achalasia.docx

of 12
-
Upload
rinaldi-sobli -
Category
Documents
-
view
13 -
download
0
Transcript of achalasia.docx
PENATALAKSANAAN DYSFAGIA AKIBAT ACHALASIA OESOFAGUSBakti SetioPendahuluan Dysfagia adalah kesukaran makan akibat gangguan dalam proses menelan dengan dampak negatif terhadap kesehatan dan kualitas hidup dan pada kasus berat berdampak juga terhadap kesehatan mental dan sosial 1-3. Berdasarkan proses fisiologi menelan maka disfagia dapat terjadi pada fase oral, fase faringeal dan fase esofagal. Kelainan ini harus dipikirkan secara serius oleh karena dapat menyebabkan aspirasi pneumonitis, aspirasi pneumonia dan bahkan kematian 3,4. Di Amerika Serikat diperkirakan 15 sampai dengan 40 % populasi dengan usia lebih dari 60 tahun mempunyai masalah dengan disfagia dan diperkirakan pada tahun 2010 hampir 16.500.000 individu memerlukan perhatian akan disfagia 4,5 .ndisfagia orofaring diperkirakan mengenai 22 % populasi dunia yang berumur lebih dari 50 tahun 6.Pada fasilitas kesehatan diperkirakan mengenai 20-30 % pasien rawat akut dan 59-66 % pasien rawat inap kronik dan dimasyarakat disfagia diperikan mengenai 14 % populasi usia lebih dari 65 tahun 6. Literatur lain mengatakan bahwa gangguan menelan terjadi pada sekitar 20 % individu berusia lebih dari 50 tahun dan 60 % pada pasien nursing home 7. Penulis tertarik untuk membahas permasalahan disfagia ini dikarenakan di rumah sakit daerah tingkat kabupaten banyaknya kasus disfagia yang tidak tertangani secara tuntas, keterbatasan pemeriksaan penunjang dalam menegakan diagnosis, dan keterbatasan alat-alat dalam mengatasi disfagia seperti oesofagoskopi.
Mekanisme fisiologis menelanMenelan adalah kemampuan untuk membawa suatu bolus makanan (keras, cair, gas atau bentuk campuran) dari mulut ke lambung, menjaga makanan dan cairan melewati laring, serta kombinasi fungsi yang menghentikan makanan dan cairan masuk kelaring. Ini merupakan proses yang komplek yang memerlukan koordinasi lebih dari 40 pasang otot baik involunter dan volunter serta beberapa saraf kranial.Pada menelan ada 4 fase yaitu fase persiapan oral, fase oral, fase faringeal dan fase esofageal.1. Fase persiapan oralPada fase ini mulut dipersiapkan untuk menerima makanan dan memulai proses makanan. Struktur yang terlibat meliputi bibir, gigi dan geligi, dan bagian depan lidah. Secara tidak langsung kerja ini diperantarai oleh tangan ke mulut dengan menyiapkan mulut untuk menerima makanan. Sekali diterima, bibir akan menutup makanan dikunyah jika diperlukan lidah mempersiapkan makanan ke bolus yang kohesif untuk ditransport. Mekanisme ini melibatkan penutupan bibir, gerakan memutar dan kesamping kiri kanan gigi dan lidah dan menggelembungnya palatum mole anterior untuk mencegah makanan masuk secara premnatur ke faring. Fase persiapan ini di bawah kendali volunter dengan melibatkan saraf kranial V, VII, X dan XII.2. Fase oralPada fase ini , dimana lidah yang dipeersarafi oleh saraf XII memposisikan diri digaris tengah kemudian menjadi elevasi dan menekan bolus makanan ke arah palatum durumg. Gerakan ini memberi sinyal reseptor-reseptor dipilar anterior tonsil, palatum mole, dan orofaring untuk memulai reflek fase esofageal dan memberikan makanan atau cairan dari cavum oral. Elevasi dari palatum mole pada fase ini akan menutup nasofaring akibat kontraksi m. Levator velli palatini. Selanjutnya terjadi kontraksi m palatoglosus yang menyebabkan istmus fausium tertutup, diikuti kontraksi m palatofaring sehingga mencegah regurgitasi.3. Fase faringealPada fase ini, laring akan menutup untuk melindungi jalan nafas secara optimal. Komplek urutan ini dimulai pada tingkat plika vokalis asli dan berlanjut pada tingkat plika vokalis palsu, plika arieepiglotik dan epiglotis. Saat yang kritis adalah saat penutupan laring pada tingkat glotis. Jika terjadi penutupan pilka vokalis, kartilago aritenoid naik dan miring ke arah posterior dan dasar lidah bergerak kearah posterior untuk menutup vestibula laring. Penutupan plika vokalis mencegah aspirasi atau masuknya makanan atau cairan kedalam trakhea, dibawah tingkat plika vokalis asli. Secara simultan epiglotis akan menutup dan melindungi jalan nafas. Gerakan eipglotis terjadi oleh karena tekanan bolus makanan, kekuatan otot menekan ke bawah dan tekanan dasar lidah sebelumnya yang bergerak ke posterior dan meningginya laring. Penutupan epiglotis penting untuk proses menelan yang aman dan mencegah masuknya makanan ke dalam vestibulum laring. Seiring dengan gerakan peristalti otot, peristaltik faring memerlukan, gerak lidah dan laring untuk membentuk tekanan dalam laring selama menelan. Retraksi lidah dan laring bawah pada akhir menelan meningkatkan tekanan pada hipofaring. Bolus kemudia didorong melalui sfingter esofageal atas (UES) oleh kekuatan dorongan laring dan mulailah fase esofageal yang merupakan fase involunter.4. Fase esofagealPada fase ini terjadi fase involunter yaitu fase perpindahan bolus makanan dari esofagus ke lambung. Dalam keadaan istirahat introiutus esofagus selalu tertutup. Dengan adanya rangsangan dari bolus makanan pada akhir fase faringeal, maka terjadi relaksasi muskulus krikofaring, sehingga introiutus esofagus terbuka dan bolus makanan masuk ke dalam lambung. Setelah bolus makanan lewat, maka sfingter akan berkontraksi lebih kuat, melebihi tonus introitus esofagus pada waktu istirahat, sehingga makanan tidak akan kembali ke faring sehingga refluks dapat dicegah.Gerak bolus makanan di esofagus bagian atas masih dipengaruhi oleh kontraksi m konstriktor faring inferior pada akhir fase faringeal. Selanjutnya bolus makanan akan didorong ke distal oleh gerakan peristaltik esofagus.Dalam keadaan istirhat sfingter bagian bawah selalu tertutup dengan tekanan rata-rata 8 mmHg lebih dari tekanan di dalam lambung sehingga tidak akan terjadi regurgiutasi isi lambung. Pada akhir fase esofagus sfingter ini akan terbuka secara refleks ketika dimulainya peristaltik esofagus servikal untuk mendorong bolus makanan ke distal selanjutnya setelah bolus lewat, maka sfingter akan menutup kembali.AchalasiaAchalasia untuk pertama kali dideteksi lebih dari 300 tahun yang lalu. Saat pertama kali, achalasia dikenal dengan cardiospasm karena dokter berpendapat hal ini ada kaitannya dengan blokade pada cardiac sphincter (LES) dari eosofagus. Pada pertengahan abad 20 baru mulai dikenal dengan sebutan achalasia. Secara khusus kelainan ini ditandai oleh adanya kegagalan untuk relaksasi dan pada kenyataanya pada LES di eosofagus tidak mampu untuk relaksasi.
Definisi menurut Dr. Arnon Lambroza adalah sebagai berikut : Achalasia is an esophageal motility disorder, which is characterized by delayed food passage through the esophagus. Patients with achalasia feel that food gets stuck in their throat or chest and may experience severe regurgitation and weight loss. With achalasia, the esophagus loses its ability to contract in a sequential manner and the lower esophageal sphincter fails to open completely, thereby slowing food transit into the stomach.
Dengan kata lain, ada dua masalah utama yang menyebabkan gejala dari achalasia adalah :1. Esofagus tidak mampu meneruskan makanan dari tenggorokan ke dalam perut.2. Sphincter atau katup antara esofagus dan stomach tidak mengalami relaksasi saat proses menelan.
Akibatnya makanan tidak hanya bergerak secara lambat saat turun dari tenggorokan, tetapi tidak dapat masuk ke dalam stomach, sehingga makanan tertahan di esofagus. Banyak faktor yang dicurigai dapat menyebabkan kelainan achalasia, diantaranya adalah :1. Herpes zoster, yang dikenal dengan shingles2. Infeksi3. Faktor herediter4. Kanker5. Kelaianan autoimmuneAchalasia bisa terjadi baik pada laki-laki maupun perempuan dengan resiko yang sama, pada semua umur tetapi lebih sering pada umur dewasa antara 25 60 tahun.Kesukaran menelan makanan baik padat dan cair pada kasus achalasia sering merupakan gejala utama, dan gejala ini sendiri sering disebut dengan istilah dysfagia. Pada awalnya gejala ini tidak berat dan tidak terus menerus terjadi, tetapi akan berkembang menjadi berat dan bertambah berat seiring bertambahnya waktu. Banyak pasien menggambarkan dysfagia sebagai perasaan penuh di tenggorokan. Gejala lain yang sering dirasakan pada pasien achalasia adalah :1. Chest pain, nyeri ini akibat spasmus dan akan terasa lebih berat saat habis makan, nyeri ini berbeda dengan angina, pada chest pain akibat jantung biasanya akan bertambah berat saat aktifitas.2. Regurgitasi, hal ini terjadi ketika setelah makan baik padat atau cair kembali ke atas, atau saat berbaring. Keluhan ini sering dirasakan malam hari pada saat pasien tidur, sehingga dapat menimbulkan aspirasi pneumonia.3. Heartburn, keluhan ini bukan disebabkan oleh adanya asam lambung dari stomach (seperti GERD) tetapi akibat asam laktat yang berasal dari proses penghancuran makanan di oesofagus.4. Penurunan berat badan, sebagaian besar pasien achalasia mengalami penurunan berat badan, tetapi tidak terlalu berat. Pasien achalasia dengan dysfagia saat makan sering diatasi dengan cara minum banyak ketika makan (utamanya dalam stadium awal) atau kadang pasien mencoba mengangakat lenganya ke atas melebihi kepalanya, berdiri dan berlomat-lompat agar makanan turun ke bawah. Beberapa pasien mencoba minum minuman yang mengandung carbonat.
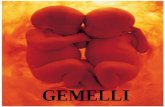
Pathofisiologi achalasiaEsophageal Motility AbnormalitiesLebih dari 75 tahun, Goldblums group melaporkan hilangnya sel ganglion myenteric sebanyak 64 % dan berkurangnya marker (36 %) pada 42 kasus dengan achalasia yang telah dilakukan esofagektomi. Pada penelitian yang sama juga dilaporkan adanya sel T pada proses inflamasi dari plexus myenteric dengan adanya fibrosis. Pada biopsi pasien achalasia didapatkan adanya gambaran sel ganglion berkurang, dan dapat sampai tidak dijumpainya ganglion dan fibrosis. Pada gambar 6 didapatkan adanya derajad inflamasi ganglion dan aganglionosis.gambar 6 : histopatologi achalasia
a. plexus myenteric normal ditandai adanya gambaran sel ganglion multipel dan infiltrasi lymposit minimal.b. inflammation myenteric ringan. Inflamasi limposit ringan dan sel ganglion masih dapat diidentifikasi. c. inflamasi myenteric sedang adanya infiltrasi limposit dan tidak dijumpai adanya gambaran sel ganglion . d. inflamasi myenteric berat ditandai adanya sel limposit berkelompok dengan plexus myenteric. Sel ganglion hilang. (Source: Hirano and Kahrilas112 with permission from Blackwell Publishing.)Dari pemeriksaan histopatologi otot halus dari esofagus pasien achalasia didapatkan adanya gambaran yang tidak normal, Goldblum menggambarkan adanya hypertropi sama dengan proses degenerasi dari muskulus propria dan mukosa pada 42 kasus yang telah mengalami reseksi. Dengan menggunakan USG frekuensi tinggi, mittal et al. Menunjukan markernya meniingkat pada kedua lapisan dinding otot. Peningkatan ini juga dijumpai pada pasien dengan atau tanpa dilatasi esofageal. Mekanisme adanya proses hypertropi ini kurang begitu jelas. Obstruksi esofageal mungkin akan menyebabkan terjadinya hypertropi muskulus sekunder pada binatang percobaan. Sebagai tambahan adanya defisiensi nitric oxida pada pasien achalasia juga dijumpai. Nitric oxide mempunyai fungsi menghambat dari proliferasi muskulus halus dan hypertropi otot halus fisera. Menarikny lagi, 52 % dari 42 spesimen dari reseksi esofageal dijumpai adanya eosinophilia pada muskulus propria. Tottrup et al. Melaporkan adanya peningkatan ekspresi eosinophilic cationic protein , akibat aktifasi eosinopihl pada achalasia. Meskipun eosinopihl tidak menunjukan kontrol terhadap esofagus, tidak ada hubungan antara eosinopil esofagitis dan achalasia. Pada eosinopillic esofagitis ditandai adanya infiltrasi eosinophil pada mukosa squamous, meskipun infiltrasi eosinopihl pada muskulus propria juga dapat dijumpai. Integrity of Cholinergic InnervationA number of physiologic studies have uncovered an intact cholinergic innervation to the esophagus in achalasia. An in vitro study by Trounce et al.23 in 1957 demonstrated contractions of muscle strips from achalasia patients to the combination of the acetylcholinesterase inhibitor, eserine, and the ganglionic agonist, nicotine. Intact acetylcholinesterase activity of preserved ganglion cells in the lower segment of the esophagus of achalasia patients was described by Adams24 in 1961. The acetylcholinesterase inhibitor edrophonium chloride was later shown to significantly increase the LES pressures in patients with achalasia.25 These findings suggest that at least some postganglionic, cholinergic nerve endings remain intact. Further evidence in this regard came from a study looking at the effects of the anticholinergic agent atropine in patients with achalasia.26 This study demonstrated a 30% to 60% reduction in LES pressure with atropine in patients with achalasia. A similar reduction was found in a control group of healthy volunteers. Of note, however, is the fact that the residual pressure after atropine was significantly higher in the achalasia patients (17 mmHg) than in the normal subjects (5 mmHg).Recently, botulinum toxin has been introduced as a novel treatment for achalasia. Botulinum toxin acts to inhibit the exocytosis of acetylcholine from cholinergic nerve endings. Most studies using botulinum toxin have found a significant symptomatic response rate. However, objective measures of response including LES pressure and esophageal emptying were modest and in some studies not significantly different from baseline values.27, 28 Similar to the studies using atropine, a significant residual LES pressure was observed following botulinum toxin, 25 mmHg in a study by Pasricha et al.28 and 20 mmHg in a study by Cuilliere et al.29 Therefore, the studies using atropine and botulinum toxin both support the concept of preservation of cholinergic nerves in patients with achalasia. Furthermore, they have provided evidence for a significant, noncholinergic component to LES basal pressure. It is likely that this residual pressure represents the myogenic contribution to LES tone. Heterogeneity in the response to botulinum toxin suggests a variable degree of cholinergic preservation of individual achalasia patients.Loss of Inhibitory InnervationPreservation of the excitatory, cholinergic innervation to the esophagus implies that the neuronal loss that characterizes achalasia may be selective for inhibitory neurons. Dodds et al.30 provided indirect evidence for this through the use of cholecystokinin, which has direct excitatory effects on smooth muscle as well as indirect inhibitory effects via postganglionic inhibitory neurons. In patients with achalasia, cholecystokinin induced LES contraction as opposed to the relaxation of the LES seen in control subjects, thereby providing evidence for impaired postganglionic inhibitory nerves. More recent evidence comes from in vitro studies looking at the responses of preparations of LES specimens from patients with achalasia. Circular muscles strips of the LES from normal subjects characteristically relax in response to electrical field stimulation through the activation of nitric oxide containing inhibitory neurons.31, 32 Paradoxically, LES strips from achalasia patients were found to contract in response to electrical field stimulation (Figure 7).31 Such findings can be readily explained by the absence of inhibitory neurons and presence of excitatory neurons.Figure 7:In vitro study demonstrating the effects of electrical field stimulation (EFS) on circular muscle strips from the LES of control subjects (a) and patients with achalasia (b).
Electrical field stimulation activates enteric neurons, which results in relaxation of the LES that is unaffected by atropine (Atr) but abolished by tetrodotoxin (TTX). In the LES from an achalasia patient, ERS results in paradoxical contraction that is sensitive to both Atr and TTX. This experiment provides evidence for the loss of intrinsic inhibitory innervation with preservation of cholinergic excitatory innervation in achalasia. (Source: Tottrup et al.31 with permission from the BMJ Publishing Group.) Full size image (12 KB) Download Power Point slide (287 KB)
Evidence to support the concept of inhibitory neuronal loss came from both immunohistochemical and physiologic studies. Early studies postulated a defect in the adrenergic, inhibitory innervation of the esophagus.24 Vasoactive intestinal polypeptide (VIP) was also considered a candidate inhibitory neurotransmitter of the esophagus, and a reduction in VIP-containing neurons was demonstrated in achalasia patients.33, 34, 35 Following the discovery of nitric oxide, a number of studies have demonstrated the absence of nitric oxide synthasecontaining neurons in LES specimens from patients with achalasia.6, 36, 37 Furthermore, recent experimental studies have shown that selective blockade of the inhibitory arm of the enteric innervation of the esophagus produces a manometric picture that closely mimics that of achalasia. Studies in both experimental animals and human subjects have shown that inhibition of nitric oxide synthase increases the resting tone of the LES and nearly abolishes LES relaxation (Figure 8a).32, 38, 39, 40 In the esophageal body, inhibition of nitric oxide synthase results in loss of the normal latency gradient manifest as simultaneous esophageal body contractions (Figure 8b). In healthy subjects, intravenously administered, recombinant hemoglobin, which inactivates nitric oxide, has been shown to produce simultaneous esophageal body contractions and failed LES relaxation (Figure 9).39 This motility pattern mimics the motility pattern of the vigorous form of achalasia (Figure 4). It lends credence to the model of achalasia that incorporates the selective loss of inhibitory and preservation of cholinergic enteric neural function (Figure 10b).Figure 8:a: Effect of nitro-L-arginine methyl ester (L-NAME) on LES relaxation in the opossum in vivo.
Control esophageal manometry illustrates an esophageal body peristaltic contraction and LES relaxation in two separate recording channels. Following the intravenous administration of L-NAME, a selective inhibitor of nitric oxide synthase, the latency prior to the esophageal contraction is shortened, basal LES pressure increased and LES relaxation is abolished. L-arginine, an antagonist of L-NAME, reverses the effects of L-NAME. (Source: Yamato et al.32 with permission from Elsevier.) b: Effect of L-NAME on esophageal peristalsis in the opossum in vivo. Control esophageal manometry (A) demonstrates an esophageal body peristaltic sequence with increasing latency period before each contraction that characterizes peristalsis. In the second sequence (B), the animal has been pretreated with L-NAME, a selective inhibitor of nitric oxide synthase, resulting in a loss of the latency gradient and hence simultaneous esophageal body contractions. Finally in the third panel (C), the animal was pretreated with both L-NAME and atropine (Atr), an antimuscarinic agent, resulting in simultaneous and low-amplitude esophageal contractions. Full size image (65 KB) Download Power Point slide (495 KB)
Figure 9:Effect of recombinant hemoglobin that inactivates nitric oxide on esophageal peristalsis in a human subject.
Control manometry (a) reveals a sequential peristaltic wave and normal LES relaxation in response to a swallow. Following an infusion of hemoglobin (b), deglutition produces simultaneous esophageal contraction and absent LES relaxation, mimicking the manometric profile of achalasia. (Source: Murray et al.39 with permission from American Gastroenterological Association.) Full size image (54 KB) Download Power Point slide (477 KB)
Figure 10:Pathophysiology of idiopathic achalasia.
Left: The normal condition where excitatory, cholinergic (Ach) motor neurons innervate the smooth muscle cells of the LES and contribute to the genesis of basal pressure of the LES (LESP). Inhibitory, nitric oxide (NO) motor neurons also act on the LES to produce the relaxation that accompanies a swallow. Middle: Achalasia resulting from the loss of inhibitory neurons. In this situation, the absence of NO motor neurons results in an elevation in the basal LESP and absence of swallow induced relaxation of the LES. Esophageal aperistalsis is defined by simultaneous esophageal body contractions. Right: Achalasia with complete loss of myenteric neurons. Here the basal LESP is below normal owing to the absent excitatory neurons, and swallow-induced relaxation is absent owing to the lack of inhibitory neurons. Esophageal aperistalsis is defined by the absence of esophageal body contractions. (Source: Hiranoand Kahrilas112 with permission from Blackwell Publishing.) Full size image (39 KB) Download Power Point slide (666 KB)
Pathologic studies that have examined esophageal resection specimens from achalasia patients undergoing esophagectomy likely select patients with long-standing or end-stage disease. The complete aganglionosis demonstrated in the majority of such patients may represent an end result of ongoing myenteric inflammation. Such descriptions support a second model of achalasia in which both the excitatory, cholinergic neurons and inhibitory, nitric oxide neurons are absent (Figure 10c). Under such circumstances, the functional obstruction of the gastroesophageal junction is caused by the residual myogenic tone of the LES. Complete absence of esophageal peristaltic activity is the result of the absent enteric neural innervation.Although the nitric oxidecontaining neurons may be lost in achalasia, the intracellular pathways by which nitric oxide acts remain intact in achalasia. This is evidenced by the efficacy of exogenously administered nitrates that act as nitric oxide donors in the treatment of achalasia. Furthermore, a study by Bortolotti et al.41 demonstrated a significant decrease in LES pressure following administration of sildenafil (Viagra). Sildenafil is an inhibitor of phosphodiesterase type 5 that breaks down cyclic guanosine monophosphate stimulated by nitric oxide. The efficacy of sildenafil in achalasia supports the integrity of the nitric oxide second messenger system in the smooth muscle of the LES in achalasia.