Acei Dan Arb

of 8
-
Upload
fathnur-sani -
Category
Documents
-
view
217 -
download
0
Transcript of Acei Dan Arb
-
8/14/2019 Acei Dan Arb
1/8
Articles
2026 www.thelancet.com Vol 366 December 10, 2005
IntroductionNational and international guidelines endorse the viewthat inhibition of the renin-angiotensin system withangiotensin-converting-enzyme (ACE) inhibitors shouldbe first-line antihypertensive therapy in patients withdiabetic and non-diabetic nephropathy. In the UK, theRenal Association, British Diabetic Association, BritishHypertension Society, and National Institute of ClinicalExcellence all encourage use of these drugs as first-line
treatment to reduce proteinuria and retard theprogression of renal disease.14 The recommendation indiabetes has been formalised in the new GeneralMedical Services Contract for primary care in the UK,with remuneration linked to the prescription of thesedrugs for this indication.4 Similar advice is included inother European and US guidelines, which advocate thateither ACE inhibitors or angiotensin-II receptor blockers(ARB) be used to delay the progression of renal disease.5,6
Implicit in this advice is the assumption that inhibitionof the renin-angiotensin system with ACE inhibitors(and, more recently, ARBs) has specific renoprotectiveeffects beyond those resulting from lowering blood
pressure alone.
79
Blood-pressure-independent effects ofACE inhibitors on cardiovascular outcomes have also
been proposed, based on the results of several largemulticentre trials, especially the HOPE, PROGRESS, andEUROPA studies,1012 and similar claims have been madefor ARBs.13 However, these placebo-controlled trials havebeen difficult to interpret because use of the active drugreduced blood pressure compared with the control group.The log-linear association between blood pressure andthe incidence of cardiovascular events14 means that areduction in systolic blood pressure of as little as
5 mm Hg reduces the incidence of stroke by about 40%and myocardial infarction by 20%.15 The reduction in theoccurrence of cardiovascular endpoints seen in placebo-controlled trials of ACE inhibitors or ARBs is in the rangeexpected from the blood-pressure-lowering effect,arguing against pleiotropic effects of inhibition ofthe renin-angiotensin system on cardiovascularendpoints.2,15,16 Indeed, when the cardiovascular effects inpatients randomly assigned ACE inhibitors were assessedin trials with an active comparator rather than placebo, noparticular advantage of ACE inhibitors was seen overother classes of blood-pressure-lowering drugs.15
Blood pressure is also an important risk factor for the
progression of renal disease.
1719
However, the guidelinesthat advocate use of ACE inhibitors and ARBs in renal
Lancet 2005; 366: 202633
Centre for Clinical
Pharmacology, Department of
Medicine, BHF laboratories at
University College London,
London, UK(J P Casas MD,
W Chua BSc,
S LoukogeorgakisBSc,ProfP Vallance FMedSci,
A D Hingorani FRCP,
R J MacAllister FRCP); and
Department of Epidemiology
and Population Health, London
School of Hygiene & Tropical
Medicine, London, UK
(J P Casas, L Smeeth MRCGP)
Correspondence to:
Dr Juan P Casas, Centre for
Clinical Pharmacology,
Department of Medicine, BHF
Laboratories, University College
London, London WC1E 6JF, UK
Effect of inhibitors of the renin-angiotensin system and
other antihypertensive drugs on renal outcomes:systematic review and meta-analysis
Juan P Casas, Weiliang Chua,Stavros Loukogeorgakis, Patrick Vallance,Liam Smeeth, Aroon D Hingorani, Raymond J MacAllister
SummaryBackground A consensus has emerged that angiotensin-converting-enzyme (ACE) inhibitors and angiotensin-IIreceptor blockers (ARBs) have specific renoprotective effects. Guidelines specify that these are the drugs of choice forthe treatment of hypertension in patients with renal disease. We sought to determine to what extent this consensusis supported by the available evidence.
Methods Electronic databases were searched up to January, 2005, for randomised trials assessing antihypertensive
drugs and progression of renal disease. Effects on primary discrete endpoints (doubling of creatinine and end-stagerenal disease) and secondary continuous markers of renal outcomes (creatinine, albuminuria, and glomerularfiltration rate) were calculated with random-effect models. The effects of ACE inhibitors or ARBs in placebo-controlled trials were compared with the effects seen in trials that used an active comparator drug.
Findings Comparisons of ACE inhibitors or ARBs with other antihypertensive drugs yielded a relative risk of 071(95% CI 049104) for doubling of creatinine and a small benefit on end-stage renal disease (relative risk 087,075099). Analyses of the results by study size showed a smaller benefit in large studies. In patients with diabeticnephropathy, no benefit was seen in comparative trials of ACE inhibitors or ARBs on the doubling of creatinine(109, 055215), end-stage renal disease (089, 074107), glomerular filtration rate, or creatinine amounts.Placebo-controlled trials of ACE inhibitors or ARBs showed greater benefits than comparative trials on all renaloutcomes, but were accompanied by substantial reductions in blood pressure in favour of ACE inhibitors or ARBs.
Interpretation The benefits of ACE inhibitors or ARBs on renal outcomes in placebo-controlled trials probably resultfrom a blood-pressure-lowering effect. In patients with diabetes, additional renoprotective actions of thesesubstances beyond lowering blood pressure remain unproven, and there is uncertainty about the greaterrenoprotection seen in non-diabetic renal disease.
-
8/14/2019 Acei Dan Arb
2/8
Articles
www.thelancet.com Vol 366 December 10, 2005 2027
disease base their recommendations largely on the
results of placebo-controlled trials, often using surrogatemarkers rather than clinically relevant endpoints.2022 Toassess blood-pressure-independent renoprotection dueto inhibition of the renin-angiotensin system, weundertook a systematic review and meta-analysis ofrandomised controlled trials investigating the effect ofdifferent classes of antihypertensive drugs onprogression of renal disease. In particular, we comparedthe effects on renal outcomes of inhibition of the renin-angiotensin system in trials using placebo controlsversus trials with active comparator drugs.
MethodsThree electronic databases (MEDLINE, EMBASE, and
the Cochrane Library) were searched from 1960 toJan 31, 2005, for randomised controlled trialsinvestigating any antihypertensive drug and progressionof human renal disease, with MeSH headings and textwords (discussed in detail in search strategies,webappendix). We searched for any additional studies inthe references of all identified publications, includingprevious relevant meta-analyses and narrative reviews.
Selection criteriaFor inclusion, studies had to be randomised, controlled,parallel-design in adults, and examine the effect of anydrug treatment with a blood-pressure-lowering action on
progression of renal disease. Progression of renaldisease was assessed by use of incident renal endpointsas primary outcomes (doubling of serum creatinine andend-stage renal disease, defined as the need for kidneytransplantation or haemodialysis) and secondarycontinuous markers (glomerular filtration rate [GFR],serum creatinine, and urine albumin excretion). Studieshad to have a minimum follow-up of 1 year. Only studiespublished as full-length articles or letters in peer-reviewed English-language journals were included.
Data extractionThe following information was extracted and entered intodatabases by three investigators (JPC, WCH, RJM): study
design, type of intervention, patients characteristics, andoutcomes (webappendix). If relevant informationregarding design, or renal outcomes was unavailable, ordoubt existed about duplicate publications, authors werecontacted to obtain the necessary information(webappendix). Uncertainties were resolved by consensus.
Statistical analysisWe compared effects of inhibition of the renin-angiotensin system, by use of ACE inhibitors or ARBs,on renal outcomes in trials that used placebo as acomparator with trials that used other antihypertensivedrugs ( blockers, diuretics, calcium-channel blockers, blockers, or combinations of these) as comparators.The trial arm with ACE-inhibitor or ARB medication was
assigned as the experimental group. We used
metaregression models to measure to what extent thedifference in blood-pressure change (expressed as atertile of blood-pressure reduction) between randomisedgroups accounted for the observed difference in renaloutcomes. All trials with ACE-inhibitor or ARBtreatment were included for these analyses. We excludedtrials that did not provide information on achieved bloodpressure from our metaregression models.
For continuous variables (blood pressure, serumcreatinine, GFR, and urine albumin excretion) resultswere expressed as the mean difference in the change inthe variable between randomised groups. Thisdifference was calculated by subtraction of the meanchange in the variable in the reference group (follow-up
value minus baseline value; -reference) from thecorresponding mean change in the experimental group(follow-up value minus baseline value; -experimental)by use of random-effect models.
For binary renal outcomes (the doubling of serumcreatinine and occurrence of end-stage renal disease), thepooled relative risk (RR) and 95% CIs were calculatedwith random-effect models by the method ofDerSimonian and Laird.23 The DerSimonian and LairdQ test was used to assess the degree of heterogeneitybetween studies, and I2 was used as a measure to describethe percentage of variability in point estimates that wasdue to heterogeneity rather than sampling error.23 To
assess the robustness of the findings, sensitivity analyseswere done according to study-level characteristics, suchas disease status (type 1 or 2 diabetes vs no diabetes), andstudy size (n500 vs n500).Funnel plots and the Eggerregression asymmetry test were used to investigate small-study bias (eg, publication bias). Data were analysed withStata 8.2. The webappendix provides further details aboutthe statistical analysis.2426
Role of the funding sourceNo funding source had any role in study design, datacollection, data analysis, data interpretation, or writingof the report. All authors had full access to all the data inthe study and all took full responsibility for the decision
to submit for publication.
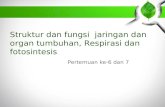
ResultsFigure 1 summarises the identification process foreligible clinical trials. We found 127 eligible studiescorresponding to 150 group comparisons with aweighted mean follow-up of 42 years. 99 groupcomparisons used trials including only patients withdiabetes (weighted mean GFR 845 mL/min),36 included only patients without diabetes(734 mL/min), ten included both types of patient(750 mL/min), and five did not report information onthe presence of diabetes (96 mL/min). The study samplesize was 100 or less patients in 98 comparisons (weightedmean follow-up 25 years), between 100 and 500 patients
See Lancet Online for
webappendix
-
8/14/2019 Acei Dan Arb
3/8
Articles
2028 www.thelancet.com Vol 366 December 10, 2005
in 34 comparisons (28 years), and 500 or more patientsin 18 comparisons (45 years). The table shows the maincharacteristics of studies included in our analysis.
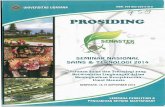
13 trials (n=37 089) were included that compared theeffect of ACE inhibitors or ARBs on the occurrence ofend-stage renal disease with the effect of otherantihypertensives. In these trials, a small reduction wasseen in the risk of end-stage renal disease in favour of
either ACE inhibitors or ARBs (p=004; figure 2, A) withno differences in the degree of change of systolic(132 mm Hg, 95% CI 403 to 138) or diastolic
(058 mm Hg, 22 to 104) blood pressure between
the groups. We did not record any interstudyheterogeneity (p=048, I2=0%). The Egger test suggestedno evidence of small-study bias (p=023), although thisfactor is discussed in more detail later. No significantbenefit of ACE inhibitors or ARBs over otherantihypertensive drugs was seen in patients withdiabetes (four trials, n=14 437; figure 2, A).
11 trials (n=3376) were included that compared theeffect of ACE inhibitors or ARBs with active comparatorson the doubling of creatinine. We saw a non-significantreduction in the risk of doubling of creatinine in favour ofeither ACE inhibitors or ARBs (p=007; figure 2, B). Therewere no differences in the degree of change of systolic(097 mm Hg, 309 to 114) or diastolic (023 mm Hg,
099 to 146) blood pressure between randomisedgroups. As with the comparison on occurrence of end-stage renal disease, we recorded no significant interstudyheterogeneity (p=026, I2=0%) or small-study bias(p=066). In patients with diabetes (six trials, n=3044),ACE inhibitors or ARBs showed no benefit compared withother antihypertensive drugs (RR 109, 055215).
We included 38 trials (n=5711) that compared theeffect of ACE inhibitors or ARBs on serum creatinineconcentration with that of other antihypertensives. ACE-inhibitor or ARB treatment led to a small reduction increatinine concentration (p=001; figure 3, A) and in thedegree of change of systolic blood pressure
(149 mm Hg, 292 to 005), but not diastolic bloodpressure (059 mm Hg, 155 to 037). Some small-study bias (p=007) and interstudy heterogeneity(p00001, I2=663%) was indicated. In patients withdiabetes, no benefit on creatinine was seen (figure 3, A).
44 trials (n=5266) in our analysis compared the effect ofACE inhibitors or ARBs on urine albumin excretion withother antihypertensive drugs (figure 3, B). ACE-inhibitoror ARB treatment resulted in a small reduction in dailyurinary albumin excretion (p=0001). There were nodifferences between groups in the degree of change ofsystolic (095 mm Hg, 251 to 061) or diastolic(008 mm Hg, 103 to 087) blood pressure. However,we recorded substantial evidence of small-study bias
(p=0001) and significant study heterogeneity (p00001,I2=578%). In patients with diabetes, a small reduction indaily urine albumin excretion was seen (figure 3, B).
Database search:
MEDLINE/PubMed (n=943)
Cochrane Library (n=2043)
EMBASE (n=1471)
150 group comparisons by diabetes status:
99 with only patients with diabetes
36 with only patients without diabetes
10 with mixed diabetes status
5 with unknown diabetes status
4160 studies excluded:
Reasons include: search overlap, no randomisation,
no antihypertensive drug intervention, no renal
outcomes, no adult patients, follow-up less than
1 year, only patients with ESRD included
Group comparisons by interventions assessed:
48 with ACE inhibitors or ARBs vsplacebo
11 with other active interventions vsplacebo
77 with ACE inhibitors or ARBs vsother active
interventions
5 with ACE inhibitors vsARBs or ACE inhibitors 9 with other active interventions vsother
active interventions
297 studies retrieved for full paper review
127 studies included in meta-analysis
170 studies excluded:
Reasons include: no randomisation, no renal
outcomes, ad-hoc analysis of same trial, trial design
reporting, cost study, non-adult patients, follow-up
less than 1 year, only patients with ESRD included
Number of group Mean (range) Mean proportion Proportion of studies Mean (range) Mean (range) Mean (range)
comparisons sample size of patients w it h onl y including baseline G FR base line baseline
(number of hypertension patients with (mL/min) creatinine albuminuria
patients) (range) diabetes (%) (mol/L) (mg/day)
Group comparisons
All 150 (73 514) 490 (1133 357) 649 (0100) 73% 869 (1581842) 1131 (68389) 6028 (723100)
ACE inhibitors or ARBs vs placebo 48 (16 588) 345 (114912) 326 (0100) 89% 978 (1581842) 1105 (698389) 5355 (731900)
ACE inhibitors or ARBs vs other active interventions 77 (43 439) 564 (1333 357) 857 (0100) 62% 774 (188150) 1270 (683492) 5195 (723000)
ACE inhibitors vs ARBs 5 (594) 118 (24250) 75 (0100) 60% 803 (384967) 1573 (7072652) 926 (92102)
Other active interventions vs placebo 11 (6390) 581 (124406) 40 (0100) 89% 995 (641129) 984 (7861494) 11287 (731900)
Other active interventions vs other active interventions 9 (6503) 722 (206125) 100 (0100) 75% 761 (55898) 1414 (1202152) 9505 (553100)
Table: Characteristics of studies in meta-analysis
Figure 1: Identification process for eligible randomised controlled trials
-
8/14/2019 Acei Dan Arb
4/8
Articles
www.thelancet.com Vol 366 December 10, 2005 2029
61 trials (n=39 485) were included that compared the
effect of ACE inhibitors or ARBs with otherantihypertensive drugs on the GFR. Compared withother drugs, ACE-inhibitor or ARB treatment had noeffect on the GFR (figure 3, C) or on the degree ofchange of systolic (016 mm Hg, 122 to 09) ordiastolic (011 mm Hg, 05 to 072) blood pressure.We recorded no significant interstudy heterogeneity(p=094, I2=0%) or small-study bias (p=088). The GFRdid not improve in patients with diabetes (figure 3, C).
For the primary outcomes (end-stage renal disease anddoubling of creatinine), no significant evidence of small-study bias was seen, but data were based on smallnumbers of trials (end-stage renal disease, 13 trials,p=023; doubling of creatinine, 11, p=066). For thesecondary continuous outcomes, more trials had outcome
data available, and with significant small-study bias for
creatinine (38, p=007) and urine albumin excretion (44,p=0001). For the occurrence of end-stage renal disease,analysis according to study size (500, 500 to 1500, and1500 patients), showed that the apparent beneficial effectof ACE inhibitors or ARBs over other antihypertensivedrugs falls as study size increases (figure 2, A), and thep value for a metaregression according to study size was0013. However, the trend was greatly affected byALLHAT,27 which provided almost half the events of end-stage renal disease and showed no beneficial effect. Fordoubling of creatinine, analysis by study size also indicatedno benefit of ACE inhibitors or ARBs compared with otherantihypertensive substances in large studies (figure 2, B).
In trials with the comparator arm as placebo ratherthan another antihypertensive drug, patients randomly
RR of end-stage renal disease
ACE inhibitors or ARBs vsother active interventions
05 10 15
068 (048096)Studies with less than 500 patients (n=9) 45/596 63/579
076 (061095)Studies with 500 or more patients (n=3) 133/1415 140/1142
080 (059108)S tu di es o nl y in cl udi ng p at ie nts witho ut d iabe tes ( n=8 ) 1 30 /6 58 4 2 03 /1 5 95 8
089 (074107)Studies only including pat ient s w ith dia betes (n=4) 160/ 4426 305 /10 011
Favours ACE inhibitors or ARBs Favours other
active interventions
105 (086129)ALLHAT27 126/9054 322/24303
087 (075099)All studies (n=13) 304/11065 525/26024
RR (95% CI)Intervention
n/N
Control
n/N
RR of doubling of serum creatinine
ACE inhibitors or ARBs vsother active interventions
055 (030099)Studies with less than 500 patients (n=8) 22/425 37/443
097 (049192)Studies with 500 or more patients (n=3) 112/1280 152/1228
109 (055215)
Studies only including pat ient s w ithout dia betes (n=3) 10/ 120 15/1 02
Studies only including pat ient s w ith dia betes (n=6) 120/ 1530 161 /151 4
Favours ACE inhibitors or ARBs Favours other
active interventions
051 (024110)
071 (049104)All studies (n=11) 134/1705 189/1671
RR (95% CI)Intervention
n/N
A
B Control
n/N
03 05 10 15
Figure 2: Effect of ACE inhibitors or ARBs compared with other active interventions on relative risk of (A) end-stage renal disease, and (B) doubling of serum creatinine
Studies included are: (RR of end-stage renal disease) webreferences 2, 26, 27, 37, 44, 47, 56 , 67, 89, 118, 120, 126, and 127; (doubling of serum creatinine) webreferences 6, 8, 26 , 27, 56, 67, 89, 90,
95, 115, and 118 (webappendix).
-
8/14/2019 Acei Dan Arb
5/8
-
8/14/2019 Acei Dan Arb
6/8
Articles
www.thelancet.com Vol 366 December 10, 2005 2031
assigned to receive ACE inhibitors or ARBs were at lowerrisk of end-stage renal disease and doubling ofcreatinine, than was placebo (webtable 1), and alsoshowed reductions in serum creatinine and urinealbumin excretion (webtable 2). However, GFR was notaffected (122 mL/min, 095 to 339). These effectswere associated with the expected reduction in bloodpressure in the ACE-inhibitor or ARB groups (reductionsranging from 227 to 596 mm Hg; webtables 1 and2). Similar benefits were seen in patients with diabetes.We also recorded substantial evidence of small-study
bias in trials investigating the effect of ACE inhibitors orARBs on serum creatinine (p=007) and urine albuminexcretion (p=0006; webtable 2). In general, the benefitsof ACE inhibitors or ARBs over placebo were greater inthe small trials (webtables 1 and 2).
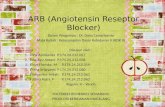
To assess the effect of the blood-pressure reduction onrenal outcomes, the difference in change in bloodpressure between randomised groups was calculated as acategorical variable by generation of tertiles of thedifference in change of systolic blood pressure. 20 placeboand head-to-head trials of ACE inhibitors or ARBs inwhich end-stage renal disease was a trial outcome wereincluded in the metaregression. The log odds ratio forend-stage renal disease increased by 013 (p=006) for aper-tertile increase of achieved blood pressure. Trials with
large blood pressure differences were associated with agreater reduction in the incidence of end-stage renaldisease than trials with small differences (figure 4, A). Theassociation of blood-pressure reduction with difference inchange in albuminuria in 55 trials was more substantial(for a per-tertile increase in achieved blood pressure, thedifference in change in albuminuria increased by3052 mg/day, p=002; figure 4, B).
DiscussionThis analysis confirms the importance of blood-pressure
control per se in the prevention of renal disease, in viewof the larger renoprotective effect of ACE inhibitors orARBs in placebo-controlled trials than in activecomparator studies. Indeed, when blood-pressuredifferences were reduced substantially by anti-hypertensive treatment in control groups, there was noevidence of a significant salutary effect of ACE inhibitorsor ARBs on renal outcomes in patients with diabetes. Bycontrast, small benefits of the drugs were seen in non-diabetic renal disease, although uncertainty remainsbecause of evidence of small-study bias. These findingshave implications for the use of ACE inhibitors or ARBsin patients with hypertension, diabetes, and renaldisease, and for the design of future studies toinvestigate renoprotection strategies.
See Lancet Online for
webtables 1 and 2
RR of end-stage renal disease in clinical trials usingACE inhibitors or ARBs vsother interventions
Other activeinterventions
(n/N)
Degree of change of systolicblood pressure
Mean difference (95% CI)
077 ( 067 to 089)16 mm Hg (28 to 04)
090 ( 072 to 112)15 mm Hg (01 to 29)
074 ( 059 to 092)69 mm Hg (91 to 48) 155/1291
356/6327
397/26 043
ACE inhibitors/ARB(n/N)
117/1346
273/6344
206/11 049
RR (95% CI)
06 10 1208
Difference of change in albuminuria (mg/day; -ACE
inhibitors or ARBsminus -other interventions) in clinical
trials using ACE inhibitors or ARBs vsother interventions
Mean difference in change (95% CI)
A
B
3273 (5190 to 1356)12 mm Hg (32 to 07)
181 (247 to 609)341 mm Hg (09 to 59)
8312 (12678 to 3946)76 mm Hg (98 to 55)
Number of studies
(number of patients)
23 (1668)
15 (1734)
17 (2312)
130 0 10
Favours ACE inhibitors
or ARBs
Favours other
interventions
50100
-
Figure 4: Stratified effect of ACE inhibitors or ARBs on (A) RR of end-stage renal disease and (B) urine albumin excretion, according to difference achieved in systolic blood pressure between
randomised groups
Data on these figures include information from placebo-controlled trials and trials with active interventions.
-
8/14/2019 Acei Dan Arb
7/8
Articles
2032 www.thelancet.com Vol 366 December 10, 2005
Trials with a placebo comparator indicated a
renoprotective effect of ACE inhibitors or ARBs, but thiseffect is most readily explained by their action to reduceblood pressure compared with placebo (with a differenceof between 23 to 60 mm Hg seen in these trials,webtables 1 and 2). Systemic blood pressure is a majordeterminant of the progression of renal disease,1719 andblood-pressure differences that are inevitable in placebo-controlled trials of ACE inhibitors or ARBs confoundinterpretation of effects on renal endpoints. Thisinterpretation was supported by the results of ourexploratory metaregression analysis, showing theimportance of lower blood pressure on end-stage renaldisease and urine albumin excretion (figure 4), and isconsistent with previous findings from overviews of
clinical trials examining effects of antihypertensive drugson cardiovascular outcomes.15,16 These conclusions wouldbe strengthened if metaregression could be used toinvestigate the renoprotective effects of antihypertensivedrugs other than ACE inhibitors and ARBs compared withplacebo. Although such a benefit has been suggested forcalcium-channel blockers,28 there were insufficient trialsof this type for us to undertake such an analysis reliably.
Comparator trials involving other antihypertensivedrugs provide the most specific data for therenoprotective effects of ACE inhibitors or ARBs. Thesefindings indicated that there was a small reduction in theincidence of end-stage renal disease (figure 2, A).
However, two uncertainties exist in the interpretation ofthese data. First, neither ACE inhibitors nor ARBsaffected GFR compared with other antihypertensivedrugs. Second, analysis of the treatment effect of ACEinhibitors or ARBs on end-stage renal disease anddoubling of creatinine according to study size showed areduced benefit in large studies (figure 2). Althoughstatistical tests for the primary outcomes for small-studybias were not significant, such tests have low power,especially when the number of trials is less than 20.29
The greater beneficial effect seen in the small studiescould indicate valid differences between the small andlarge studies. Renal function at entry in the very largeALLHAT trial was good compared with some of the
small studies that recruited a greater proportion ofpatients with poor renal function. However, when theALLHAT investigators stratified the data by degree ofrenal impairment, there was no evidence for a greaterbeneficial effect of ACE inhibitors in people with poorrenal function.27 In the ALLHAT trial, participantsassigned thiazide diuretics had a roughly 2 mm Hglower systolic blood pressure than those assigned ACEinhibitors, and this difference in blood pressure mighthave contributed to the absence of any beneficial effectof ACE inhibitors over thiazides on renal outcomes.However, another possible explanation for the gradientof effect seen in figure 2, A is small-study bias, for tworeasons: first, small negative studies are likely to haveremained unpublished, and second, those small studies
that have been published are likely to be of lower quality
than large trials, and more prone to bias.The discordance we show between the results of smalland large studies parallels that seen for intravenousmagnesium as a treatment for myocardial infarction. Ameta-analysis of small trials had suggested thatmagnesium treatment reduced mortality,30 yet the verylarge ISIS-4 trial showed no benefit of magnesium.31 TheISIS-4 finding was widely accepted as more valid thanthe previous meta-analysis,32 and it was subsequentlyshown that the misleading result from the meta-analysisof small studies of magnesium could be explained bypublication bias.33 It is possible, but by no means certain,that the small beneficial effect of ACE inhibitors or ARBson renal outcomes is similarly affected by publication or
other sources of small-study bias. It is notable that for thesecondary renal outcomes (serum creatinine and urinealbumin excretion) with sufficient numbers of trials,tests for small-study bias were highly significant.
In patients with diabetes, the results from the currentstudy emphasise the lack of a proven advantage of ACEinhibitors or ARBs over other antihypertensive drugs inpreventing renal disease. Trials with an activecomparator did not identify any consistent benefit on theoccurrence of end-stage renal disease, doubling ofcreatinine, or other indices of renal function (figure 2).Although a small benefit was recorded on urine albuminexcretion in favour of ACE inhibitors or ARBs compared
with antihypertensive drugs, significant small-study biaswas also seen. This lack of specific benefit of ACEinhibitors or ARBs in diabetic renal disease accords withfindings seen in cardiovascular outcomes.34
In conclusion, claims that ACE inhibitors and ARBsare renoprotective in diabetes seem to derive fromsmall placebo-controlled trials that provide uncertainevidence of the existence of any true advantage over andabove blood-pressure control. For renal outcomes,blood-pressure lowering remains more important thanthe drug class prescribed. More persuasive evidenceexists that shows a specific renoprotective effect in non-diabetic renal disease than in diabetic renal disease, butuncertainty remains. Further trials of the effect of
ACE inhibitors and ARBs on the progression of renaldisease will be most informative if their designincludes antihypertensive comparators, and if they areadequately powered to detect differences in clinicallyimportant renal endpoints. Such studies will have to bevery much larger than has hitherto been customary.There seems to be little justification for ACE inhibitorsor ARBs to be first-line choices for renoprotection indiabetes on the basis of efficacy, and residual uncer-tainty still exists about the inherent value of thesedrugs in other renal disorders. In view of the presentanalysis, treatment decisions for hypertension inrenal disease should be based on the blood-pressure-lowering effect, comparative tolerability, and cost ofantihypertensive treatment.
-
8/14/2019 Acei Dan Arb
8/8
Articles
www.thelancet.com Vol 366 December 10, 2005 2033
Contributors
J P Casas contributed to the protocol design, data extraction, and
statistical analysis. W Chua and S Loukogeorgakis helped with theprotocol design and data extraction. P Vallance helped with the datainterpretation. L Smeeth helped with the protocol design and statisticalanalysis. A D Hingorani contributed to the protocol design and datainterpretation. R J MacAllister contributed to the protocol design, dataextraction, and analysis and interpretation of data. All authorscontributed to the writing and revision of the report.
Conflict of interest statement
P Vallance receives payment as a member of the Research AdvisoryBoard for Glaxo-Smith-Kline. The remaining authors declare that theyhave no conflict of interest.
Acknowledgments
We thank A H Barnett, T Kazumi, G A Cinotti, G Remuzzi, H Herlitz,A L Kamper, S Katayama, G Schernthaner, L Tarnow, J Ahmad,F H Nystrom, R Pontremoli, E B Pedersen, M Praga, T Shiigai,S Ljungman, N Bascil Tutuncu, I M Stratton, A Ersoy, J A Staessen,
L Thijs, K T Woo, P de Leeuw, L Del Vecchio, A Perna, C Mogensen,P Ruggenenti, H Ahmad, M A Siddique, I Parwez, S Shafique, andother authors for providing relevant information from clinical trialsabout renal outcomes, characteristics of patients investigated, and studydesign; and Valerie McCormack for her statistical support. Thesecontributors do not necessarily agree with all parts of the paper.LS holds a UK Medical Research Council Clinician Scientist Fellowship.ADH holds a British Heart Foundation Senior Fellowship.
References1 Renal Association. Treatment of adults and children with renal
failure: standards and audit measures. 3rd edn. London: RoyalCollege of Physicians of London and the Renal Association, 2002.
2 Williams B, Poulter NR, Brown MJ, et al. Guidelines formanagement of hypertension: report of the fourth working party ofthe British Hypertension Society, 2004-BHS IV.J Hum Hypertens2004; 18: 13985.
3 McIntosh A, Hutchinson A, Marshall S, et al. Clinical guidelines and
evidence review for type 2 diabetes. Renal disease: prevention andearly management. Sheffield: ScHARR, University of Sheffield, 2002.
4 Royal College of General Practitioners. http://www.rcgp.org.uk/(accessed March 1, 2005).
5 American Diabetes Association. Standards of medical care indiabetes, 2005. Diabetes Care 2005; 28 (suppl 1): S436.
6 Chobanian AV, Bakris GL, Black HR, et al. The seventh report of thejoint national committee on prevention, detection, evaluation, andtreatment of high blood pressure: the JNC 7 report.JAMA 2003; 289:256072.
7 Heart Outcomes Prevention Evaluation Study Investigators. Effectsof ramipril on cardiovascular and microvascular outcomes in peoplewith diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet2000; 355: 25359.
8 Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect ofangiotensin-converting-enzyme inhibition on diabetic nephropathy.The Collaborative Study Group. N Engl J Med1993; 329: 1456-62.
9 Lewis EJ, Hunsicker LG, Clarke WR, et al; Collaborative StudyGroup. Renoprotective effect of the angiotensin-receptor antagonistirbesartan in patients with nephropathy due to type 2 diabetes.N Engl J Med2001; 345: 85160.
10 EURopean trial On reduction of cardiac events with Perindopril instable coronary Artery disease Investigators. Efficacy of perindopril inreduction of cardiovascular events among patients with stablecoronary artery disease: randomised, double-blind, placebo-controlled,multicentre trial (the EUROPA study). Lancet2003; 362: 78288.
11 The Heart Outcomes Prevention Evaluation (HOPE) StudyInvestigators. Effects of an angiotensin converting enzyme inhibitor,ramipril, on cardiovascular events in high-risk patients. N Engl J Med2000; 342: 14553.
12 PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individualswith previous stroke or transient ischaemic attack. Lancet2001; 358:103341.
13 Weber MA, Julius S, Kjeldsen SE, et al. Blood pressure dependent
and independent effects of antihypertensive treatment on clinicalevents in the VALUE Trial. Lancet2004; 363: 204951.
14 Prospective Studies Collaboration. Age-specific relevance of usualblood pressure to vascular mortality: a meta-analysis of individual
data for one million adults in 61 prospective studies. Lancet2002;360: 190313.
15 Blood Pressure Lowering Treatment Trialists Collaboration.Effects of different blood-pressure-lowering regimens on majorcardiovascular events: results of prospectively-designed overviewsof randomised trials. Lancet2003; 362: 152735.
16 Law M, Wald N, Morris J. Lowering blood pressure to preventmyocardial infarction and stroke: a new preventive strategy.Health Technol Assess 2003; 7: 194.
17 He J, Whelton PK. Elevated systolic blood pressure and risk ofcardiovascular and renal disease: overview of evidence fromobservational epidemiologic studies and randomized controlledtrials. Am Heart J1999; 138: 21119.
18 Klag MJ, Whelton PK, Randall BL, et al. Blood pressure and end-stage renal disease in men. N Engl J Med1996; 334: 1318.
19 Tozawa M, Iseki K, Iseki C, Kinjo K, Ikemiya Y, Takishita S. Bloodpressure predicts risk of developing end-stage renal disease in menand women. Hypertension 2003; 41: 134145.
20 Jafar TH, Schmid CH, Landa M, et al. Angiotensin-convertingenzyme inhibitors and progression of nondiabetic renal disease. Ameta-analysis of patient-level data. Ann Intern Med2001; 135: 7387.
21 Giatras I, Lau J, Levey AS. Effect of angiotensin-converting enzymeinhibitors on the progression of nondiabetic renal disease: a meta-analysis of randomized trials. Angiotensin-Converting-EnzymeInhibition and Progressive Renal Disease Study Group.Ann Intern Med1997; 127: 33745.
22 Strippoli GF, Craig M, Deeks JJ, Schena FP, Craig JC. Effects ofangiotensin converting enzyme inhibitors and angiotensin IIreceptor antagonists on mortality and renal outcomes in diabeticnephropathy: systematic review. BMJ2004; 329: 828.
23 Deeks JJ, Higgins, JPT, Altman DG, eds. Analysing and presentingresults. In: Alderson P, Green S, Higgins J, eds. Cochrane Reviewershandbook 4.2.2 (updated March, 2004); section 8. http://www.cochrane.org/resources/handbook/hbook.htm (accessed Jan 31, 2004).
24 Pudar Hozo S, Djulbegovic B, Hozo I. Estimating the mean and
variance from the median, range, and the size of a sample.BMC Med Res Methodol2005; 5: 13.
25 Altman DG. Practical statistics for medical research. London:Chapman & Hall, 1991.
26 Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen,C-reactive protein, albumin, or leukocyte count with coronary heartdisease: meta-analyses of prospective studies.JAMA 1998; 279:147782.
27 Rahman M, Pressel S, Davis BR, et al. Renal outcomes in high-riskhypertensive patients treated with an angiotensin-converting enzymeinhibitor or a calcium channel blocker vs a diuretic: a report from theAntihypertensive and Lipid-Lowering Treatment to Prevent HeartAttack Trial (ALLHAT). Arch Intern Med2005; 165: 93646.
28 Voyaki SM, Staessen JA, Thijs L, et al. Systolic Hypertension inEurope (Syst-Eur) Trial Investigators. Follow-up of renal functionin treated and untreated older patients with isolated systolichypertension.J Hypertens 2001; 19: 51119.
29 Sterne JA, Gavaghan D, Egger M. Publication and related bias in
meta-analysis: power of statistical tests and prevalence in theliterature.J Clin Epidemiol2000; 53: 111929.
30 Teo KK, Yusuf S, Collins R, Held PH, Peto R. Effects ofintravenous magnesium in suspected acute myocardial infarction:overview of randomised trials. BMJ1991; 303: 1499503.
31 ISIS-4 (Fourth International Study of Infarct Survival)Collaborative Group. ISIS-4: a randomised factorial trial assessingearly oral captopril, oral mononitrate, and intravenous magnesiumsulphate in 58 050 patients with suspected acute myocardialinfarction. Lancet 1995; 345: 66985.
32 Yusuf S, Flather M. Magnesium in acute myocardial infarction.BMJ1995; 310: 75152.
33 Egger M, Smith GD. Misleading meta-analysis. BMJ1995; 310:75254.
34 Turnbull F, Neal B, Algert C, et al.; Blood Pressure LoweringTreatment Trialists Collaboration. Effects of different bloodpressure-lowering regimens on major cardiovascular events inindividuals with and without diabetes mellitus: results ofprospectively designed overviews of randomized trials.Arch Intern Med2005; 165: 141019.