faal henoestasis
15
1 “ HEMOST ASIS” Yaitu pencegahan hilangnya darah, bila pembuluh darah mengalami cedera atau pecah Melalui beberapa cara : Ada 4 langkah : 1. Spasme 2. Pembentukan platelet plug 3. Koagulasi 4. Pembentuk an jaringan fibrous
-
Upload
agung-indra -
Category
Documents
-
view
229 -
download
0
Transcript of faal henoestasis

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 1/15
1
“ HEMOSTASIS”
Yaitu pencegahan hilangnya darah, bila pembuluh darah
mengalami cedera atau pecah
Melalui beberapa cara :
Ada 4 langkah :
1. Spasme
2. Pembentukan platelet plug
3. Koagulasi4. Pembentukan jaringan fibrous

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 2/15
2
1. Spasme P.darah :
Reflex saraf o.k rasa nyeri / impuls dr.
p.drh yang rusak
P. drh pecah Spasme miogenik setempat o.kkerusakan ddg p. drh
Faktor humoral setempat dr. jar. yang
kena trauma & trombosit darah
melepas
Vasokonstriktor tromboxan A2Makin parah kerusakan makin hebat spasmenya
Aliran darah dr p. drh yg pecah <<

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 3/15
3
2. Pembentukan sumbat trombosit (platelet plug )Terjadi pd perlukaan pembuluh darah yang berukuran kecil yg
terjadi tiap hariTromb luka pbl. drh tromb.bengkak irreg. dg. tonjolan, kontraksi protein kontraktil pelepasan granula-2 dgfaktor aktif trombosit lengket pd luka keluar ADP &tromboksan A2 mengaktifkan trombosit2 yang lainsaling melekat sumbat tromb. + benang-2 fibrin
sumbat rapat kuat Trauma permanen endotel tidak utuh platelet kontak
dengan serum kolagen agregasi platelet melepaskanzat kimia (ADP) permeabilitas platelet disekitarnyamenjadi lengket menempel pada agregat sebelumnya

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 4/15
Proses agregasi dipacu juga olehpembentukan TXA2, TXA2 secara :
langsung : memacu terbentuknya agregasiplatelet
tidak langsung : merangsang agregasi
platelet lebih lanjut melalui perangsanganterhadap pelepasan ADP.

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 5/15

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 6/15
6
“ Mekanisme Pembekuan Darah “
Teori Dasar : Tergantung dr keseimbangan antara Prokoagulan & Antikoagulan
Normal : Antikoagulan > dominan drpd koagulandarah tidak membeku
Pbl.drh rusak: Prokoagulan teraktivasi > aktivasi antikoagulan bekuan
3 Langkah Pembekuan :
1. Rangkaian reaksi kimiawi yang kompleks dengan lebihdari 12 faktor pembekuan terbentuk kompleksubstansi teraktivasi disebut activator protrombin :sebagai respon terhadap rupturnya pembuluh darah /kerusakan darah.
2. Aktivator protrombin : mengkatalisa perubahanprotrombin menjadi trombin
3. trombin sebagai enzim, mengubah fibrinogen menjadibenang-2 fibrin yang merangkai trombosit sel darah danplasma membentuk bekuan.

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 7/15
7
Clotting Factors
F I : Fibrinogen
F II : Prothrombin
F III : Tissue thromboplastin
F IV : Calcium
F V : Proaccelerin ; labile factor
Ac globulin (Ac-G)F VII : Stable F
F VIII : Antihaemophilic F.A
F IX : Antihaemophilic F.B
F X : Stuart Power FactorF XI : Antihaemophilic F.C
F XII : Hagemam F
F XIII : Fibrin stabilizing F

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 8/15
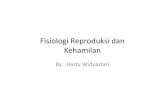
XII XIIa
XI XIa
IX
VIIIa,PL,Ca2+
IXa
Fibrin Monomer
Thrombin
Fibrinogen
Prothrombin
VVa
XaX
Factor VII
Ca2+
Tissue factor/Ca2+
Factor VIIa
Tissue factor (extrinsic system)
Cross-linked FibrinXIII
VIII
Contact Activation (intrinsic system)
Ca2+
PL,Ca2+
SECONDARY HEMEOSTASIS

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 9/15
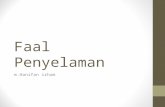
XIaXI
FDPs
TISSUE
INJURY
TF-VII
TF-VIIa
IXaIX
Anticoagulant
PathwayS-Prot
Factor V
VIIIa
XaX Va
APC
C-ProtII THROMBIN
Fibrinogen
Fibrinolytic
Pathway
FIBRIN Plasmin
TPA
PLASMINOGEN
Plasmin Inhibitor
TFPI
PT
APTT
PT &
APTT
TESTHEMOSTASIS & TROMBOSIS
Becomes active =
Activates =Inhibits =
9Povan,2004

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 10/15
TES HEMOSTASISScreening Tests Normal Value Measures Clinical Correlations
Primary Hemostasis
Platelet count 150,000 –300,000/ L Number of platelets per L Decreased platelet count (thrombocytopenia)—bleeding
usually not a problem until platelet count <50,000/mL;
high risk of spontaneous bleeding including CNS with
count <10,000/ L; usually due to decreased production
or increased destruction
Elevated platelet count (thrombocytosis)—commonly
reactive to inflammation or malignancy, or in
polycythemia vera; can be associated with hemorrhage
or thrombosis
Bleeding time(BT)
2.5 –10 min (template BT) Interaction between platelets and
the subendothelium
Prolonged BT caused by:
Thrombocytopenia (platelet count <50,000/ L)
Abnormal platelet function (vWD, ASA, NSAIDs

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 11/15
SECONDARY HEMOSTASIS
Prothrombin time
(PT) and
International
Normalized Ratio
(INR)
11–13 s, depending on
reagent; INR 1.0
Extrinsic system and common
pathway—factors VII, X,V,
prothrombin, and fibrinogen
Prolonged PT —most commonly caused by:
Use of warfarin (inhibits vitamin K–dependent
factors II, VII, IX, and X)
Liver disease with decreased factor synthesis
Antibiotics, some cephalosporins,
(moxalactam, cefamandole, cefotaxime,
cefoperazone) that inhibit vitamin K–dependent
factors
Activated partial
thromboplastin
time (aPTT)
22–34 s Intrinsic system and common
pathway including factors XII,
XI, IX, VIII, X, V, prothrombin,
and fibrinogen
Prolongation of aPTT most commonly caused
by:
Depends on type of
thromboplastin used;
"activated" with Kaolin
Heparin therapy
Factor deficiencies; factor levels have to be
>30% of normal to cause prolongation

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 12/15
Con’t
Thrombinclotting time(TCT)
10–12 s Conversion of fibrinogen to
fibrin monomer Prolonged TCT caused by:
Low fibrinogen level (DIC)
Abnormal fibrinogen molecule (liver
disease)
Presence of heparin, FDPs or a
paraprotein (multiple myeloma); theseinterfere with the conversion
Very high fibrinogen level (acute phase
reactant)
"Mixes" Variable Performed when one or more of
the above screening tests is
prolonged; the patient's plasma("abnormal") is mixed with
"normal" plasma and the
screening test is repeated
If the "mix" corrects the screening test,
one or more factor deficiencies are
present.
If the "mix" does not correct the
screening test, an inhibitor

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 13/15
TES KOAGULASI
ABNORMAL
PT APTT normal
• Warfarin, def. vitamin K, early liver disease, defisiensikongenital faktor VII deficiency.
PT APTT
•
Overdosis warfarin, def. vitamin K, liver failure, DIC.PT normal APTT
• Unfractionated heparin (UFH), haemophilia A or B, lupusanticoagulant , rarely vWD affects APTT, factor VIIIinhibitors are rare but typically prolong APTT.
PT normal APTT normal
• PT and APTT normal (do not exclude a significant bleedingtendency, for example effect of low molecular weightheparin, mild factor deficiency, platelet abnormality, or veryrare factor deficiency such as factor XIII )

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 14/15

8/13/2019 faal henoestasis
http://slidepdf.com/reader/full/faal-henoestasis 15/15