Capita Selecta-blok 6
29
Herry A. Kapita Selecta Blok VII FK UNSRI Patophysiolog y Gangguan Keseimbangan Na +
-
Upload
maya-rentina -
Category
Documents
-
view
222 -
download
0
description
ada
Transcript of Capita Selecta-blok 6

Herry A.Kapita Selecta Blok VIIFK UNSRI
Patophysiology Gangguan Keseimbangan Na+

Laki-laki, umur 23 tahun. Dibawa ke RS karena diare sejak 2 hari yang lalu. Tidak nafsu makan dan hanya minum air putih dan teh manis. Pada pemeriksaan didapati kondisi umum pasien lemah, compos mentis, nadi 100 x/menit. Tekanan darah baring 120/80 mmHg dan pada posisi berdiri 100/70 mmHg. Turgor kulit sedikit menurun. Tidak ada kelainan neurologis.

Bagaimana TBW ?
Normovomelic (Euvolemic)
Hypovolemic Hypervolemic

Postural /Orthostatic Hypotension
Sudden fall in blood pressure, typically greater than 20/10 mmHg, that occurs when a person assumes a more vertical postion i.e from sitting to standing or from lying down to sitting or standing (Wikidoc)

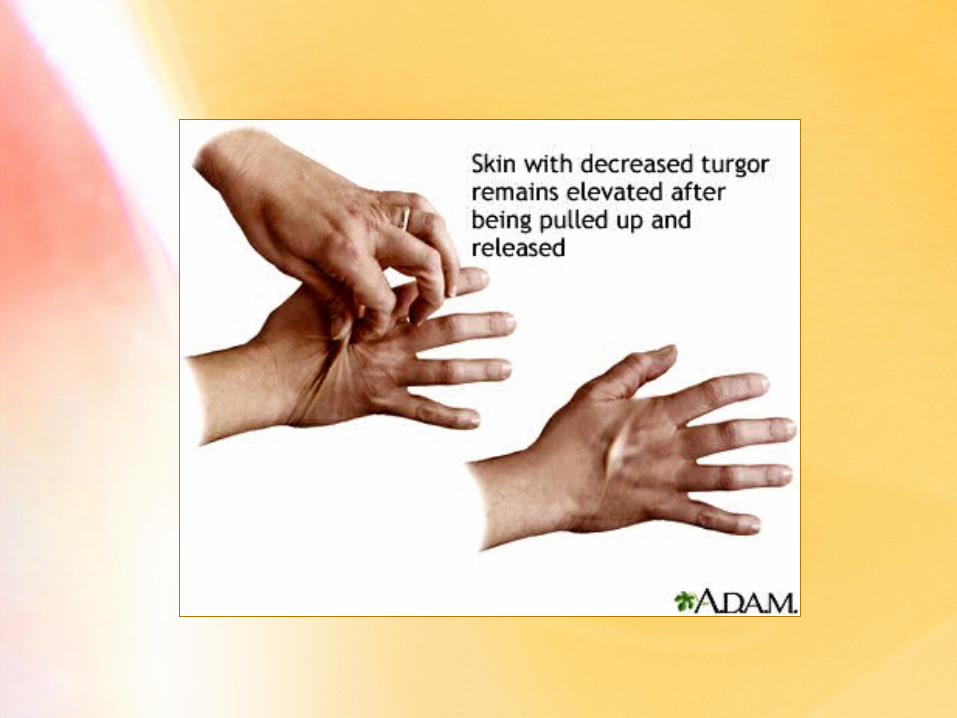
Skin Turgor [ter´ger] The skin's ability to change shape and return to normal (elasticity). To determine skin turgor grasps the skin on the back of the hand, lower arm, or abdomen between two fingers so that it is tented up. The skin is held for a few seconds then released.Skin with normal turgor snaps rapidly back to its normal position. Skin with decreased turgor remains elevated and returns slowly to its normal position (MedlinePlus).

Nadi 100 x/menit Postural hypotension
Skin Tugor
Hypovolemic(Dehidration)
HypovolemicMild Kehilangan cairan 3 – 5% TBWModerate 6 – 10% TBWSevere > 10% TBWShock > 15% TBW

Pemeriksaan laboratorium, didapati;Glucose 90 mg/dlBUN 42 mg/dl (9 – 25)Creatinine 1,2 mg/dl (0,8 – 1,2)Na+ 120 mEq/l (135 – 145)K+ 3,5 mEq/l (3,5 – 5)
Hyponatremic

Posm = 2 (Na+) +(Glukosa)
18
(BUN)2,8
+
Urea osmotik tidak efektif.
Glukosa, normal, osmotik tidak efektif.
Posm efektif = 2 (Na+)Posm efektif = 2 (Na+)
Rumus Menghitung Osmolaritas Plasma/CES
Berapa Osmolaritas Cairan Tubuh ?

Posm = (2x120 + 90/18 + 35/2,3) mOsm/l(240 + 5 + 15) mOsm/l260 mOsm/l
Posm efektif = 2(NA+) mOsm/l240 mOsm/l
Posm normal =285 ± 10 mOsm/l
Hypoosmotic

Hypovolemic hypoosmolar hyponatremic State !
Pasien dalam kondisi :
Bagaimana kondisi ini terjadi ?
Pasien ini mengalami diare berat disebabkan viral gastroenteritis. Cairan diare mengandung Na+ dan K+ ± 85 mEq/l.
Berat badan sebelum diare 60 kg. Saat pemeriksaan BB = 56,4 kg.
TBW = 60 x 60% = 36 literKehilangan cairan = 60 – 56,4= 3,6 liter (10%) + elektrolit (?)

Diare
Kehilangan air
Kehilangan elektrolit (terutama Na+)
Input
Air tanpa elektrolit
Hypovolemic Hyponatremic

Hyponatremic
Osmoreceptor
ADH Reabsorbsi air di collecting
duct
Urine output
Hypoosmotic

HIPOVOLEMIA
Baroreceptor
Sekresi Renin di ginjal
AngiotensinogenAngiotensin I
Angiotensin II
Renin
Sekresi Aldosteron EKSKRESI Na+
Na+ di CES Volume CES
Sekresi ANF
Sekresi ADH
Haus
AIRInput
Output
Kehilangan cairan 10% TBW
VASOKONSTRIKSI
Reabsorbsi Na+ (di collecting duct)

Koreksi Hyponatremia
Na+ deficit = TBW {(Na+)desired – (Na+)current}
Na+ deficit = 36 (130 – 120) mEq
= 360 mEq
Cairan infus NaCl 3% (Na+) = 513 mEq/l
NaCl 3% yang dibutuhkan = 360/513 x 1000 ml= 700 ml
over the first 8-12 hours at rate of 25-50 mL/hour, not to exceed a maximum rate of 100 mL/hour.
Mengapa TBW bukan CES ?

C I S C E S
K+ 145 mEq/l Na+ 145 mEq/l
24 liter 12 liter
360 mOsm NaCl
Apabila kedalam CES ditambahkan …
H2O
Osmolaritas 290 mOsm/l
Osmolaritas

C I S C E S
K+ 150 mEq/l Na+ 150 mEq/l
23,1 liter 12,9 liter
Osmolaritas 300 mOsm/l
Setelah tercapai keseimbangan baru …

Mengapa BUN meningkat ?
Volume Depletion
RBF
GFR Ekskresi Ureum
oleh ginjal

Hyponatremic SymptomsAbnormal mental status
ConfusionDecrease consciousnessHallucinationsPosible coma
ConvulsionsFatique IrritabilityHeadacheLoos of appetite Muscle spasms or crampsMuscle weaknessNauseaRestlessnessVomiting

140 mEq/l 140 -> 119 mEq/l in 2h
140 -> 122 mEq/l in 3d
140 -> 99 mEq/l in 16 d
320
340
360
380
400
420
440
460
Perubahan Kandungan Air Otak karena Hyponatremia
Normal
Mati
Asymptomatic Lethargic
Bra
in W
ater
g/1
00 g
dry
wei
gh
t

Peran Sistem Circulasi pada Hypovolemic State Penurunan tekanan darah Melalui Baroreceptor
Pusat Vasomotor aktivasi sistem syaraf sympathis.
Jantung meningkatkan denyut jantung meningkatkan kontraksi jantung
Pembuluh darah Vasokonstriksi perifer

Di AS hukuman mati di kursi listrik sudah dianggap tidak manusiawi, karena itu diganti dengan suntikan mati. Terhukum pertama diberi injeksi obat penenang, kemudian obat pelemas otot, terakhir diberikan injeksi larutan KCl intravena. Hanya dalam beberapa menit, terhukum mati karena henti jantung (cardiac arrest).
Patophysiologi Ganguan Keseimbangan K+

)(KP )(NaP
)(KP )(NaP log 61,5 - V
iKiNa
oKoNa
Resting Membrane Potential
PK > 100 x PNa
Ko = 4 mEq/l dan Ki = 140 mEq/l
Perubahan (K+) CES perubahan Membran Potential

Perubahan Potential Membran
-70 mV
0 mV
+ 30 mV
Depolarisasi
Repolarisasi
Overshoot
Hiperpolarisasi- 90 mV
Garis Isopotential
Potential Membran Istirahat
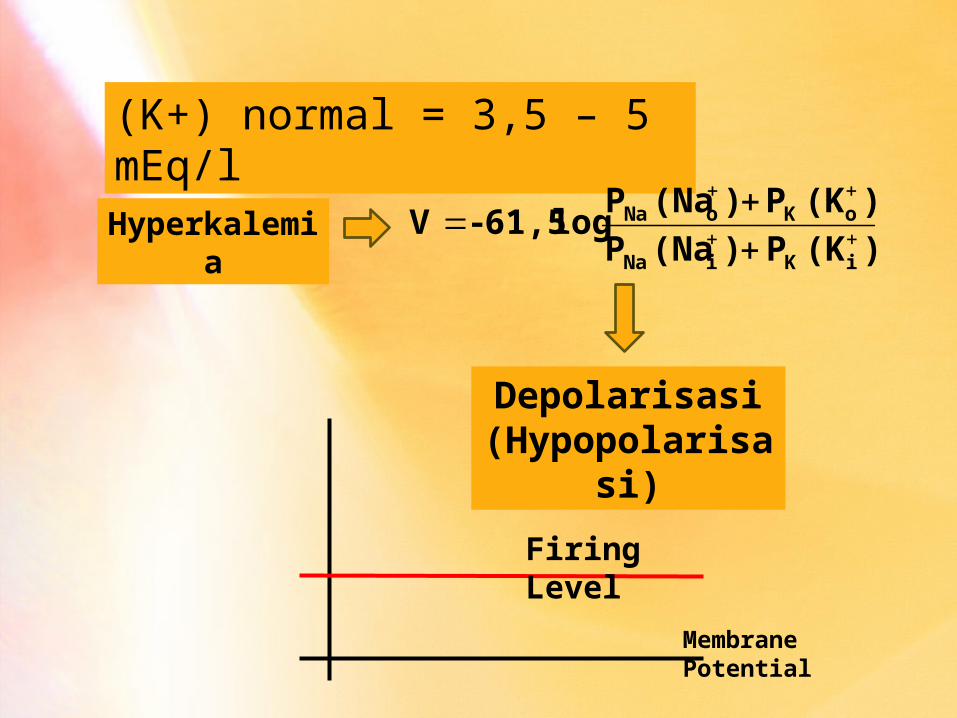
(K+) normal = 3,5 – 5 mEq/l
Hyperkalemia)(KP )(NaP
)(KP )(NaP log 61,5 - V
iKiNa
oKoNa
Depolarisasi(Hypopolarisasi)
Firing Level
Membrane Potential

ReferenceRose, B.D. & Post, T.W. 2001; Clinical Physiology of Acid-Base and Electrolyte Disoders, 5thed, McGraw Hill.

Sekian