Gastrooesepageal Refluks
29
Gastrooesepageal Refluks atau Sering Muntah Pada Anak Karena Pengaruh Alergi atau Hipersensitif Makanan Latar Belakang Audi, laki-laki usia 2 tahun sejak lahir hingga sekarang , sering mengalami muntah, meski dengan pertambahan usia berangsur berkurang. Setelah usia 9-12 bulan mulai timbul gangguan mengunyah dan menelan sehingga hanya mau minum susu dan makan harus diblender. Selain itu Audi mudah sekali terserang demam, batuk dan pilek. Selain mengalami gangguan tidur malam, dia juga mengalami keterlambatan bicara atau bila bicara tidak jelas dan gangguan perkembangan motorik kasar dan gangguan keseimbangan (usia 6-8 bulan tidak duduk dan merangkak, jalan terlambat, dan setelah bisa berjalan jalan sering terjatuh atau goyang) . Setelah itu dokter mengadviskan untuk dilakukan penanganan alergi dan hipersensitifitas makanan dengan menghindari sementara beberapa makanan yang diduga penyebab alergi makanan ternyata tidak dalam waktu lama keluhan muntah membaik, daya tahan tubuhnya semakin dan beberapa keluhan lainnya yang menyertai membaik. Amati Gangguan Gastroesophageal Refluks dan Sering muntah pada anak anda Pada usia bayi di bawah 6 bulan sering muntah dan gumoh. Setelah usia 6 bulan hingga 2 tahun berkurang. Pada kasus tertentu membaik setelah usia 5 – 7 tahun Muntah atau mual timbul saat berlari, menangis, batuk, memasukkan tangan ke mulut, tercium bau tajam (bau tidak enak, bau amis atau terlalu wangi) Gangguan lain yang sering Menyertai Gangguan mengunyah menelan : Tidak menyukai variasi banyak makanan, tidak mau makan nasi hanya minum susu.
-
Upload
riani-youfvie -
Category
Documents
-
view
251 -
download
6
Transcript of Gastrooesepageal Refluks

Gastrooesepageal Refluks atau Sering Muntah Pada Anak
Karena Pengaruh Alergi atau Hipersensitif Makanan
Latar Belakang
Audi, laki-laki usia 2 tahun sejak lahir hingga sekarang , sering mengalami muntah, meski dengan pertambahan usia berangsur berkurang. Setelah usia 9-12 bulan mulai timbul gangguan mengunyah dan menelan sehingga hanya mau minum susu dan makan harus diblender. Selain itu Audi mudah sekali terserang demam, batuk dan pilek. Selain mengalami gangguan tidur malam, dia juga mengalami keterlambatan bicara atau bila bicara tidak jelas dan gangguan perkembangan motorik kasar dan gangguan keseimbangan (usia 6-8 bulan tidak duduk dan merangkak, jalan terlambat, dan setelah bisa berjalan jalan sering terjatuh atau goyang) . Setelah itu dokter mengadviskan untuk dilakukan penanganan alergi dan hipersensitifitas makanan dengan menghindari sementara beberapa makanan yang diduga penyebab alergi makanan ternyata tidak dalam waktu lama keluhan muntah membaik, daya tahan tubuhnya semakin dan beberapa keluhan lainnya yang menyertai membaik.
Amati Gangguan Gastroesophageal Refluks dan Sering muntah pada anak anda
Pada usia bayi di bawah 6 bulan sering muntah dan gumoh. Setelah usia 6 bulan hingga 2 tahun berkurang. Pada kasus tertentu membaik setelah usia 5 – 7 tahun
Muntah atau mual timbul saat berlari, menangis, batuk, memasukkan tangan ke mulut, tercium bau tajam (bau tidak enak, bau amis atau terlalu wangi)
Gangguan lain yang sering Menyertai
Gangguan mengunyah menelan : Tidak menyukai variasi banyak makanan, tidak mau makan nasi hanya minum susu. Sering pilih-pilih makanan. Makanan yang disukai adalah makanan yang gampang dikunyah seperti telor, mi, krupuk, biskuit, brokoli, wortel. tetapi makanan yang berserat seperti daging sapi, sayur, atau nasi lebih tidak disukai.
Sebagian Besar kasus anak berat badannya lebih atau kegemukan sebagian kecil lainnya sebaliknya sulit naik berat badan
Gangguan Motorik kasar dan keseimbangan Gangguan sensoris : sensitif terhadap suara (frekuensi tinggi) , cahaya (mudah
silau), perabaan telapak kaki dan tangan sensitif (jalan jinjit, flat foot, mudah geli, mudah jijik, tidak suka memegang bulu, boneka dan bianatang berbulu)

Daya tahan menurun sering sakit demam, batuk, pilek setiap bulan bahkan sebulan 2 kali (normal sakit seharusnya 2-3 bulan sekali)
Emosi tinggi, keras kepala (sering membantah) dan gangguan konsentrasi
Amati Tanda dan gejala gangguan saluran cerna yang lain karena alergi dan hipersensitif makanan (Gastrointestinal Hipersensitivity)
(Gejala Gangguan Fungsi saluran cerna yang ada selama ini sering dianggap normal)
Pada Bayi : GASTROOESEPHAGEAL REFLUKS ATAU GER, Sering MUNTAH/gumoh, kembung,“cegukan”, buang angin keras dan sering, sering rewel gelisah (kolik) terutama malam hari, BAB > 3 kali perhari, BAB tidak tiap hari. Feses warna hijau,hitam dan berbau. Sering “ngeden & beresiko Hernia Umbilikalis (pusar), Scrotalis, inguinalis. Air liur berlebihan. Lidah/mulut sering timbul putih, bibir kering
Pada anak yang lebih besar :
1. Mudah MUNTAH bila menangis, berlari atau makan banyak. MUAL pagi hari.2. Sering Buang Air Besar (BAB) 3 kali/hari atau lebih, sulit BAB sering
ngeden kesakitan saat BAB (obstipasi). Kotoran bulat kecil hitam seperti kotoran kambing, keras, warna hitam, hijau dan bau tajam. sering buang angin, berak di celana. Sering KEMBUNG, sering buang angin dan bau tajam. Sering NYERI PERUT, tidur malam nungging (biasanya karena perut tidak nyaman)
3. Nyeri gigi, gigi berwarna kuning kecoklatan, gigi rusak, gusi mudah bengkak/berdarah. Bibir kering dan mudah berdarah, sering SARIAWAN, lidah putih & berpulau, mulut berbau, air liur berlebihan.
MANIFESTASI KLINIS YANG SERING MENYERTAI ALERGI DAN HIPERSENSITIFITAS MAKANAN PADA BAYI :
KULIT : sering timbul bintik kemerahan terutama di pipi, telinga dan daerah yang tertutup popok. Kerak di daerah rambut. Timbul bekas hitam seperti tergigit nyamuk. Kotoran telinga berlebihan & berbau. Bekas suntikan BCG bengkak dan bernanah. Timbul bisul.
SALURAN NAPAS : Napas grok-grok, kadang disertai batuk ringan. Sesak pada bayi baru lahir disertai kelenjar thimus membesar (TRDN/TTNB)
HIDUNG : Bersin, hidung berbunyi, kotoran hidung banyak, kepala sering miring ke salah satu sisi karena salah satu sisi hidung buntu, sehingga beresiko ”KEPALA PEYANG”.
MATA : Mata berair atau timbul kotoran mata (belekan) salah satu sisi. KELENJAR : Pembesaran kelenjar di leher dan kepala belakang bawah. PEMBULUH DARAH : telapak tangan dan kaki seperti pucat, sering terba
dingin GANGGUAN HORMONAL : keputihan/keluar darah dari vagina, timbul bintil
merah bernanah, pembesaran payudara, rambut rontok.

PERSARAFAN : Mudah kaget bila ada suara keras. Saat menangis : tangan, kaki dan bibir sering gemetar atau napas tertahan/berhenti sesaat (breath holding spells)
PROBLEM MINUM ASI : minum berlebihan, berat berlebihan krn bayi sering menangis dianggap haus (haus palsu : sering menangis belum tentu karena haus atau bukan karena ASI kurang.). Sering menggigit puting sehingga luka. Minum ASI sering tersedak, karena hidung buntu & napas dengan mulut. Minum ASI lebih sebentar pada satu sisi,`karena satu sisi hidung buntu, jangka panjang bisa berakibat payudara besar sebelah.
MANIFESTASI KLINIS YANG SERING MENYERTAI ALERGI DAN HIPERSENSITIFITAS MAKANAN PADA ANAK
SALURAN NAPAS DAN HIDUNG : Batuk / pilek lama (>2 minggu), ASMA, bersin, hidung buntu, terutama malam dan pagi hari. MIMISAN, suara serak, SINUSITIS, sering menarik napas dalam.
KULIT : Kulit timbul BISUL, kemerahan, bercak putih dan bekas hitam seperti tergigit nyamuk. Warna putih pada kulit seperti ”panu”. Sering menggosok mata, hidung, telinga, sering menarik atau memegang alat kelamin karena gatal. Kotoran telinga berlebihan, sedikit berbau, sakit telinga bila ditekan (otitis eksterna).
SALURAN CERNA : Mudah MUNTAH bila menangis, berlari atau makan banyak. MUAL pagi hari. Sering Buang Air Besar (BAB) 3 kali/hari atau lebih, sulit BAB (obstipasi), kotoran bulat kecil hitam seperti kotoran kambing, keras, sering buang angin, berak di celana. Sering KEMBUNG, sering buang angin dan bau tajam. Sering NYERI PERUT.
GIGI DAN MULUT : Nyeri gigi, gigi berwarna kuning kecoklatan, gigi rusak, gusi mudah bengkak/berdarah. Bibir kering dan mudah berdarah, sering SARIAWAN, lidah putih & berpulau, mulut berbau, air liur berlebihan.
PEMBULUH DARAH Vaskulitis (pembuluh darah kecil pecah) : sering LEBAM KEBIRUAN pada tulang kering kaki atau pipi atas seperti bekas terbentur. Berdebar-debar, mudah pingsan, tekanan darah rendah.
OTOT DAN TULANG : nyeri kaki atau kadang tangan, sering minta dipijat terutama saat malam hari. Kadang nyeri dada
SALURAN KENCING : Sering minta kencing, BED WETTING (semalam ngompol 2-3 kali)
MATA : Mata gatal, timbul bintil di kelopak mata (hordeolum). Kulit hitam di area bawah kelopak mata. memakai kaca mata (silindris) sejak usia 6-12 tahun.
HORMONAL : rambut berlebihan di kaki atau tangan, keputihan, gangguan pertumbuhan tinggi badan.
Kepala,telapak kaki/tangan sering teraba hangat. Berkeringat berlebihan meski dingin (malam/ac). Keringat berbau.
FATIQUE : mudah lelah, sering minta gendong

GANGGUAN PERILAKU YANG SERING MENYERTAI PENDERITA ALERGI DAN HIPERSENSITIFITAS MAKANAN PADA ANAK
SUSUNAN SARAF PUSAT : sakit kepala, MIGRAIN, TICS (gerakan mata sering berkedip), , KEJANG NONSPESIFIK (kejang tanpa demam & EEG normal).
GERAKAN MOTORIK BERLEBIHAN Mata bayi sering melihat ke atas. Tangan dan kaki bergerak terus tidak bisa dibedong/diselimuti. Senang posisi berdiri bila digendong, sering minta turun atau sering menggerakkan kepala ke belakang, membentur benturkan kepala. Sering bergulung-gulung di kasur, menjatuhkan badan di kasur (“smackdown”}. ”Tomboy” pada anak perempuan : main bola, memanjat dll.
AGRESIF MENINGKAT sering memukul kepala sendiri, orang lain. Sering menggigit, menjilat, mencubit, menjambak (spt “gemes”)
GANGGUAN KONSENTRASI: cepat bosan sesuatu aktifitas kecuali menonton televisi,main game, baca komik, belajar. Mengerjakan sesuatu tidak bisa lama, tidak teliti, sering kehilangan barang, tidak mau antri, pelupa, suka “bengong”, TAPI ANAK TAMPAK CERDAS
EMOSI TINGGI (mudah marah, sering berteriak /mengamuk/tantrum), keras kepala, negatifisme
GANGGUAN KESEIMBANGAN KOORDINASI DAN MOTORIK : Terlambat bolak-balik, duduk, merangkak dan berjalan. Jalan terburu-buru, mudah terjatuh/ menabrak, duduk leter ”W”.
GANGGUAN SENSORIS : sensitif terhadap suara (frekuensi tinggi) , cahaya (mudah silau), perabaan telapak kaki dan tangan sensitif (jalan jinjit, flat foot, mudah geli, mudah jijik, tidak suka memegang bulu, boneka dan bianatang berbulu)
GANGGUAN ORAL MOTOR : TERLAMBAT BICARA, bicara terburu-buru, cadel, gagap. GANGGUAN MENELAN DAN MENGUNYAH, tidak bisa makan makanan berserat (daging sapi, sayur, nasi) Disertai keterlambatan pertumbuhan gigi.
IMPULSIF : banyak bicara,tertawa berlebihan, sering memotong pembicaraan orang lain
AUTIS dan ADHD (Alergi dan hipersensititas makanan bukan penyebab Autis atau ADHD tetapi hanya memperberat gejalanya)
KOMPLIKASI SERING MENYERTAI ALERGI DAN HIPERSENSITIFITAS MAKANAN PADA ANAK
Daya tahan menurun sering sakit demam, batuk, pilek setiap bulan bahkan sebulan 2 kali. (normal sakit seharusnya 2-3 bulan sekali)
Karena sering sakit berakibat Tonsilitis kronis (AMANDEL MEMBESAR) hindari operasi amandel yang tidak perlu atau mengalami Infeksi Telinga
Waspadai dan hindari efek samping PEMAKAIAN OBAT TERLALU SERING. Mudah mengalami INFEKSI SALURAN KENCING. Kulit di sekitar kelamin
sering kemerahan SERING TERJADI OVERDIAGNOSIS TBC (MINUM OBAT JANGKA
PANJANG PADAHAL BELUM TENTU MENDERITA TBC / ”FLEK ”)

KARENA GEJALA ALERGI MIRIP PENYAKIT TBC. BATUK LAMA BUKAN GEJALA TBC PADA ANAK BILA DIAGNOSIS TBC MERAGUKAN SEBAIKNYA ”SECOND OPINION” DENGAN DOKTER LAINNYA
MAKAN BERLEBIHAN KEGEMUKAN atau OBESITAS INFEKSI JAMUR (HIPERSENSITIF CANDIDIASIS) di lidah, selangkangan, di
leher, perut atau dada, KEPUTIHAN
Bila tanda dan gejala Gastrooesepageal Refluks (GER) atau Sering Muntah pada anak tersebut terjadi pada anak anda dan disertai salah satu gangguan saluran cerna serta beberapa tanda, gejala atau komplikasi alergi dan hipersensitifitas makanan tersebut maka sangat mungkin Gastrooesepageal Refluks (GER) atau Sering Muntah pada anak disebabkan karena alergi atau hipersenitifitas makanan. Penyebab lain yang memperberat Gastrooesepageal Refluks (GER) atau Sering Muntah Pada Anak adalah saat anak terkena infeksi seperti demam, batuk, pilek, diare atau muntah dan infeksi lainnya Memastikan Diagnosis
Diagnosis Gastrooesepageal Refluks (GER) atau Sering Muntah Pada Anak yang disebabkan alergi atau hipersensitif makanan dibuat bukan dengan tes alergi tetapi berdasarkan diagnosis klinis, yaitu anamnesa (mengetahui riwayat penyakit penderita) dan pemeriksaan yang cermat tentang riwayat keluarga, riwayat pemberian makanan, tanda dan gejala alergi makanan sejak bayi dan dengan eliminasi dan provokasi.
Untuk memastikan makanan penyebab alergi dan hipersensitifitas makanan harus menggunakan Provokasi makanan secara buta (Double Blind Placebo Control Food Chalenge = DBPCFC). DBPCFC adalah gold standard atau baku emas untuk mencari penyebab secara pasti alergi makanan. Cara DBPCFC tersebut sangat rumit dan membutuhkan waktu, tidak praktis dan biaya yang tidak sedikit.
Beberapa pusat layanan alergi anak melakukan modifikasi terhadap cara itu. Children Allergy clinic Jakarta melakukan modifikasi dengan cara yang lebih sederhana, murah dan cukup efektif. Modifikasi DBPCFC tersebut dengan melakukan “Eliminasi Provokasi Makanan Terbuka Sederhana”. Bila setelah dilakukan eliminasi beberapa penyebab alergi makanan selama 3 minggu didapatkan perbaikan dalam gangguan muntah tersebut, maka dapat dipastikan penyebabnya adalah alergi makanan.
Pemeriksaan standar yang dipakai oleh para ahli alergi untuk mengetahui penyebab alergi adalah dengan tes kulit. Tes kulit ini bisa terdari tes gores, tes tusuk atau tes suntik. PEMERIKSAAN INI HANYA MEMASTIKAN ADANYA ALERGI ATAU TIDAK, BUKAN UNTUK MEMASTIKAN PENYEBAB ALERGI. Pemeriksaan ini mempunyai sensitifitas yang cukup baik, tetapi sayangnya spesifitasnya rendah. Sehingga seringkali terdapat false negatif, artinya hasil negatif belum tentu bukan penyebab alergi. Karena hal inilah maka sebaiknya tidak membolehkan makan makanan penyebab alergi hanya berdasarkan tes kulit ini.

Dalam waktu terakhir ini sering dipakai alat diagnosis yang masih sangat kontroversial atau ”unproven diagnosis”. Terdapat berbagai pemeriksaan dan tes untuk mengetahui penyebab alergi dengan akurasi yang sangat bervariasi. Secara ilmiah pemeriksaan ini masih tidak terbukti baik sebagai alat diagnosis. Pada umumnya pemeriksaan tersebut mempunyai spesifitas dan sensitifitas yang sangat rendah. Bahkan beberapa organisasi profesi alergi dunia tidak merekomendasikan penggunaan alat tersebut. Yang menjadi perhatian oraganisasi profesi tersebut bukan hanya karena masalah mahalnya harga alat diagnostik tersebut tetapi ternyata juga sering menyesatkan penderita alergi yang sering memperberat permasalahan alergi yang ada
Namun pemeriksaan ini masih banyak dipakai oleh praktisi kesehatan atau dokter. Di bidang kedokteran pemeriksaan tersebut belum terbukti secara klinis sebagai alat diagnosis karena sensitifitas dan spesifitasnya tidak terlalu baik. Beberapa pemeriksaan diagnosis yang kontroversial tersebut adalah Applied Kinesiology, VEGA Testing (Electrodermal Test, BIORESONANSI), Hair Analysis Testing in Allergy, Auriculo-cardiac reflex, Provocation-Neutralisation Tests, Nampudripad’s Allergy Elimination Technique (NAET), Beware of anecdotal and unsubstantiated allergy tests.
PENATALAKSANAAN
Penanganan Gastrooesepageal Refluks (GER) atau Sering Muntah Pada Anak karena alergi dan hipersensitifitas makanan pada anak haruslah dilakukan secara benar, paripurna dan berkesinambungan. Pemberian obat terus menerus bukanlah jalan terbaik dalam penanganan gangguan tersebut tetapi yang paling ideal adalah menghindari penyebab yang bisa menimbulkan keluhan alergi tersebut.
Penghindaran makanan penyebab alergi pada anak harus dicermati secara benar, karena beresiko untuk terjadi gangguan gizi. Sehingga orang tua penderita harus diberitahu tentang makanan pengganti yang tak kalah kandungan gizinya dibandingklan dengan makanan penyebab alergi. Penghindaran terhadap susu sapi dapat diganti dengan susu soya, formula hidrolisat kasein atau hidrolisat whey., meskipun anak alergi terhadap susu sapi 30% diantaranya alergi terhadap susu soya. Sayur dapat dipakai sebagai pengganti buah. Tahu, tempe, daging sapi atau daging kambing dapat dipakai sebagai pengganti telur, ayam atau ikan. Pemberian makanan jadi atau di rumah makan harus dibiasakan mengetahui kandungan isi makanan atau membaca label makanan.
Obat-obatan simtomatis, anti histamine (AH1 dan AH2), ketotifen, ketotofen, kortikosteroid, serta inhibitor sintesaseprostaglandin hanya dapat mengurangi gejala sementara, tetapi umumnya mempunyai efisiensi rendah. Sedangkan penggunaan imunoterapi dan natrium kromogilat peroral masih menjadi kontroversi hingga sekarang.
Obat
Pengobatan Gastrooesepageal Refluks (GER) atau Sering Muntah Pada Anak karena alergi dan hipersensitifitas makanan yang baik adalah dengan

menanggulangi penyebabnya. Bila gangguan sulit makan yang dialami disebabkan karena gangguan alergi dan hipersensitifitas makanan, penanganan terbaik adalah menunda atau menghindari makanan sebagai penyebab tersebut.
Konsumsi obat-obatan saluran cerna atau penahan muntah, terapi tradisional ataupun beberapa cara dan strategi untuk menangani Gastrooesepageal Refluks (GER) atau Sering Muntah pada anak tidak akan berhasil selama penyebab utama alergi dan hipersensitifitas makanan tidak diperbaiki.
What is GERD?
Gastroesophageal reflux disease (GERD) is a more serious form of gastroesophageal reflux (GER), which is common. GER occurs when the lower esophageal sphincter (LES) opens spontaneously, for varying periods of time, or does not close properly and stomach contents rise up into the esophagus. GER is also called acid reflux or acid regurgitation, because digestive juices—called acids—rise up with the food. The esophagus is the tube that carries food from the mouth to the stomach. The LES is a ring of muscle at the bottom of the esophagus that acts like a valve between the esophagus and stomach.
When acid reflux occurs, food or fluid can be tasted in the back of the mouth. When refluxed stomach acid touches the lining of the esophagus it may cause a burning sensation in the chest or throat called heartburn or acid indigestion. Occasional GER is common and does not necessarily mean one has GERD. Persistent reflux that occurs more than twice a week is considered GERD, and it can eventually lead to more serious health problems. People of all ages can have GERD.
[Top]
What are the symptoms of GERD?
The main symptom of GERD in adults is frequent heartburn, also called acid indigestion—burning-type pain in the lower part of the mid-chest, behind the breast bone, and in the mid-abdomen. Most children under 12 years with GERD, and some adults, have GERD without heartburn. Instead, they may experience a dry cough, asthma symptoms, or trouble swallowing.
[Top]
What causes GERD?
The reason some people develop GERD is still unclear. However, research shows that in people with GERD, the LES relaxes while the rest of the esophagus is working. Anatomical abnormalities such as a hiatal hernia may also contribute to GERD. A hiatal hernia occurs when the upper part of the stomach and the LES move above the diaphragm, the muscle wall that separates the stomach from the chest. Normally, the diaphragm helps the LES keep acid from rising up into the esophagus. When a hiatal hernia is present, acid reflux can occur more easily. A hiatal hernia can occur in people of

any age and is most often a normal finding in otherwise healthy people over age 50. Most of the time, a hiatal hernia produces no symptoms.
Other factors that may contribute to GERD include
obesity pregnancy smoking
Common foods that can worsen reflux symptoms include
citrus fruits chocolate drinks with caffeine or alcohol fatty and fried foods garlic and onions mint flavorings spicy foods tomato-based foods, like spaghetti sauce, salsa, chili, and pizza
[Top]
What is GERD in children?
Distinguishing between normal, physiologic reflux and GERD in children is important. Most infants with GER are happy and healthy even if they frequently spit up or vomit, and babies usually outgrow GER by their first birthday. Reflux that continues past 1 year of age may be GERD. Studies show GERD is common and may be overlooked in infants and children. For example, GERD can present as repeated regurgitation, nausea, heartburn, coughing, laryngitis, or respiratory problems like wheezing, asthma, or pneumonia. Infants and young children may demonstrate irritability or arching of the back, often during or immediately after feedings. Infants with GERD may refuse to feed and experience poor growth.
Talk with your child’s health care provider if reflux-related symptoms occur regularly and cause your child discomfort. Your health care provider may recommend simple strategies for avoiding reflux, such as burping the infant several times during feeding or keeping the infant in an upright position for 30 minutes after feeding. If your child is older, your health care provider may recommend that your child eat small, frequent meals and avoid the following foods:
sodas that contain caffeine chocolate peppermint spicy foods acidic foods like oranges, tomatoes, and pizza

fried and fatty foods
Avoiding food 2 to 3 hours before bed may also help. Your health care provider may recommend raising the head of your child’s bed with wood blocks secured under the bedposts. Just using extra pillows will not help. If these changes do not work, your health care provider may prescribe medicine for your child. In rare cases, a child may need surgery. For information about GER in infants, children, and adolescents, see the Gastroesophageal Reflux in Infants and Gastroesophageal Reflux in Children and Adolescents fact sheets from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
[Top]
How is GERD treated?
See your health care provider if you have had symptoms of GERD and have been using antacids or other over-the-counter reflux medications for more than 2 weeks. Your health care provider may refer you to a gastroenterologist, a doctor who treats diseases of the stomach and intestines. Depending on the severity of your GERD, treatment may involve one or more of the following lifestyle changes, medications, or surgery.
Lifestyle Changes If you smoke, stop. Avoid foods and beverages that worsen symptoms. Lose weight if needed. Eat small, frequent meals. Wear loose-fitting clothes. Avoid lying down for 3 hours after a meal. Raise the head of your bed 6 to 8 inches by securing wood blocks under the
bedposts. Just using extra pillows will not help.
Medications
Your health care provider may recommend over-the-counter antacids or medications that stop acid production or help the muscles that empty your stomach. You can buy many of these medications without a prescription. However, see your health care provider before starting or adding a medication.
Antacids, such as Alka-Seltzer, Maalox, Mylanta, Rolaids, and Riopan, are usually the first drugs recommended to relieve heartburn and other mild GERD symptoms. Many brands on the market use different combinations of three basic salts—magnesium, calcium, and aluminum—with hydroxide or bicarbonate ions to neutralize the acid in your stomach. Antacids, however, can have side effects. Magnesium salt can lead to diarrhea, and aluminum salt may cause constipation. Aluminum and magnesium salts are often combined in a single product to balance these effects.

Calcium carbonate antacids, such as Tums, Titralac, and Alka-2, can also be a supplemental source of calcium. They can cause constipation as well.
Foaming agents, such as Gaviscon, work by covering your stomach contents with foam to prevent reflux.
H2 blockers, such as cimetidine (Tagamet HB), famotidine (Pepcid AC), nizatidine (Axid AR), and ranitidine (Zantac 75), decrease acid production. They are available in prescription strength and over-the-counter strength. These drugs provide short-term relief and are effective for about half of those who have GERD symptoms.
Proton pump inhibitors include omeprazole (Prilosec, Zegerid), lansoprazole (Prevacid), pantoprazole (Protonix), rabeprazole (Aciphex), and esomeprazole (Nexium), which are available by prescription. Prilosec is also available in over-the-counter strength. Proton pump inhibitors are more effective than H2 blockers and can relieve symptoms and heal the esophageal lining in almost everyone who has GERD.
Prokinetics help strengthen the LES and make the stomach empty faster. This group includes bethanechol (Urecholine) and metoclopramide (Reglan). Metoclopramide also improves muscle action in the digestive tract. Prokinetics have frequent side effects that limit their usefulness—fatigue, sleepiness, depression, anxiety, and problems with physical movement.
Because drugs work in different ways, combinations of medications may help control symptoms. People who get heartburn after eating may take both antacids and H2 blockers. The antacids work first to neutralize the acid in the stomach, and then the H2 blockers act on acid production. By the time the antacid stops working, the H2 blocker will have stopped acid production. Your health care provider is the best source of information about how to use medications for GERD.
[Top]
What if GERD symptoms persist?
If your symptoms do not improve with lifestyle changes or medications, you may need additional tests.
Barium swallow radiograph uses x rays to help spot abnormalities such as a hiatal hernia and other structural or anatomical problems of the esophagus. With this test, you drink a solution and then x rays are taken. The test will not detect mild irritation, although strictures—narrowing of the esophagus—and ulcers can be observed.
Upper endoscopy is more accurate than a barium swallow radiograph and may be performed in a hospital or a doctor’s office. The doctor may spray your throat to numb it and then, after lightly sedating you, will slide a thin, flexible plastic tube with a light and lens on the end called an endoscope down your throat. Acting as a

tiny camera, the endoscope allows the doctor to see the surface of the esophagus and search for abnormalities. If you have had moderate to severe symptoms and this procedure reveals injury to the esophagus, usually no other tests are needed to confirm GERD.
The doctor also may perform a biopsy. Tiny tweezers, called forceps, are passed through the endoscope and allow the doctor to remove small pieces of tissue from your esophagus. The tissue is then viewed with a microscope to look for damage caused by acid reflux and to rule out other problems if infection or abnormal growths are not found.
pH monitoring examination involves the doctor either inserting a small tube into the esophagus or clipping a tiny device to the esophagus that will stay there for 24 to 48 hours. While you go about your normal activities, the device measures when and how much acid comes up into your esophagus. This test can be useful if combined with a carefully completed diary—recording when, what, and amounts the person eats—which allows the doctor to see correlations between symptoms and reflux episodes. The procedure is sometimes helpful in detecting whether respiratory symptoms, including wheezing and coughing, are triggered by reflux.
A completely accurate diagnostic test for GERD does not exist, and tests have not consistently shown that acid exposure to the lower esophagus directly correlates with damage to the lining.
Surgery
Surgery is an option when medicine and lifestyle changes do not help to manage GERD symptoms. Surgery may also be a reasonable alternative to a lifetime of drugs and discomfort.
Fundoplication is the standard surgical treatment for GERD. Usually a specific type of this procedure, called Nissen fundoplication, is performed. During the Nissen fundoplication, the upper part of the stomach is wrapped around the LES to strengthen the sphincter, prevent acid reflux, and repair a hiatal hernia.
The Nissen fundoplication may be performed using a laparoscope, an instrument that is inserted through tiny incisions in the abdomen. The doctor then uses small instruments that hold a camera to look at the abdomen and pelvis. When performed by experienced surgeons, laparoscopic fundoplication is safe and effective in people of all ages, including infants. The procedure is reported to have the same results as the standard fundoplication, and people can leave the hospital in 1 to 3 days and return to work in 2 to 3 weeks.
Endoscopic techniques used to treat chronic heartburn include the Bard EndoCinch system, NDO Plicator, and the Stretta system. These techniques require the use of an endoscope to perform the anti-reflux operation. The EndoCinch and NDO Plicator systems involve putting stitches in the LES to create pleats that help strengthen the

muscle. The Stretta system uses electrodes to create tiny burns on the LES. When the burns heal, the scar tissue helps toughen the muscle. The longterm effects of these three procedures are unknown.
[Top]
What are the long-term complications of GERD?
Chronic GERD that is untreated can cause serious complications. Inflammation of the esophagus from refluxed stomach acid can damage the lining and cause bleeding or ulcers—also called esophagitis. Scars from tissue damage can lead to strictures—narrowing of the esophagus—that make swallowing difficult. Some people develop Barrett’s esophagus, in which cells in the esophageal lining take on an abnormal shape and color. Over time, the cells can lead to esophageal cancer, which is often fatal. Persons with GERD and its complications should be monitored closely by a physician.
Studies have shown that GERD may worsen or contribute to asthma, chronic cough, and pulmonary fibrosis.
For information about Barrett’s esophagus, see the Barrett’s Esophagus fact sheet from the NIDDK.
[Top]
Points to Remember
Frequent heartburn, also called acid indigestion, is the most common symptom of GERD in adults. Anyone experiencing heartburn twice a week or more may have GERD.
You can have GERD without having heartburn. Your symptoms could include a dry cough, asthma symptoms, or trouble swallowing.
If you have been using antacids for more than 2 weeks, it is time to see your health care provider. Most doctors can treat GERD. Your health care provider may refer you to a gastroenterologist, a doctor who treats diseases of the stomach and intestines.
Health care providers usually recommend lifestyle and dietary changes to relieve symptoms of GERD. Many people with GERD also need medication. Surgery may be considered as a treatment option.
Most infants with GER are healthy even though they may frequently spit up or vomit. Most infants outgrow GER by their first birthday. Reflux that continues past 1 year of age may be GERD.

The persistence of GER along with other symptoms—arching and irritability in infants, or abdominal and chest pain in older children—is GERD. GERD is the outcome of frequent and persistent GER in infants and children and may cause repeated vomiting, coughing, and respiratory problems.
[Top]
Hope through Research
The reasons certain people develop GERD and others do not remain unknown. Several factors may be involved, and research is under way to explore risk factors for developing GERD and the role of GERD in other conditions such as asthma and laryngitis.
PDF Version * (136 KB)
Also see:Gastroesophageal Reflux in Children and Adolescents
Home : Digestive Diseases A-Z List of Topics and Titles : Gastroesophageal Reflux in Infants

Gastroesophageal Reflux in Infants
On this page:
What is gastroesophageal reflux (GER)? What are the symptoms of GER? How is GER diagnosed? What is the treatment for GER? Points to Remember Hope through Research For More Information
What is gastroesophageal reflux (GER)?
Gastroesophageal reflux (GER) occurs when stomach contents reflux, or back up, into the esophagus during or after a meal. The esophagus is the tube that connects the mouth to the stomach. A ring of muscle at the bottom of the esophagus opens and closes to allow food to enter the stomach. This ring of muscle is called the lower esophageal sphincter (LES). The LES normally opens to release gas after meals. With infants, when the LES opens, stomach contents often reflux into the esophagus and out the mouth, resulting in regurgitation, or spitting up, and vomiting. GER can also occur when babies cough, cry, or strain.
[Top]
What are the symptoms of GER?
GER is common in healthy infants. More than half of all babies experience reflux in the first 3 months of life, but most stop spitting up between the ages of 12 to 24 months. Only a small number of infants have severe symptoms. An infant with GER may experience
spitting up vomiting coughing irritability poor feeding blood in the stools
In a small number of babies, GER results in symptoms that cause concern. These symptoms include
poor growth due to an inability to hold down enough food irritability or refusing to feed due to pain blood loss from acid burning the esophagus

breathing problems
These problems can be caused by disorders other than GER. Your health care provider will need to determine whether GER is the cause of your child’s symptoms.
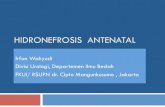
Digestive system noting the mouth, esophagus, lower esophageal sphincter (LES), stomach, and small intestine.
[Top]
How is GER diagnosed?
An infant who is consistently spitting up or vomiting may have GER. The doctor or nurse will talk with you about your child’s symptoms and examine your child. Tests may be ordered to help determine whether your child’s symptoms are related to GER. Sometimes treatment is started without tests. If the infant is healthy, content, and growing well, often no tests or treatment are needed.
[Top]
What is the treatment for GER?
Call your child’s health care provider right away if any of the following occur:
vomiting large amounts or persistent projectile (forceful) vomiting, particularly in infants younger than 2 months old
vomiting fluid that is green or yellow or that looks like coffee grounds or blood

difficulty breathing after vomiting or spitting up refusing food that seems to result in weight loss or poor weight gain excessive crying and irritability
The treatment for reflux depends on an infant’s symptoms and age. Some babies may not need treatment because GER often resolves by itself. Healthy babies may only need their feedings thickened with cereal and to be kept upright after eating. Overfeeding can aggravate reflux, so your health care provider may suggest different ways of handling feedings. For example, smaller quantities with more frequent feedings can help decrease the chances of regurgitation. If a food allergy is suspected, you may be asked to change the baby’s formula. Breastfeeding mothers may be asked to change their own diets for 1 to 2 weeks. If a child is not growing properly, higher-calorie food or tube feeding may be recommended.
When an infant is uncomfortable, has difficulty sleeping or eating, or does not grow, your health care provider may suggest a trial of medication to decrease the amount of acid in the stomach. Any potential complications related to the medication will be explained. However, most infants don’t need medication and outgrow reflux by 1 or 2 years of age.
*If medication is needed, treatment will often start with a class of medications called H2-blockers, also called H2-receptor agonists. These drugs help keep acid from backing up into the esophagus. H2-blockers are often used to treat children with GER because they come in liquid form. H2-blockers include
cimetidine (Tagamet) ranitidine (Zantac) famotidine (Pepcid) nizatidine (Axid)
A second class of medications often used to reduce stomach acid is proton-pump inhibitors (PPIs), which block the production of stomach acid. PPIs include
esomeprazole (Nexium) omeprazole (Prilosec) lansoprazole (Prevacid) rabeprazole (Aciphex) pantoprazole (Protonix)
* The authors of this fact sheet do not specifically endorse the use of drugs for children that have not been tested in children (“off label” use). Such a determination can only be made under the recommendation of the treating health care provider.
Specific Instructions for Infants with GER
If you feed your baby with a bottle, add up to 1 tablespoon of rice cereal to 2 ounces of infant milk. You can add cereal to expressed milk if you are

breastfeeding. If the mixture is too thick for your baby you can change the nipple size or cut a little “x” in the nipple.
Burp your baby after he’s consumed 1 or 2 ounces of formula. For breast-fed infants, burp after feeding on each side.
Do not overfeed. Talk with your infant’s doctor or nurse about the amount of formula or breast milk that your baby is consuming.
When possible, hold your infant upright in your arms for 30 minutes after feedings.
Infants with GER should usually sleep on their backs, as is suggested for all infants. Rarely, a physician may suggest alternative sleep positions.
[Top]
Points to Remember
GER occurs when stomach contents back up into the esophagus. GER is common in infants but most grow out of it. In infants, GER may cause spitting up, vomiting, coughing, poor feeding, or
blood in the stools. Treatment depends on the infant’s symptoms and age and may include changes in
eating and sleeping habits. Medication may also be an option. Only rarely and in severe cases is surgery required.
[Top]
Hope through Research
The National Institute of Diabetes and Digestive and Kidney Diseases, through its Division of Digestive Diseases and Nutrition, supports basic and clinical research into gastrointestinal diseases. Researchers are studying the risk factors for developing GER and what causes the LES to open, with the aim of improving future treatment for GER. They are also studying the efficacy and safety of drug therapy for the treatment of GER in children and investigating the effectiveness of medications compared with surgery.
Page 1 Page 1GASTROESOPHAGEAL REFLUX (GER) IN CHILDREN Gastroesophageal reflux (GER) PADA ANAK Gastroesophageal Reflux (GER) occurs when stomach contents spontaneously regurgitate Gastroesophageal Reflux (GER) terjadi ketika isi perut secara spontan memuntahkan into the esophagus. ke kerongkongan. All children and adults will experience episodes of reflux from time Semua anak dan orang dewasa akan mengalami episode refluks dari waktu

to time. ke waktu. While adults may recognize it as heartburn, infants will often spit-up or vomit. Sementara orang dewasa bisa mengenalinya sebagai mulas, bayi akan sering meludah-up atau muntah. Though it is not uncommon for infants to spit-up, when it becomes a chronic occurrence, Meskipun tidak jarang untuk bayi untuk meludah-up, ketika menjadi kejadian kronis, parents often become concerned. orang tua sering menjadi prihatin. It is often noted that there is no true, definable cause of GER in children. Hal ini sering dicatat bahwa tidak ada didefinisikan, penyebab sebenarnya dari APK pada anak-anak. Some speculate Beberapa berspekulasi that it may be due to immaturity of the brain as in premature babies, food allergies, or bahwa hal itu mungkin karena ketidakmatangan otak seperti pada bayi prematur, alergi makanan, atau slow digestion. memperlambat pencernaan. Regardless of the cause, if your infant or toddler is exhibiting the Terlepas dari penyebabnya, jika bayi atau anak adalah menunjukkan yang following symptoms, it may be an indication that he/she is experiencing GER: gejala berikut, mungkin menjadi indikasi bahwa dia mengalami APK: irritability; difficulty sleeping; stomach pain; feeding problems such as choking, lekas marah, sulit tidur, sakit perut, makan masalah seperti tersedak, gagging, regurgitation/vomiting, and feeding refusal; respiratory difficulty such as tersedak, regurgitasi / muntah, dan penolakan makan; kesulitan pernapasan seperti chronic cough or recurrent pneumonia; growth failure; unusual posturing; and a batuk kronis atau pneumonia berulang, pertumbuhan kegagalan; sikap yang tidak biasa, dan hoarse or raspy voice . serak atau suara serak. For children with developmental disabilities, the symptoms are Untuk anak-anak cacat pembangunan, gejala yang often more severe and/or more persistent. sering lebih parah dan / atau lebih persisten. Diagnosis of GER in infants and toddlers is often achieved by taking a medical history, Diagnosis APK pada bayi dan balita sering dicapai dengan mengambil riwayat medis, observation, and a physical examination. observasi, dan pemeriksaan fisik. In some instances, a procedure called a barium Dalam beberapa kasus, prosedur yang disebut barium sebuah swallow may be warranted. menelan dapat dibenarkan. During this procedure, the infant or child is fed barium Selama prosedur ini, bayi atau anak makan barium which may be viewed using an x-ray camera. yang dapat dilihat menggunakan kamera x-ray. The barium is then observed as it travels barium tersebut kemudian diamati karena perjalanan down the esophagus into the stomach. menuruni kerongkongan ke perut. The radiologist may then observe if reflux occurs. ahli radiologi kemudian boleh mengamati jika refluks terjadi. Once GER has been diagnosed, there are several treatment options. Setelah APK telah didiagnosis, ada beberapa pilihan pengobatan. They include Mereka termasuk positioning, dietary changes, changes in feeding schedules, medications, and surgery. posisi, perubahan pola makan, perubahan jadwal makan, obat-obatan, dan pembedahan.

Positioning : As many adults with GER can tell you, lying down after eating often leads Positioning: Seperti banyak orang dewasa dengan APK dapat memberitahu Anda, berbaring setelah makan sering menyebabkan to an increase in reflux. peningkatan refluks. This too applies to infants and toddlers. Hal ini juga berlaku untuk bayi dan balita. By keeping your child Dengan menjaga anak Anda in an upright position following feeds, you may reduce the occurrence of reflux. dalam posisi tegak feed berikut, Anda dapat mengurangi terjadinya refluks. Dietary changes : Some infants experience less GER when their formula is changed to a Perubahan diet: Beberapa bayi mengalami APK kurang bila rumus mereka berubah ke hypoallergenic or predigested formula such as Nutramagin, Pregestimil, and Alimentum. hipoalergenik atau formula yg telah dicernakan sebelumnya seperti Nutramagin, Pregestimil, dan Alimentum. For older children GER trigger foods should also be avoided such as orange juice, Untuk anak yang lebih tua APK makanan pemicu juga harus dihindari seperti jus jeruk, lemonade, mashed potatoes, French fries, chicken nuggets, macaroni and cheese, limun, kentang pure, kentang goreng, nugget ayam, makaroni dan keju, spaghetti and sauce, chocolate, doughnuts, and potato chips to name a few. spaghetti dan saus, coklat, donat, dan keripik kentang untuk beberapa nama. Change in feeing schedules : Small frequent meals are recommended throughout the day Perubahan feeing jadwal: makan sering Kecil dianjurkan sepanjang hari and eating two hours before bedtime should be avoided. dan makan dua jam sebelum tidur harus dihindari. Medications : There are various types and brands of medications used to reduce GER. Obat-obatan: Ada berbagai jenis dan merek obat yang digunakan untuk mengurangi APK. Acid reducers, such as Zantac, Pepcid, Tagamet, and Axid, suppress the amount of acid pengurang Acid, seperti Zantac, Pepcid, Tagamet, dan Axid, menekan jumlah asam in the stomach. dalam perut. Acid blockers, such as Prilosec, Prevacid, and Nexium, turn off the acid Acid blocker, seperti Prilosec, Prevacid, dan Nexium, matikan asam pumps in the stomach. Please note that you should discuss medications for GER with pompa di perut dengan. Harap dicatat bahwa anda harus membahas obat untuk APK your doctor prior to administering them to your child. dokter Anda sebelum pemberian mereka kepada anak Anda.
Page 2 Page 2For infants and toddlers, repeated occurrences of reflux may lead to negative attitudes Untuk bayi dan balita, kejadian berulang-ulang refluks dapat mengakibatkan sikap negatif towards food and eating. terhadap makanan dan makan. For those children who have feeding aversions and are receiving Bagi anak-anak yang makan keengganan dan menerima medication for GER, it is important that medication is given continuously. obat untuk APK, penting bahwa obat diberikan terus menerus. Many times, Banyak kali,

parents are prone to discontinuing medications once their child's symptoms subside. orang tua rentan terhadap obat menghentikan gejala itu mereda setelah anak mereka. In Dalam doing so the child's symptoms may return and feeding progress hindered. sehingga gejala-gejala mungkin anak kembali dan makan kemajuan melakukan terhalang. Surgery : In instances where behavioral changes and/or medication have been unable to Bedah: Dalam kasus di mana perubahan perilaku dan / atau pengobatan tidak mampu control the GER, a procedure called a Fundoplication may be done. APK kontrol, prosedur yang disebut fundoplication dapat dilakukan. During the Selama Fundoplication, the upper part of the stomach is wrapped around the esophagus. Fundoplication, bagian atas perut melilit kerongkongan. Food Makanan continues to pass to the stomach however reflux is prevented. terus berlalu ke perut namun refluks dicegah. If your child has developed feeding aversions due to GER contact a speech-language Jika anak Anda telah mengembangkan keengganan makan karena kontak APK pidato bahasa pathologist. ahli patologi. A speech-language pathologist can provide feeding therapy for infants and A-bahasa patolog pidato dapat memberikan terapi makanan untuk bayi dan toddlers and provide strategies for parents. balita dan memberikan strategi untuk orang tua. Center for Speech and Language Pathology Pusat dan Patologi Bahasa Pidato
http://www.bayusatria.web.id/2010/11/terapi-cairan-intravena-kristaloid-pada.html