Dr. H. I. Firmansyah, SpPD, KPTI, FINASIM Pendidikan · Ketua Komite PPRA RSPI Sulianti Saroso...
27
Pendidikan: Dokter Umum FKUY 1989 Spesialis Penyakit Dalam FKUI 2003 Institute of Tropical Medicine Prince Leopold, Antwerpen, Belgium 2005 Fellow of Indonesian Society of Internal Medicine 2009 Konsultan Penyakit Tropik & Infeksi FKUI 2013 Pekerjaan: Ka.SMF Penyakit Dalam RSPI Sulianti Saroso, 2014-sekarang Ketua Komite PPRA RSPI Sulianti Saroso 2015-sekarang Pembimbing Klinik Residen Divisi Penyakit Tropik & Infeksi, Departemen Ilmu Penyakit Dalam FKUI, 2006-sekarang Pembimbing Klinik Mahasiswa FK Untar, 2005-sekarang Koordinator Bidang Pelayanan Pokja HIV-AIDS RSPI-SS, 2004-2015 Ketua Komite PPI RSPI-SS, 2004-2014 Organisasi: Ketua Perhimpunan Pengendalian Infeksi Indonesia (PERDALIN JAKARTA), 2016-sekarang Anggota Perhimpunan Konsultan Penyakit Tropik dan Infeksi Indonesia (PETRI), 2006-sekarang Dr. H. I. Firmansyah, SpPD, KPTI, FINASIM
Transcript of Dr. H. I. Firmansyah, SpPD, KPTI, FINASIM Pendidikan · Ketua Komite PPRA RSPI Sulianti Saroso...

Pendidikan:Dokter Umum FKUY 1989Spesialis Penyakit Dalam FKUI 2003Institute of Tropical Medicine Prince Leopold, Antwerpen, Belgium 2005Fellow of Indonesian Society of Internal Medicine 2009Konsultan Penyakit Tropik & Infeksi FKUI 2013
Pekerjaan:Ka.SMF Penyakit Dalam RSPI Sulianti Saroso, 2014-sekarang Ketua Komite PPRA RSPI Sulianti Saroso 2015-sekarangPembimbing Klinik Residen Divisi Penyakit Tropik & Infeksi, Departemen Ilmu Penyakit Dalam FKUI, 2006-sekarangPembimbing Klinik Mahasiswa FK Untar, 2005-sekarangKoordinator Bidang Pelayanan Pokja HIV-AIDS RSPI-SS, 2004-2015Ketua Komite PPI RSPI-SS, 2004-2014
Organisasi:Ketua Perhimpunan Pengendalian Infeksi Indonesia (PERDALIN JAKARTA), 2016-sekarangAnggota Perhimpunan Konsultan Penyakit Tropik dan Infeksi Indonesia (PETRI), 2006-sekarang
Dr. H. I. Firmansyah, SpPD, KPTI, FINASIM
KEY POINTS
• Resistant bacterial strains are selected in hospitals due to huge usage of antibiotics
• To preserve the susceptibility of microorganism, and postpone the development of resistance, antibiotics should be used rationally
• If resistant bacteria develop in an environment where the specific antibiotic used, they will become prevalent in that environment
• Good antibiotic prescribing practices should be encouraged within hospitals
• The microbiology laboratory service can asisstclinicians to use targeted antibiotic treatment for patients
1. Mendes RE, et al. Antimicrob Agents Chemother. 2013 Nov;57(11):5721-6
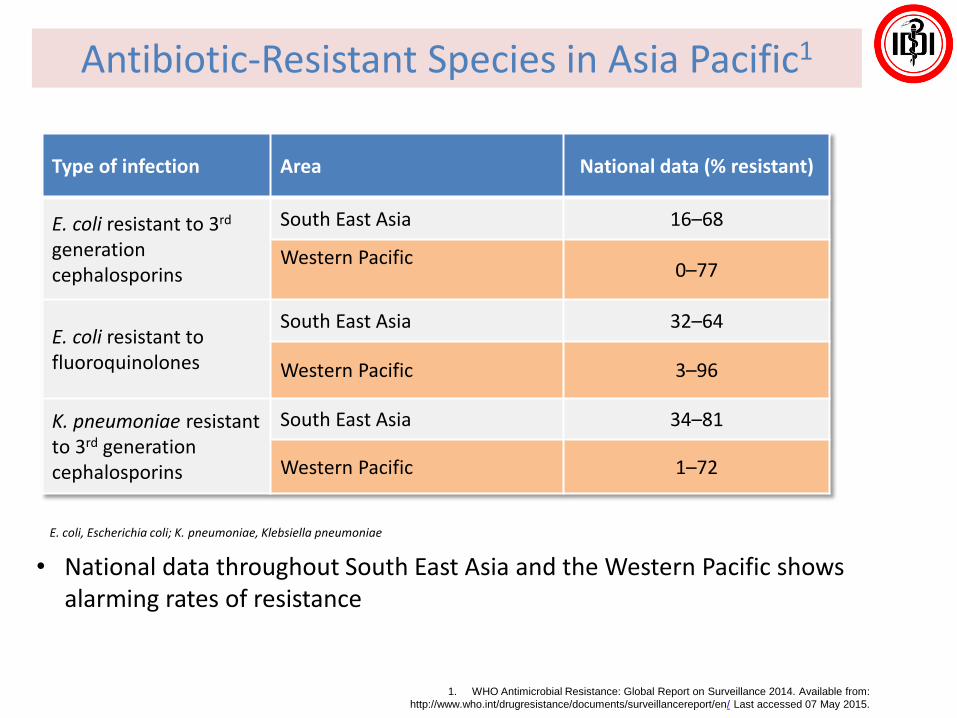
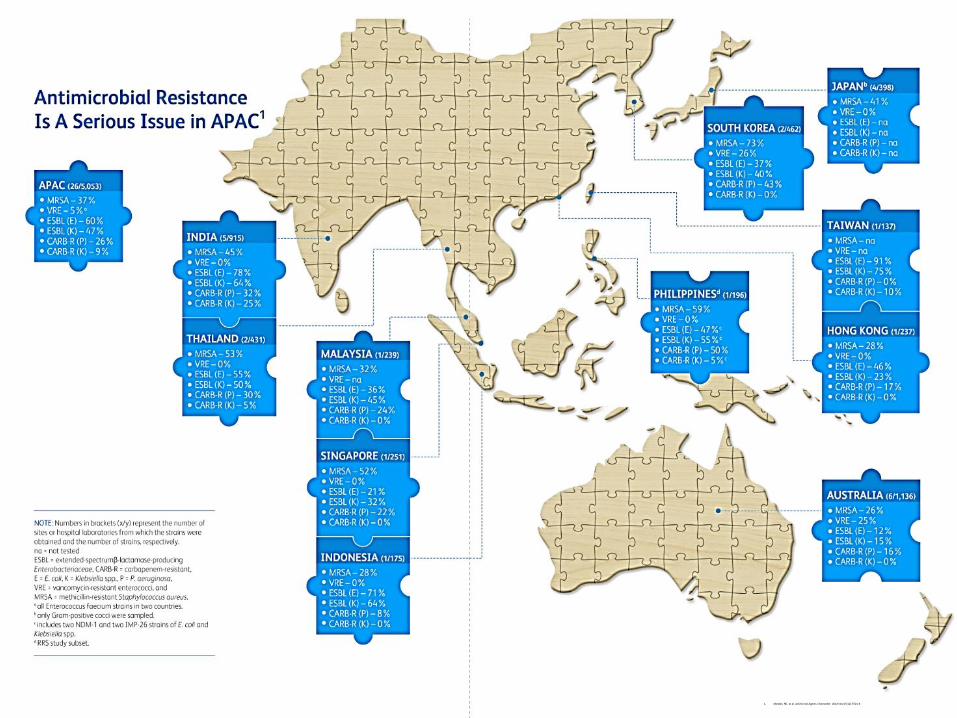
Antibiotic-Resistant Species in Asia Pacific1
• National data throughout South East Asia and the Western Pacific shows alarming rates of resistance
Type of infection Area National data (% resistant)
E. coli resistant to 3rd
generation cephalosporins
South East Asia 16–68
Western Pacific0–77
E. coli resistant to fluoroquinolones
South East Asia 32–64
Western Pacific 3–96
K. pneumoniae resistant to 3rd generation cephalosporins
South East Asia 34–81
Western Pacific 1–72
E. coli, Escherichia coli; K. pneumoniae, Klebsiella pneumoniae
1. WHO Antimicrobial Resistance: Global Report on Surveillance 2014. Available from:
http://www.who.int/drugresistance/documents/surveillancereport/en/ Last accessed 07 May 2015.
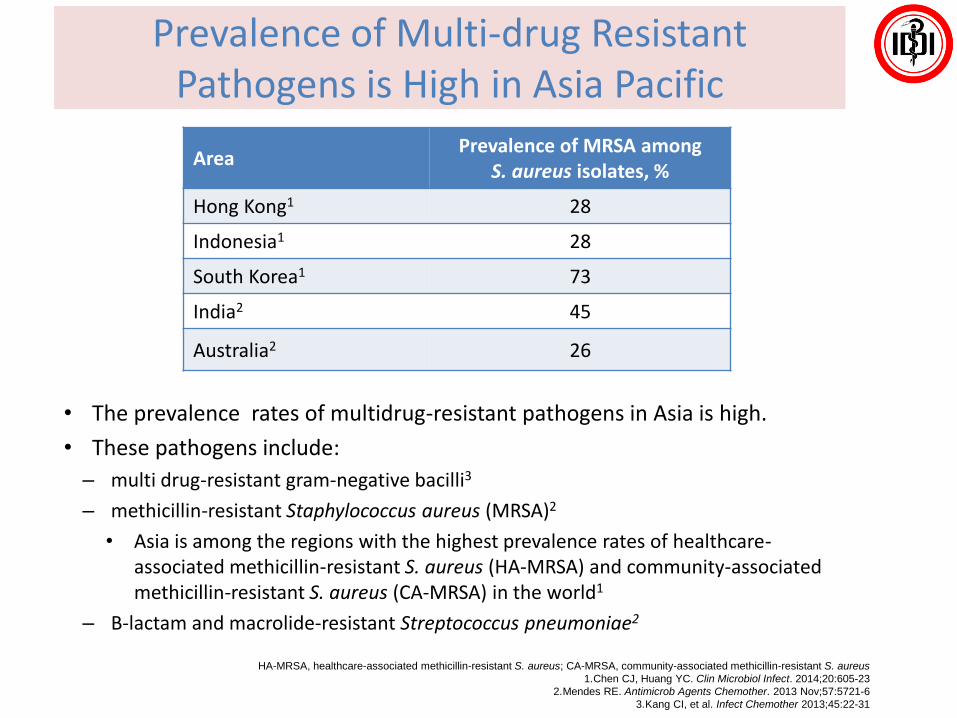
Prevalence of Multi-drug Resistant Pathogens is High in Asia Pacific
• The prevalence rates of multidrug-resistant pathogens in Asia is high.
• These pathogens include:
– multi drug-resistant gram-negative bacilli3
– methicillin-resistant Staphylococcus aureus (MRSA)2
• Asia is among the regions with the highest prevalence rates of healthcare-associated methicillin-resistant S. aureus (HA-MRSA) and community-associated methicillin-resistant S. aureus (CA-MRSA) in the world1
– Β-lactam and macrolide-resistant Streptococcus pneumoniae2
AreaPrevalence of MRSA among
S. aureus isolates, %
Hong Kong1 28
Indonesia1 28
South Korea1 73
India2 45
Australia2 26
HA-MRSA, healthcare-associated methicillin-resistant S. aureus; CA-MRSA, community-associated methicillin-resistant S. aureus
1.Chen CJ, Huang YC. Clin Microbiol Infect. 2014;20:605-23
2.Mendes RE. Antimicrob Agents Chemother. 2013 Nov;57:5721-6
3.Kang CI, et al. Infect Chemother 2013;45:22-31
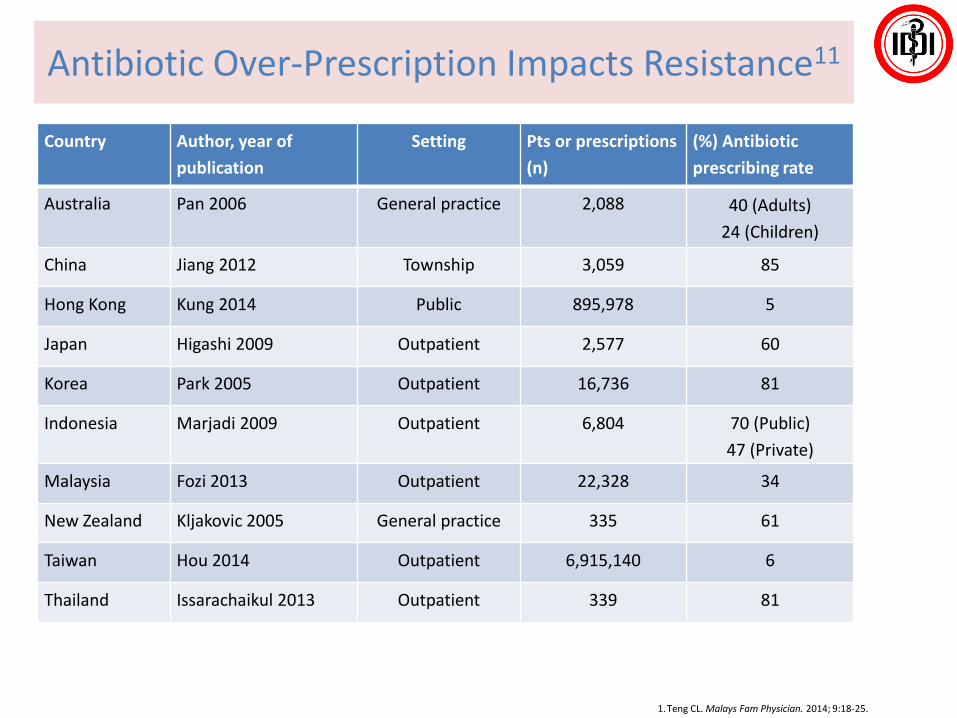
Antibiotic Over-Prescription Impacts Resistance11
1.Teng CL. Malays Fam Physician. 2014; 9:18-25.
Country Author, year of
publication
Setting Pts or prescriptions
(n)
(%) Antibiotic
prescribing rate
Australia Pan 2006 General practice 2,088 40 (Adults)
24 (Children)
China Jiang 2012 Township 3,059 85
Hong Kong Kung 2014 Public 895,978 5
Japan Higashi 2009 Outpatient 2,577 60
Korea Park 2005 Outpatient 16,736 81
Indonesia Marjadi 2009 Outpatient 6,804 70 (Public)
47 (Private)
Malaysia Fozi 2013 Outpatient 22,328 34
New Zealand Kljakovic 2005 General practice 335 61
Taiwan Hou 2014 Outpatient 6,915,140 6
Thailand Issarachaikul 2013 Outpatient 339 81
ANTIBIOTIC GUIDELINES
• Demonstrate a commitment to rational and prudent use of antibiotics
• Policies should focus on using antibiotics with the narrowest spectrum, which are cheap, have minimal toxicity and have the least impact on development of resistance
MRSA, methicillin-resistant Staphylococcus aureus
1. . Song JH. Antimicrobial Resistance Control 2015. Available from http://www.globalhealthdynamics.co.uk/wp-content/uploads/2015/05/06_Song.pdf. Accessed 08 June 2015.
2. Teng CL. Malays Fam Physician. 2014; 9:18–253. Chen CJ, Huang YC. Clin Microbiol Infect. 2014;20:605-23
4. Mendes RE. Antimicrob Agents Chemother. 2013 Nov;57:5721-65. Kang CI, et al. Infect Chemother 2013;45:22-31
Image source: © James Thew
Antimicrobial Resistance
9
• Inappropriate use, poor drug
quality and patient non-
compliance with therapy all
contribute to thedevelopment
of antimicrobial resistance1
• There are several multi-drug resistant pathogens (such as
MRSA and multi-drug resistant gram negative bacilli) which are
a significant issue and present in both the hospital and
community setting2–5
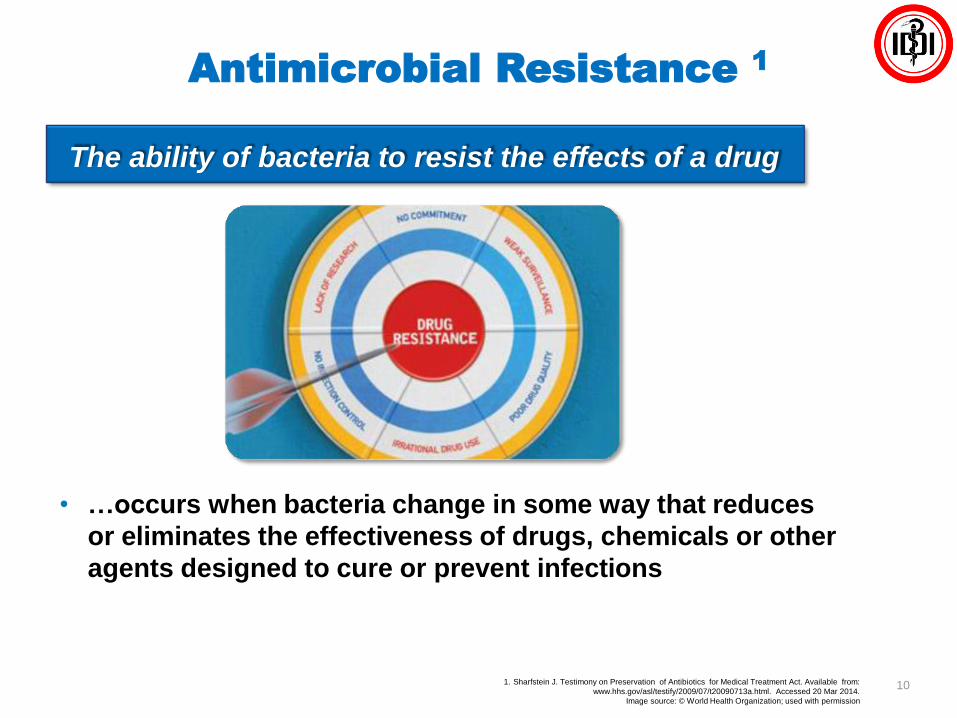
Antimicrobial Resistance 1
101. Sharfstein J. Testimony on Preservation of Antibiotics for Medical Treatment Act. Available from:
www.hhs.gov/asl/testify/2009/07/t20090713a.html. Accessed 20 Mar 2014.
Image source: © World Health Organization; used with permission
• …occurs when bacteria change in some way that reduces
or eliminates the effectiveness of drugs, chemicals or other
agents designed to cure or prevent infections
The ability of bacteria to resist the effects of a drug
1. Mulvey MR, Simor AE. CMAJ 2009;180:408-15.
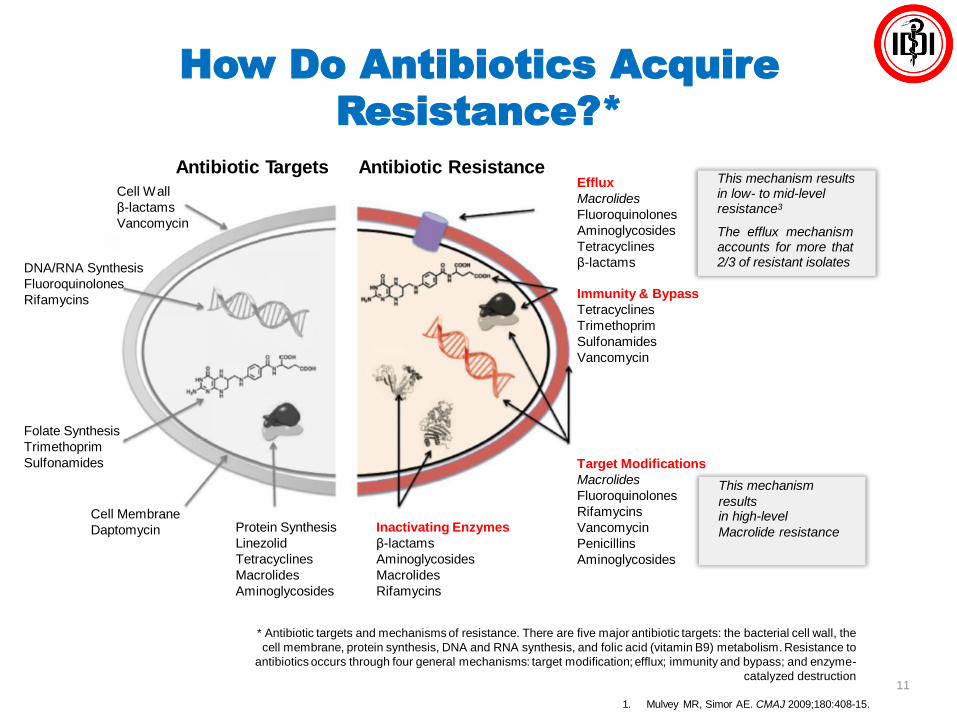
How Do Antibiotics Acquire
Resistance?*
Antibiotic Targets Antibiotic Resistance
Cell Wall
β-lactams
Vancomycin
DNA/RNA Synthesis
Fluoroquinolones
Rifamycins
Folate Synthesis
Trimethoprim
Sulfonamides
Cell Membrane
Daptomycin Protein Synthesis
Linezolid
Tetracyclines
Macrolides
Aminoglycosides
Inactivating Enzymes
β-lactams
Aminoglycosides
Macrolides
Rifamycins
Immunity & Bypass
Tetracyclines
Trimethoprim
Sulfonamides
Vancomycin
Efflux
Macrolides
Fluoroquinolones
Aminoglycosides
Tetracyclines
β-lactams
Target Modifications
Macrolides
Fluoroquinolones
Rifamycins
Vancomycin
Penicillins
Aminoglycosides
This mechanism results in low- to mid-level resistance3
The efflux mechanismaccounts for more that2/3 of resistant isolates
This mechanism
resultsin high-level
Macrolide resistance
11
* Antibiotic targets and mechanisms of resistance. There are five major antibiotic targets: the bacterial cell wall, the
cell membrane, protein synthesis, DNA and RNA synthesis, and folic acid (vitamin B9) metabolism. Resistance to
antibiotics occurs through four general mechanisms: target modification; efflux; immunity and bypass; and enzyme-
catalyzed destruction
By Drug Inactivation or Modification1
12
• Bacteria can produce enzymes that modify or destroy the
chemical structure of the antibiotic
• The most common resistance-producing enzymes are the
β-lactamases
– Hydrolyse the β-lactam ring of penicillins, cephalosporins and carbapenems
• Two important β-lactamase subfamilies, primarily
responsible for causing resistance in Gram-negative
bacteria):
– Carbapenemases
• Metallo-β-lactamases (IMP, VIM, NDM-1), oxacillinase (OXA) and
Klebsiella pneumoniae carbapenemase (KPC) are among the most
important subtypes
– Extended-spectrum β-lactamases (ESBLs)
• TEM, SHV, CTX-M and OXA are the most common gene mutations
producing resistance
1. Mulvey MR, Simor AE. CMAJ 2009;180:408-15.
By Altering the Target Site1
13
• Antimicrobial efficacy is dependent on site-specific binding to, or within, the target pathogen
– The site varies between drug classes
• Resistance occurs when the pathogen changes the structureof the target
– Either prevents binding or reduces binding affinity
• Example: altered binding proteins in cell wall– Organisms: Streptococcus pneumoniae, MRSA
– Antibiotics affected: penicillin, methicillin, cloxacillin
• Example: altered DNA gyrase or topoisomerase– Organisms: S. pneumoniae, Pseudomonas aeruginosa,
Enterobacteriaceae
– Antibiotics affected: ciprofloxacin, levofloxacin, moxifloxacin
MRSA, methicillin-resistant Staphylococcus aureus
1. Mulvey MR, Simor AE. CMAJ 2009;180:408-15.
By Decreasing Drug Accumulation1
14
• To be effective, antimicrobials must achieve adequate concentrations at
their target sites
• There are two mechanisms by which pathogens prevent this:
– Decreased permeability
• Arises from mutations in genes coding for porins – outer membrane proteins that
allow diffusion of molecules into the bacterial cell
– Increased drug efflux
• Occurs where pathogens have evolved an active efflux mechanism that pumps
drugs out of the cytoplasm before they can bind to their target
• Some pumps are specific for a single drug class, others are multidrug resistant
• Example: change in outer membrane porins
– Organisms: Enterobacteriaceae, P. aeruginosa
– Antibiotics affected: gentamicin, tobramycin
• Example: efflux pump
– Organisms: S. aureus, streptococci
– Antibiotics affected: tetracycline, clindamycin, erythromycin
1. Mulvey MR, Simor AE. CMAJ 2009;180:408-15.
By Altering Metabolic Pathways
• Another resistance mechanism
used by bacteria is the bypass
of steps previously inhibited
by antibiotics1
– e.g. sulphonamides are chemical
competitive analogs of para-
aminobenzoic acid (PABA), and
inhibit folic acid and nucleic acid in
bacteria2
– Resistant bacteria avoid the need
for the PABA pathway by using
preformed folic acid instead2
Bypass Pathways
A + B AB
151. Coates A, et al. Nature Rev Drug Discovery 2002;1:895-910.
2. Sulfadiazine Tablets USP. Drugs.com. Available from: http://www.drugs.com/pro/sulfadiazine.html?printable=1. Last accessed 25 Apr 2014.
Gram-Positive and Gram-Negative
Organisms Develop Resistance
16
1. Huttner A, et al. Antimicrob Resist Infect Control 2013;2:31.
• Although resistance in Gram-positive organisms is
familiar, resistance among Gram-negative bacteria
is growing1
Resistant Gram-positiveorganisms, including…
S. aureus
Enterococcus faecium
Enterococci
Clostridium difficile
Resistant Gram-negativeorganisms, including…
Enterobacteriacae
Acinetobacter spp.
Klebsiella spp.
P. aeruginosa
Escherichia coli
Burkholderia cepacia
Proteus mirabilis
Neisseria gonorrhoeae
Who Should Prescribe Antibiotics?
171. CDC. Antibiotics Aren’t Always the Answer. Available from: www.cdc.gov/features/getsmart/. Accessed 8 Apr 2014.
2. WHO Fact Sheet. Rational Use of Medicines. Available from: www.who.int/mediacentre/factsheets/fs338/en/. Accessed 8 Apr 2014.
• Antibiotics are prescription medicines
– Antibiotics should only be used when a doctor determines
that they are needed to treat a bacterial infection1
• Antibiotics need to be prescribed by a doctor
– No other healthcare professionals should provide or
dispense antibiotics without a doctor ’s prescription
• Distribution of antibiotics by anyone other than a
doctor leads to problems, such as overuse,
inappropriate self-medication and use of the wrong
dosage2
Antibiotic Prescription in the Community
181. Suda KJ, et al. J Am Pharmacist Ass 2012;52:6-10.
2. NICE Clinical Guideline 69
Image source: © KOUNADEAS IOANNHS
• The majority of antibiotic prescriptions in the outpatient
setting are for upper respiratory tract infections (URTIs)1
– Ear infection, sinusitis, pharyngitis, sore throat, coughs/colds
• However, not all need to be treated immediately with
antibiotics2
• Depending on clinical assessment of severity, a no
antibiotic or delayed antibiotic prescribing strategy is
recommended for adults or children with:2
– Acute ear infection
– Acute sore throat, pharyngitis or tonsillitis
– Common cold
– Acute rhinosinusitis
– Acute cough or bronchitis
When a Doctor May
Prescribe Antibiotics1
URTI, upper respiratory tract infection
1.CDC Adult Appropriate Antibiotic Use Summary. Available from:
www.cdc.gov/getsmart/campaign-materials/info-sheets/adult-approp-summary.pdf. Accessed 18 Mar 2014.
Non-specific upper respiratory tract infections (adult)
• Non-specific URTIs or acute rhinopharyngitis, in the
absence of sinus, pharyngeal and lower airway
symptoms, are typically VIRAL in origin1
• Antibiotic treatment is NOT RECOMMENDED1
– Antibiotics do not enhance illness resolution or prevent
complications
• Purulent secretions are common in patients with
URTIs, but do not predict bacterial infection or benefit
from antibiotic treatment1
42
Acute pharyngitis (adult)
• The aetiological agent in ≈10% cases of pharyngitis is Group
A beta haemolytic streptococcus (GABHS)
• Acute pharyngitis is self-limiting in the large majority of
adults, who need SUPPORTIVE CARE ONLY
• Limit antibiotic prescription to patients most likely to have
GABHS infection
– History of fever, tonsillar exudates, absent cough, lymphadenitis
– Penicillin or amoxicillin preferred
– Treat for 10 days
– First-generation cephalosporin, clindamycin, clarithromycin or
azithromycin in penicillin-allergic patients
.
43
1. CDC Adult Appropriate Antibiotic Use Summary. Available from: www.cdc.gov/getsmart/campaign-materials/info-sheets/adult-approp-summary.pdf. Accessed 18 Mar 2014.
2. Shulman ST, et al. Clin Infect Dis 2012;55:1279–82.
When a Doctor May
Prescribe Antibiotics1
When a Doctor May
Prescribe Antibiotics1,2
1. CDC Adult Appropriate Antibiotic Use Summary.
Available from: www.cdc.gov/getsmart/campaign-materials/info-sheets/adult-approp-summary.pdf. Accessed 18 Mar 2014.
2. Chow AW, et al. Clin Infect Dis 2012;54:1041-5
Rhinosinusitis (adult)
• Diagnose acute bacterial rhinosinusitis if:
– Symptom duration ≥7 days; maxillary facial/tooth pain or
tenderness are present; purulent secretions are evident
• Resolves WITHOUT ANTIBIOTIC TREATMENT in the
majority of cases
• Reserve antibiotics for patients with moderate-to-severe
symptoms
• Initiate empiric antibiotic treatment with the most
narrow-spectrum agent active against the likely
pathogens
44
When a Doctor May
Prescribe Antibiotics1
1. CDC Adult Appropriate Antibiotic Use Summary. Available from: www.cdc.gov/getsmart/campaign-materials/info-sheets/adult-approp-summary.pdf. Accessed 18 Mar 2014.
Bronchitis (adult)
• Focus on ruling out pneumonia in adults with an
acute cough illness
– Pneumonia is uncommon in the absence of vital sign
abnormalities or asymmetrical lung sounds
• Routine antibiotic treatment of uncomplicated
bronchitis is NOT RECOMMENDED
– In the unlikely event pertussis is suspected, perform a
diagnostic test and initiate antibiotics
45
When a Doctor May
Prescribe Antibiotics1
CAP, community-acquired pneumonia
1. Mandell LA, et al. Clin Infect Dis 2007;44(Suppl.2):S27-72.
Community-acquired pneumonia (adult)
• Initial empirical antibiotic therapy is recommended
– A macrolide (azithromycin, clarithromycin or erythromycin) (or
doxycycline) in previously healthy outpatients with no risk factors
for drug-resistant S. pneumoniae
• When the infection aetiology has been determined,
pathogen-directed antibiotic therapy is appropriate
• Treatment duration typically ≥5 days for most antibiotics
‒ Some antibiotics, such as azithromycin, require a shorter course
‒ Patients need to be afebrile for 48–72 hours and have
≤1 CAP-associated sign of clinical instability before antibiotic
therapy is discontinued
46
When a Doctor May
Prescribe Antibiotics1,2
1. Fujimoto T. Japan Med Ass J 2009;52:158–63.
2. NICE Clinical Guideline 69.
Ear infection
• Infection resolves spontaneously in 80% of patients1
• A no antibiotic or delayed antibiotic prescribing
strategy is recommended1,2
• Observe for 3 days after symptom onset1
• Start empirical antibiotic therapy after 3 days in
patients who fail to improve or who have more severe
symptoms1
47
When a Doctor May Prescribe
Antibiotics: Special Patient Groups
25RTI, respiratory tract infection
1. NICE Clinical Guideline 69
• In patients with RTIs, immediate antibiotic prescription
and/or further investigation and management should be
offered in the following situations:
– The patient is systemically very unwell
– Signs/symptoms of serious illness and/or complications are present
– When pre-existing co-morbidity puts the patient at high risk of
serious complications
– Acute cough and patient age >65 years with ≥2 of the following or
>80 years and ≥1 of the following:
• Hospitalisation in previous year
• Type 1 or type 2 diabetes
• History of congestive heart failure
• Current use of oral glucocorticoids
CONCLUSION
• Every hospital should make the AB guidelines for empirical treatment
• Implementing of AB guidelines should be done through continuing workshop
• Measuring of AB effectiveness based on local guidelines should be done periodically based on pharmacologic and microbiologic site
ight drug
ight time
ight dose
ight duration
+Infection
ControlRRIGHT DIAGNOSIS
Successful Antibiotic Therapy