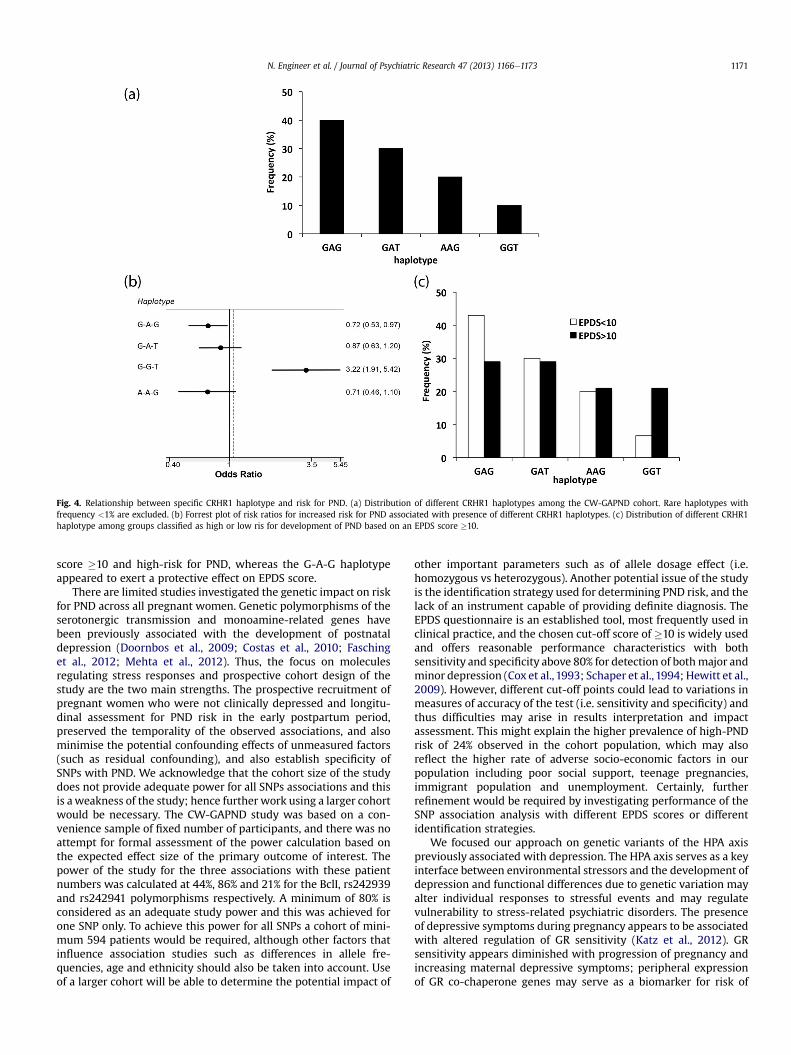
Fig. 4. Relationship between specific CRHR1 haplotype and risk for PND. (a) Distribution of different CRHR1 haplotypes among the CW-GAPND cohort. Rare haplotypes withfrequency <1% are excluded. (b) Forrest plot of risk ratios for increased risk for PND associated with presence of different CRHR1 haplotypes. (c) Distribution of different CRHR1haplotype among groups classified as high or low ris for development of PND based on an EPDS score �10.
N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e1173 1171
score �10 and high-risk for PND, whereas the G-A-G haplotypeappeared to exert a protective effect on EPDS score.
There are limited studies investigated the genetic impact on riskfor PND across all pregnant women. Genetic polymorphisms of theserotonergic transmission and monoamine-related genes havebeen previously associated with the development of postnataldepression (Doornbos et al., 2009; Costas et al., 2010; Faschinget al., 2012; Mehta et al., 2012). Thus, the focus on moleculesregulating stress responses and prospective cohort design of thestudy are the two main strengths. The prospective recruitment ofpregnant women who were not clinically depressed and longitu-dinal assessment for PND risk in the early postpartum period,preserved the temporality of the observed associations, and alsominimise the potential confounding effects of unmeasured factors(such as residual confounding), and also establish specificity ofSNPs with PND. We acknowledge that the cohort size of the studydoes not provide adequate power for all SNPs associations and thisis aweakness of the study; hence further work using a larger cohortwould be necessary. The CW-GAPND study was based on a con-venience sample of fixed number of participants, and there was noattempt for formal assessment of the power calculation based onthe expected effect size of the primary outcome of interest. Thepower of the study for the three associations with these patientnumbers was calculated at 44%, 86% and 21% for the BclI, rs242939and rs242941 polymorphisms respectively. A minimum of 80% isconsidered as an adequate study power and this was achieved forone SNP only. To achieve this power for all SNPs a cohort of mini-mum 594 patients would be required, although other factors thatinfluence association studies such as differences in allele fre-quencies, age and ethnicity should also be taken into account. Useof a larger cohort will be able to determine the potential impact of
other important parameters such as of allele dosage effect (i.e.homozygous vs heterozygous). Another potential issue of the studyis the identification strategy used for determining PND risk, and thelack of an instrument capable of providing definite diagnosis. TheEPDS questionnaire is an established tool, most frequently used inclinical practice, and the chosen cut-off score of �10 is widely usedand offers reasonable performance characteristics with bothsensitivity and specificity above 80% for detection of bothmajor andminor depression (Cox et al., 1993; Schaper et al., 1994; Hewitt et al.,2009). However, different cut-off points could lead to variations inmeasures of accuracy of the test (i.e. sensitivity and specificity) andthus difficulties may arise in results interpretation and impactassessment. This might explain the higher prevalence of high-PNDrisk of 24% observed in the cohort population, which may alsoreflect the higher rate of adverse socio-economic factors in ourpopulation including poor social support, teenage pregnancies,immigrant population and unemployment. Certainly, furtherrefinement would be required by investigating performance of theSNP association analysis with different EPDS scores or differentidentification strategies.
We focused our approach on genetic variants of the HPA axispreviously associated with depression. The HPA axis serves as a keyinterface between environmental stressors and the development ofdepression and functional differences due to genetic variation mayalter individual responses to stressful events and may regulatevulnerability to stress-related psychiatric disorders. The presenceof depressive symptoms during pregnancy appears to be associatedwith altered regulation of GR sensitivity (Katz et al., 2012). GRsensitivity appears diminished with progression of pregnancy andincreasing maternal depressive symptoms; peripheral expressionof GR co-chaperone genes may serve as a biomarker for risk of

N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e11731172
developing depressive symptoms during pregnancy. The GR geneSNPs investigated such as the BclI and ER22/23EK are linked withclinical phenotypes, possibly due to altered function of GR andtherefore may increase the risk of depressive disorders by alteringcortisol responses to psychosocial stress (Spijker & van Rossum,2009). In particular the ER22/23EK SNP has been reported torelate to decreased cortisol suppression to dexamethasoneadministration (van Rossum and Lamberts, 2004), whereas the BclIpolymorphism seems to be associated with attenuated cortisolresponses. Interestingly, our study identified a significant associa-tion with high PND risk of only the G minor allele of the BclI SNP,found despite no effect on the prenatal or postnatal EPDS score, afinding that is consistent with results from non-pregnantdepressed population (van Rossum et al., 2006). Similar findingshave also reported in a group of pre-menopausal women andsuggested that homozygous carriers of both BclI and ER22/23EKSNPs have increased risk of developing a major depressive episode(van Rossum and Lamberts, 2004; Krishnamurthy et al., 2008). Thelack of association between the ER22/23EK SNP and high EPDSscore in our study suggests that patients at risk for PND mightrepresent a subgroup with distinct geneeenvironment interactionsand unique genetic characteristics that exhibit increased vulnera-bility to pregnancy-associated triggers. The high-risk PND group ofthe CW-GAPND cohort also exhibited a strong association withrs242939, a CRHR1 SNP previously been associated with majordepression in a group of Han Chinese patients (Liu et al., 2006). Infact this SNP was associated with raised EPDS values both beforeand after delivery and were thus not specific for postpartum-onsetdepression. It is increasingly recognised that multiple genetic var-iations with discrete functional effects in a number of genes regu-lating the HPA axis may alter susceptibility to stress-relatedpsychiatric disorders and a system genetics approach is required tofully elucidate the impact of gene � environment interactions.There is already evidence for the association of genetic variants ingenes intricately tied to the CRH system with depression andanxiety, such as the GR gene or the serotonin transporter (Ressleret al., 2010). In agreement with this, we noted a combined effectof the simultaneous presence of the BclI and rs242939 SNPs thatappeared to further increase the odds of raised EPDS score and highPND risk, raising the possibility of gene � gene interactions be-tween CRHR1 and GR loci.
The CW-GAPND study provides the first preliminary evidence ofgenetic association between gene variants of the ‘stress’ endocrineaxis and risk for depression during pregnancy and post-partum. Italso offers additional benefits in understanding the biological basisof disease. Polymorphisms of genes regulating stress responsesappear to be promising targets for further investigations. Certainly,a larger prospective study of a replication sample that will include astructured diagnostic interview is required to fully explore themagnitude of this genetic effect and potential usefulness indetection and management of postnatal depression.
Funding body agreements and policies
No specific requirements as specified as conditions of the grantawards supported this research.
Contributions
N.E contributed to the design of study, recruitment of patientsand collection of clinical details, data analysis and manuscriptpreparation; L.D contributed to the molecular methods develop-ment, performed the experiments and data analysis and managedthe literature searches; D.N contributed to the recruitment ofpatients, collection of clinical details and data analysis; K.N-B
undertook data statistical analysis and manuscript preparation;S.C.S contributed to the design of study, data analysis and manu-script preparation; D.K.G. contributed to the design of the study,guided data interpretation and manuscript writing. All authorshave approved the submitted version.
Author disclosure
The authors have no conflict of interest to disclose.
Acknowledgements
The principal investigator confirms that he had full access to allof the data in the study and takes responsibility for the integrity ofthe data and the accuracy of the data analysis. Research supportedby the Robert Gaddie Memorial Fund and the Birmingham-War-wick Science City Research Alliance.
References
Bloch M, Rubinow DR, Schmidt PJ, Lotsikas A, Chrousos GP, Cizza G. Cortisolresponse to ovine corticotropin-releasing hormone in a model of pregnancyand parturition in euthymic women with and without a history of postpartumdepression. Journal of clinical endocrinology and metabolism 2005;90:695e9.
Brummelte S, Galea LA. Depression during pregnancy and postpartum: contributionof stress and ovarian hormones. Progress in Neuro-Psychopharmacology &Biological Psychiatry 2010;34:766e76.
Chrousos GP, Torpy DJ, Gold PW. Interactions between the hypothalamic-pituitary-adrenal axis and the female reproductive system: clinical implications. Annalsof Internal Medicine 1998;129:229e40.
Claes S. Glucocorticoid receptor polymorphisms in major depression. Annals of theNew York Academy of Sciences 2009;1179:216e28.
Cooper PJ, Tomlinson M, Swartz L, Woolgar M, Murray L, Molteno C. Postpartumdepression and the mother-infant relationship in a South African per-urbansettlement. British Journal of Psychiatry 1999;175:554e8.
Costas J, Gratacòs M, Escaramís G, Martín-Santos R, de Diego Y, Baca-García E, et al.Association study of 44 candidate genes with depressive and anxiety symptomsin post-partum women. Journal of Psychiatric Research 2010;44:717e24.
Cox JL, Murray D, Chapman G. A controlled study of the onset, duration andprevalence of postnatal depression. British Journal of Psychiatry 1993;163:27e31.
Doornbos B, Dijck-Brouwer DA, Kema IP, Tanke MA, van Goor SA, Muskiet FA, et al.The development of peripartum depressive symptoms is associated with genepolymorphisms of MAOA, 5-HTT and COMT. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2009;33:1250e4.
Evans J, Heron J, Francomb H, Oke S, Golding J. Cohort study of depressed moodduring pregnancy and after childbirth. British Medical Journal 2001;323:257e60.
Fasching PA, Faschingbauer F, Goecke TW, Engel A, Häberle L, Seifert A, et al. Geneticvariants in the tryptophan hydroxylase 2 gene (TPH2) and depression duringand after pregnancy. Journal of Psychiatric Research 2012;46:1109e17.
Forty L, Jones L, Macgregor S, Caesar S, Cooper C, Hough A, et al. Familiality ofpostpartum depression in unipolar disorder: results of a family study. AmericanJournal of Psychiatry 2006;163:1549e53.
Friedman SH. Postpartum mood disorders: genetic progress and treatment para-digms. American Journal of Psychiatry 2009;166:1201e4.
Grace SL, Evindar A, Stewart DE. The effect of postpartum depression on childcognitive development and behavior: a review and critical analysis of theliterature. Archives Womens Mental Health 2003;6:263e74.
Goodman J. Postpartum depression beyond the early postpartum period. Journal ofObstetric, Gynecologic, & Neonatal Nursing 2004;33:410e20.
Hearn G, lliff A, Jones I, Kirby A, Ormiston P, Parr P, et al. Postnatal depression in thecommunity. British Journal of General Practice 1998;48:1064e6.
Hewitt C, Gilbody S, Brealey S, Paulden M, Palmer S, Mann R, et al. Methods toidentify postnatal depression in primary care: an integrated evidence synthesisand value of information analysis. Health Technology Assessment 2009;13:147e230.
Jones I, Craddock N. Familiality of the puerperal trigger in bipolar disorder: resultsof a family study. American Journal of Psychiatry 2001;158:913e7.
Jones I, Hamshere M, Nangle JM, Bennett P, Green E, Heron J, et al. Bipolar affectivepuerperal psychosis: genome-wide significant evidence for linkage to chro-mosome 16. American Journal of Psychiatry 2007;164:1099e104.
Kammerer M, Taylor A, Glover V. The HPA axis and perinatal depression: ahypothesis. Archives Womens Mental Health 2006;9:187e96.
Katz ER, Stowe ZN, Newport DJ, Kelley ME, Pace TW, Cubells JF, et al. Regulation ofmRNA expression encoding chaperone and co-chaperone proteins of theglucocorticoid receptor in peripheral blood: association with depressivesymptoms during pregnancy. Psychological Medicine 2012;42:943e56.
N. Engineer et al. / Journal of Psychiatric Research 47 (2013) 1166e1173 1173
Klainin P, Arthur DG. Postpartum depression in Asian cultures: a literature review.International Journal of Nursing Studies 2009;46:1355e73.
Krishnamurthy P, Romagni P, Torvik S, Gold PW, Charney DS, Detera-Wadleigh S,et al., P.O.W.E.R. (Premenopausal, Osteoporosis Women, Alendronate, Depres-sion) Study Group. Glucocorticoid receptor gene polymorphisms in premeno-pausal women with major depression. Hormone and Metabolic Research2008;40:194e8.
Kumar HB, PurushottamM, Kubendran S, Gayathri P, Mukherjee O, Murthy AR, et al.Serotonergic candidate genes and puerperal psychosis: an association study.Psychiatric Genetics 2007;17:253e60.
Labad J, Viella E, Reynolds RM, Sans T, Cavalle P, Valero J, et al. Increased morningadrenocorticotrophin hormone (ACTH) levels in women with postpartumthoughts of harming the infant. Psychoneuroendocrinology 2011;36:924e8.
Liu Z, Zhu F, Wang G, Xiao Z, Wang H, Tang J, et al. Association of corticotropin-releasing hormone receptor 1 gene SNP and haplotype with major depres-sion. Neuroscience Letters 2006;404:358e62.
Mahon PB, Payne JL, MacKinnon DF, Mondimore FM, Goes FS, Schweizer B, et al.,NIMH Genetics Initiative Bipolar Disorder Consortium; BiGS Consortium.Genome-wide linkage and follow-up association study of postpartum moodsymptoms. American Journal of Psychiatry 2009;166:1229e37.
Magiakou M, Mastorakos G, Rabin D, Dubbert B, Gold P. Hypothalamiccorticotropin-releasing hormone suppression during the post-partum period:implications for the increase in psychiatric manifestations at this time. Journalof Clinical Endocrinology & Metabolism 1996;81:1912e7.
Mehta D, Quast C, Fasching PA, Seifert A, Voigt F, Beckmann MW, et al. The 5-HTTLPR polymorphism modulates the influence on environmental stressors onperipartum depression symptoms. Journal of Affective Disorders 2012;136:1192e7.
Meltzer-Brody S, Stuebe A, Dole N, Savitz D, Rubinow D, Thorp J. Elevated corti-cotropin releasing hormone (CRH) during pregnancy and risk of postpartumdepression (PPD). Journal of Clinical Endocrinology & Metabolism 2011;96:E40e7.
Meinlschmidt G, Martin C, Neumann ID, Heinrichs M. Maternal cortisol in latepregnancy and hypothalamic-pituitary-adrenal reactivity to psychosocial stresspostpartum in women. Stress 2010;13:163e71.
Milgrom J, Gemmill AW, Bilszta JL, Hayes B, Barnett B, Brooks J, et al. Antenatal riskfactors for postnatal depression: a large prospective study. Journal of AffectiveDisorders 2008;108:147e57.
Murphy-Eberenz K, Zandi PP, March D, Crowe RR, Scheftner WA, Alexander M, et al.Is perinatal depression familial? Journal of Affective Disorders 2006;90:49e55.
O’Hara MW, Swain AM. Rates and risk of postnatal depression e a meta-analysis.International Review of Psychiatry 1996;8:37e54.
O’Keane V, Lightman S, Patrick K, Marsh M, Papadopoulos AS, Pawlby S, et al.Changes in the maternal hypothalamic-pituitary-adrenal axis during the earlypuerperium may be related to the postpartum ‘blues’. Journal of Neuroendo-crinology 2011;23:1149e55.
Patel V, Rodrigues M, DeSouza N. Gender, poverty and postnatal depression: a studyof mothers in Goa, India. American Journal of Psychiatry 2002;159:43e7.
Paulden M, Palmer S, Hewitt C, Gilbody S. Screening for postnatal depression inprimary care: cost effectiveness analysis. British Medical Journal 2009:339[b5203].
Payne JL. Antidepressant use in the postpartum period: practical considerations.American Journal of Psychiatry 2007;164:1329e32.
Ressler KJ, Bradley B, Mercer KB, Deveau TC, Smith AK, Gillespie CF, et al. Poly-morphisms in CRHR1 and the serotonin transporter loci: gene � gene � envi-ronment interactions on depressive symptoms. American Journal of MedicalGenetics Part B: Neuropsychiatric Genetics 2010;153B:812e24.
Rich-Edwards JW, Kleinman K, Abrams A, Harlow BL, McLaughlin TJ, Joffe H, et al.Sociodemographic predictors of antenatal and postpartum depressive symp-toms among women in a medical group practice. Journal of Epidemiology &Community Health 2006;60:221e7.
Rich-Edwards JW, Mohllajee AP, Kleinman K, Hacker MR, Majzoub J, Wright RJ, et al.Elevated midpregnancy corticotropin-releasing hormone is associated withprenatal, but not postpartum, maternal depression. Journal of Clinical Endo-crinology & Metabolism 2008;93:1946e51.
van Rossum EF, Binder EB, Majer M, Koper JW, Ising M, Modell S, et al. Poly-morphisms of the glucocorticoid receptor gene and major depression. BiologicalPsychiatry 2006;59:681e8.
van Rossum EF, Lamberts SW. Polymorphisms in the glucocorticoid receptor geneand their associations with metabolic parameters and body composition.Recent Progress in Hormone Research 2004;59:333e57.
Rubertsson C, Bàrjesson K, Berglund A, Josefsson A, Sydsjà G. The Swedish valida-tion of Edinburgh postnatal depression Scale (EPDS) during pregnancy. NordicJournal of Psychiatry 2011;65:414e8.
Schaper AM, Rooney BL, Kay NR, Silva PD. Use of the Edinburgh PostnatalDepression Scale to identify postpartum depression in a clinical setting. Journalof Reproductive Medicine 1994;39:620e4.
Solé X, Guinó E, Valls J, Iniesta R, Moreno V. SNPStats: a web tool for the analysis ofassociation studies. Bioinformatics 2006;22:1928e9.
Spijker AT, van Rossum EFC. Glucocorticoid receptor polymorphisms in majordepression. Annals of the New York Academy of Sciences 2009;1179:199e215.
Spinelli MG. Postpartum psychosis: detection of risk and management. AmericanJournal of Psychiatry 2009;166:405e8.
Verkerk GJM, Pop VJM, Van Son MJM, Van Heck GLV. Prediction of depression in thepostpartum period: a longitudinal follow up study in high-risk and low-riskwomen. Journal of Affective Disorders 2003;77:159e66.
Wisner KL, Stowe ZN. Psychobiology of postpartum mood disorders. Seminars inReproductive Endocrinology 1997;15:77e89.
Yim IS, Glynn LM, Dunkel-Schetter C, Hobel CJ, Chicz-DeMet A, Sandman CA.Risk of postpartum depressive symptoms with elevated corticotropin-releasing hormone in human pregnancy. Archives of General Psychiatry2009;66:162e9.