Farm TX Khusus,2009
60
Farmakoterapi pada Kelompok Khusus Fathiyah Safithri Laboratorium Farmakologi FK-UMM 2009
-
Upload
yasmin-abdullah -
Category
Documents
-
view
392 -
download
0
Transcript of Farm TX Khusus,2009

Farmakoterapi pada Kelompok Khusus
Fathiyah SafithriLaboratorium Farmakologi FK-UMM
2009

Kelompok Khusus ?
• Neonatus dan Pediatri• Ibu menyusui• Ibu hamil• Usia lanjut• Penderita gagal ginjal• Penderita gangguan fungsi hepar

Dosis yg diresepkan (R/)
Dosis yang diminum/diberikan
Faktor FK : A D M E
Konsentrasi obat di tempat kerja
FisiologisPatologisGenetikUsiaInteraksi Faktor FD :
fungsional reseptor
EFEK / RESPON PASIEN
terapi toxic
Kepatuhan pasien
Efek samping

FARMAKOTERAPI FARMAKOTERAPI pada pada
PASIEN PEDIATRI PASIEN PEDIATRI

Pasien Pediatri• Pediatri : semua pasien < 16 th• Ada 6 kelompok umur pediatri :
Premature infants :< 36 mgg kehamilanFull-term infants :36-40 mgg kehamilanNeonates :4 mgg pertama post-natalInfants :5-32 mgg post-natalChildren :1-12 tahunAdolescents :12-16 tahun

Factors Affecting Drug Effects on the Infant
I. Drug AbsorptionII. Drug DistributionIII. Drug MetabolismIV. Drug Excretion

Absorption- Gastric acid secretion commences soon after birth and increases gradually over several hours. In preterm infants it appears slowly. Very acidic at birth with gradual decrease over the first two years. Drugs affected by gastric pH should not be administered orally.
- Gastric emptying is prolonged in the first day of life. Newborn infant: 6-8 hours, Toddlers: 2 hours
- Peristalsis in the neonate is slow. Diarrhea causes decrease absorption in small intestine.

AbsorptionSkin• thin dermis and epidermis• increased tendency to absorb larger amounts of a topical
medication– could result in unwanted systemic effects
• percutan injection absorption >Muscle mass• small muscle mass with poorly developed peripheral circulation• decrease the rate of absorption from IM injections

Drug Absorption in DrugAcetaminophenAmpicillinDiazepamDigoxinPenicillin GPhenobarbitalPhenytoinSulfonamides
the neonate compared to adults.Oral AbsorptionDecreasedIncreasedNormalNormalIncreasedDecreasedDecreasedNormal

Distribution• Dipengaruhi oleh : komposisi cairan tubuh, lemak tubuh,
ikatan protein.• Pd neonatus, 70-75% BB adalah air, pd preterm 85% pd
dewasa 50-60% .• Pd neonatus total body fat adalah 15%, sdg pada preterm
1%, toddlers 23%, preschooler 8-12% • Protein binding of drugs is reduced in the neonate.
Therefore, concentration of free drug in plasma is increased => increased effect or increase toxicity.
• Drugs (e.g. sulfonamide antibiotics) that displace bilirubin from albumin may cause kernicterus. Conversely, bilirubin may also displace protein-bound drugs (e.g. phenytoin).

Distribution
Blood-Brain Barrier • not mature until approximately 2 years of age
• drugs more easily distributed to the brain = toxic effects

Drug Metabolism• Metabolism of most drugs occurs in the liver. • The metabolizing activity of cytochrome P450-dependent
mixed-function oxidases is reduced in neonates (50-70% of adult values).
• Glucoronide formation doesn’t occur until the 3th -4rd years of life. Thus, in the neonate, drugs have slow clearance rates and prolonged half-lives.
• If the mother was taking phenobarbital, neonatal liver enzymes could have been induced. The ability of the neonate to metabolize certain drugs would be greater than expected and the effect could be less.

Drug Excretion• Glomerular filtration is much lower (30-40% of
adult) in neonates for the first few days of life. Within a week glomerular filtration and plasma flow increase by 50% and reach adult values within 6-12 months. Drugs that depend on renal flow are eliminated very slowly in the first few weeks of life (penicilins, aminoglycoside antibiotics, digoxin)
Ampicillin< 7 days old=> 50-100 mg/Kg/d , 2d at 12 hr
intervals.> 7 days old => 100-200 mg/Kg/d, 3d at 8 hr intervals

Drug Excretion
Urine pH• more acidic in infants
– pH remains constant the day and night• older children & adults more basic pH during day
and acidic at night
• results in increased reabsorption of acidic drugs

Penghitungan dosis
Formula Young (berdasar umur)
dosis anak = umur (th) x dosis dws umur+12(th)
Formula Clark (berdasar berat badan)dosis anak = BB (kg) x dosis dws
70 (kg) Berdasar luas permukaan tubuh
dosis anak = luas permk tbh(m2) x dosis dws 1,73(m2)

FARMAKOTERAPI pada FARMAKOTERAPI pada IBU MENYUSUIIBU MENYUSUI

Drug Therapy during Breast Feeding
• Drugs get through breast milk and can effect infant– All drugs can be detected in milk, but concentrations usually
too low to be of concern (breast feeding is usually safe)– Little research done on this aspect because of dangers involved in these
studies• Concentration of drugs differ in milk
– Lipid soluble drugs are in higher concentration• Generally most drugs are in too low a concentration to be harmful to infant
• Things That Can Minimize Risk:– Dose after breast feeding– Take drugs with short ½ life– Take drugs that are not found in breast milk– Avoid drugs known to be hazardous

• ASI : terlibat dalam ekskresi bbrp obat• Obat/bhn kimia yg dikonsumsi ibu dpt mencapai ASI
melalui mekanisme difusi pasif dan diduga akibat ikatan obat dg protein atau dg permukaan globul lemak ASI
• Obat/bhn kimia tsb dapat memberi efek pd bayi atau produksi ASI.
• Target : terapi farmakologik pada ibu efektif dan bayi tidak mendapat efek negatif dari terapi tersebut

Obat yg Mensupresi Obat yg Mensupresi LaktasiLaktasi
• Bromokriptin• Estradiol• Kontrasepsi oral dosis besar• Levodopa• Antidepresan trazodon• Piridoksin dosis tinggi

Prinsip Pemberian Obat untukPrinsip Pemberian Obat untuk Ibu Menyusui Ibu Menyusui
• Perhatikan apakah terapi obat tsb benar2 diperlukan .• Pilih obat yg paling aman utk ibu menyusui (yg tdk
diekskresi lewat ASI, wkt paruh pendek, tdk bahaya utk bayi)
• Jk diperkirakan obat akan berpengaruh pd bayi, perlu dipertimbangkan pengukuran konsentrasi obat dalam darah bayi
• Sedpt mungkin ibu minum obat 30-60 mnt setelah menyusui atau 3-4 jam sblm menyusui berikutnya

Farmakoterapi pada Ibu Hamil

• 1/3 to ½ of pregnant women take at least one prescription drug and most take more– Some used to treat pregnancy side effects
• Nausea• Pre-eclampsia • Constipation
– Some medications used to treat chronic disorders• Hypertension• Diabetes• Epilepsy• Cancer• Infectious Diseases
– Drugs of abuse

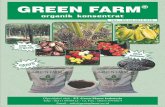
1) Placenta, berfungsi sbg :
membran semipermeable tempat metabolisme obat.
2) Hepar : metabolisme obat
Dua mekanisme yg melindungi janin dari obat yg berada dlm darah ibu

Plasenta
Umbilical arteries
Umbilical vein
Chorionic villus
Placental septum
Endometrial
arteries
and veins
Intervillus space
Chorion
Amnion

Faktor yang Mempengaruhi Transfer Obat
ke Janin
1. Sifat fisikokimia obat
2. Kadar obat yang mencapai fetus
3. Exposure rate.
4. Lama paparan
5. Distribusi jaringan.
6. Tahap perkembangan janin saat terpapar obat.
7. Interaksi dengan obat lain .

Sifat Fisikokimia ObatA. Kelarutan dalam Lemak (lipofilik)• Obat lipofilik menembus plasenta .
kecepatan & obat menembus tgt : BM & konsentrasi dlm darah ibu)
Distribusi tgt aliran darah plasenta .
• Obat non lipofilik cenderung terikat kuat dg protein plasma.
Contoh : obat lipofilik : thiopental (SC) BBL apnea
B. Derajat Ionisasi Obat- Substansi polar / terionisasi sulit melewati
plasenta
contoh : suksinilkolin, tubokurarin

Sifat Fisikokimia Obat
C. Ikatan dg protein.
mis. sulfonamides, barbiturates, phenytoin and local anesthetic agents.
D. Ukuran molekul obat- BM 250-500 mudah - BM 500-1000 sulit- BM >1000 sgt sulit (mis. heparin vs warfarin)- Sebagian besar obat mempunyai BM 100-500
.

Distribusi : Affinitas Obat thd Jaringan Tertentu
TetracyclineWarfarinAminoglycosidesQuinineChlorpromazineDiethylstilbestrol
CorticosteroidsPhenytoinIodidesPropylthiouracil
Teeth
Middle earRetina
Mullerian DuctVaginaAdrenal Gland
Thyroid Gland

Stages of Fetal Development• Sensitivity of fetus to drug is dependent upon developmental stage and when drug is
given in relation to the developmental stage• 3 stages of embryonic development
• Pre-implantation period• Embryogenic period • Fetal period
• Most critical time for any organ is when it is growing and forming its structures. Diff. organs have diff. critical periods, but the time period from day 15 to day 60 of gestation is most critical
- Heart: weeks 3-4
- Ext genitalia: weeks 8-9
- Brain & skeleton: Week 3- end of pregnancy

Stages of Fetal Development• During pre-implantation and embryonic stages the
teratogen acts in an all-or-none response, i.e. , the dose is high enough that the fetus will die, if dose is sublethal fetus will recover
• Gross malformations produced by exposure to teratogens during the embryonic period (1st trimester)
• Exposure during the 2nd and 3rd trimesters usually results in organ dysfunction rather than gross malformations

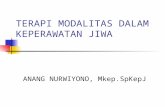
Fetal Development
CNS
Heart
Eyes
Legs
Arms
0 5 15
Teeth
Palate
Ex. genitalia
Ear
Full term

Figure 10-1: Effects of Teratogens at Specific
Stages of Fetal Development
Moore, 1993.

Farmakokinetik Obat selama kehamilan
Absorbsi Awal hamil, sekresi asam lambung 30-40%
absorbsi obat asam lemah , obat basa lemah Gastric emptying Motilitas GIT absorbsi obat yg sukar larut
(digoksin) , absorbsi obat yg dimetab di dind usus (CPZ)

Distribusi Vol plasma & CES (50%) kdr obat dg Vd kecil
(ampicillin) dlm plasma << Albumin serum 20%, glikoprotein 100% (t.u pd
eklampsia) fraksi bebas obat asam (diazepam, fenitoin, as valproat), fraksi bebas obat basa
Body fat Obat lipofilik tersimpan di jar lemak durasi obat (slow release).

Eliminasi Trimest 2&3, progesteron me aktivitas enz metab
hepar kdr obat cpt (fenitoin, carbamazepin, fenobarbital)
Awal hamil, renal blood flow dan GFR 2x eliminasi obat yg eksresi lwt ginjal
Akhir hamil, renal blood flow dan GFR

PENGARUH OBAT PD JANIN
• TOKSIK gangg fisiologik / biokimiawi janin gejala terlihat stl lahir
• TERATOGENIK malformasi anatomik pd pertumbuhan organ janin
• LETAL kematian janin dlm kandungan
TGT SIFAT OBAT & UMUR KEHAMILAN SAAT TERPAPAR

PENGARUH BURUK PD JANIN
Fase Implantasi (<3mgg) kematian embrio / abortus
Fase embrional / organogenesis (4-8 mgg) diferensiasi pertumbuhan malformasi anatomik (teratogenik)- gangg fungsional / metabolik permanen mis. Ca di kemudian hari- letal (IUFD/abortus)- subletal (malformasi pertumb organ, mis fokomelia)
Fase fetal (trim 2&3) gangg fisiologik/biokimiawi gangg pertumbuhanmis. Akhir hamil, Analgetik opioid depresi nfs neonatus

Kategori Obat utk Ibu HamilA :byk dipakai, pengaruh buruk (-)
mis. Parasetamol, Penisilin, Eritromisin, digoksin, bhn hemopoetik (Fe, folat), INH
B :sedikit dipakai, pengaruh buruk (-)B1 : pd hewan kerusakan janin (-).mis simetidin, dipiridamolB2 : peneltian pd hewan blm memadai. Mis ticarsilin, amfoterisin
C :pengaruh buruk (+) reversibel, malformasi (-).mis fenitoin, analgetik opioid, fenobarbiton, valproat, karbamazepin
D / X:pengaruh buruk (+) irreversibel, malformasi (+) mis. Isotreonin, DES

Fetal TherapyTherapy directed to the fetus.Corticosteroids. Stimulate fetal lung maturation
when preterm birth is expected.Phenobarbital. Given during the last trimester, close
to term, induces fetal liver enzymes responsible for the glucoronidation of bilirubin, reducing the incidence of jaundice.
Antiarrhythmic drugs. For the treatment of fetal arrythmias.

Teratogenicity
Teratogen. Bahan yg dpt menyebabkan perkembangan abnormal pada janin.mis. alcohol (FAS), Thalidomide (phocomelia), DES (uterine cancer), valproic acid (spina bifida).

Identification of Teratogens• Few drugs considered to be teratogenic: hard to prove
– Incidence of congenital anomalies is low– Animal test may not be applicable– Prolonged exposure may be necessary– Teratogenic effects may be delayed– Behavioral effects are hard to document– Controlled experiments cannot be done in humans
• To prove a drug is a teratogen:– Drug must cause a characteristic set of malformations– It must act only during a specific window of vulnerability (weeks 4
through 7 of gestation)– Incidence of malformations should increase with increasing dosage
and duration of exposure• Risk of malformation with most teratogens is only ~10%
– Table 10-1 lists proven teratogenic drugs


Teratogenicity
Mekanisme Teratogenik
1) Menimbulkan efek pd jaringan ibu2) Menghambat penyaluran oksigen 3) Perubahan nutrisi selama proses differensiasi.4) Defisiensi

Teratogenicity
1) Efek pd jaringan ibu. Obat memberi efek langsung pd jar. Ibu, sedang efek
sekunder atau efek tdk langsungnya pada janin.mis Cocaine meningkatkan resiko spontaneous abortions,
placenta previa and premature labor; neonatal cerebral infarction, abnormal development and decrease school performance.
2) Menghambat penyaluran oksigen dan nutrisi.Akibatnya pd janin : iskemia t. u otak shg menyebabkan
kerusakan otak berat bahkan kematian

Teratogenicity3) Perubahan penyaluran nutrisi selama differensiasi.
e.g. Vitamin A (Retinol) has important differentiation-directing actions in normal tissues. Excessive amounts may cause birth defects, bone abnormalities and liver damage.
Excess niacin may cause ocular abnormalities.4) Defisiensi.
Alterations of certain factors such as vitamins or minerals may be teratogenic.
e.g. Folic acid causes neural tube defects, supplementation reduces the incidence of spina bifida.

FARMAKOTERAPI pada LANJUT USIA

Mengapa perlu Mengapa perlu dipelajari ?dipelajari ?
Perubahan farmakokinetik pd usia lanjut Perubahan farmakodinamik pd usia lanjut Komorbiditas: interaksi obat-penyakit Polifarmasi: interaksi antar obat-obat Fungsi fisiologis menurun Kepatuhan kurang

Perubahan Perubahan FarmakokinetikFarmakokinetik
• Perubahan fisiologis dan fungsi organ menyebabkan perubahan farmakokinetik
• Perubahan Farmakokinetik meliputi : – Absorbsi– Distribusi – Clearance: eliminasi (ginjal)
metabolisme (hepar)
2004: Cusack, Amer. J of Geriatric Pharmacotherapy 2004: Cusack, Amer. J of Geriatric Pharmacotherapy

Perubahan Farmakokinetik pd Perubahan Farmakokinetik pd LansiaLansia
VOLUME DISTRIBUSI (Vd)Pada lansia, adanya peningkatan proporsi body fat,
penurunan massa otot dan total body water akan mengubah Vd
Body fat ↑ akan meningkatkan Vd obat yang larut lemak shg t½ mkn panjang, mis. Diazepam, thiopental, trazadone
Total body water ↓ akan menurunkan Vd obat yang larut air shg konsentrasi obat dalam plasma meningkat, mis. Ethanol, lithium, aminoglycosides, digoxin

Perubahan Farmakokinetik pd Perubahan Farmakokinetik pd LansiaLansia
IKATAN DG PROTEIN Pada lansia terjadi penurunan kadar albumin akibat
penyakit kronis, mis. Malnutrisi, gangguan fungsi hepar atau ginjal.
Akibatnya bioavailabilitas obat yang mengikat protein akan meningkat karena fraksi obat bebas dalam plasma meningkat.
Contoh obat yg mengikat albumin : ceftriaxone, diazepam, phenytoin, warfarin.

Perubahan Farmakokinetik pd Perubahan Farmakokinetik pd LansiaLansia
ELIMINASI Fungsi ginjal menurunkan eliminasi obat yg
diekskresi oleh ginjal. Pada lansia terjadi penurunan renal clearance (Cl) 35-50%
Cl metabolit aktif yg turun akan meningkatkan efek terapi dan resiko utk menjadi toksik
Perlu dilakukan pengurangan dosis dan atau memperpanjang interval pemberian obat.

Perubahan Farmakokinetik pd Perubahan Farmakokinetik pd LansiaLansia
METABOLISME
Pd lansia 65 th, aliran darah hepar 40-45% dibanding usia 25 th mempengaruhi first pass metabolism
Dan ukuran hepar mengecil Metabolisme oksidatif dg sitokrom P450
clearance obat

Perubahan Farmakodinamik pd Perubahan Farmakodinamik pd LansiaLansia
• respon reseptor obat dan target organ berubah sensitivitas thd obat berubah ES obat .
• Beberapa efek obat mis. Diazepam (sedasi), alkohol, fentanyl,
morphine, dan theophylline• Beberapa efek obat
mis. isoproterenol & beta -blockers

Suboptimal Prescribing
• Polypharmacy• Underuse of Effective Medications• Drug-Drug Interactions• Drug-Disease Interactions• Inadequate Monitoring• Inappropriate Dosing• Inappropriate Duration• Drugs to Avoid

FARMAKOTERAPI pada PENDERITA
GANGGUAN FUNGSI HEPAR & GINJAL

• Clearance (Cl) : kemampuan tubuh utk membersihkan darah dari obat per satuan waktu Cl hepar : organ metabolisme utama Cl ginjal : organ ekskresi utama Cl organ2 lainEliminasi utama hepar Cl (tubuh total) = Cl (hepar)Eliminasi utama ginjal Cl (tubuh total) = Cl (ginjal)

Gangguan fungsi hepar
Eliminasi kemampuan eliminasi obat yg mengalami metab hepatal (tgt keparahan penyakit) perlu penurunan dosis Berapa banyak perlu diturunkan, sulit ditentukan, krn parameter fungsi hepar yg menunj kemampuan eliminasi obat tidak ada.
Dianjurkan mengganti obat dg obat yg eliminasi
utamanya tidak melalui hepar

Gangguan fungsi hepar
distribusi obat. produksi albumin fraksi obat bebas pd obat2an yg terikat dg protein toksik
absorbsi. first pass effect terganggu fraksi obat bebas

• Cl kreatinin = sbg parameter penurunan fs ginjal. • RF = renal function
RF =
Dosis obat = RF X dosis lazim
Mis. Amikasin, eliminasi utama oleh ginjalpe fs ginjal t½ pemberian berulang : akumulasi toksik perlu pe dosis atau menjarangkan interval pemberian
Gangguan fungsi ginjal
Cl kreatinin pasien
Cl kreatinin normal

References:• Katzung, B.G. (1998) Basic and Clinical Pharmacology. 7th
ed. Appleton and Lange. Stamford, CT.• Brody, T.M., Larner,J., Minneman, K.P. and Neu, H.C. (1994)
Human Pharmacology: Molecular to Clinical. 2nd ed. Mosby-Year Book Inc. St. Louis, Missouri.
• Rang, H.P. et al. (1995) Pharmacology . Churchill Livingston. NY., N.Y.
• Harman, J.G. et al. (1996) Goodman and Gilman's The Pharmacological Basis of Therapeutics. 9th ed. McGraw Hill.