6.1. Antihipertensi

of 52
Transcript of 6.1. Antihipertensi
-
8/13/2019 6.1. Antihipertensi
1/52
ANTIHIPERTENSI
-
8/13/2019 6.1. Antihipertensi
2/52
PENDAHULUAN
Hipertensi adalah peningkatan tekanan darah
(sistole > 140 mmHg, diastole > 90 mmHg).
Klasifikasi berdasarkan JNC VII, 2003.
TD ditentukan oleh : cardiac output dan
peripheral vascular resistance.
Organ yang berpengaruh : jantung, pembuluh
darah, ginjal.
-
8/13/2019 6.1. Antihipertensi
3/52
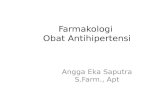
CNS
HEART
BV
SYMPATHETICNERVE
1
1
KIDNEY
1 ReninAg
A-I A-II
ACE
Ca++
Aldosteron
Retention
Na & water
BR
2BP
pathophysiopharmacology of hypertension
-
8/13/2019 6.1. Antihipertensi
4/52
First-line antihypertensive drugs
Diuretics
blockers
1blockers
ACE inhibitors
Angiotensin II antagonists
Ca antagonists
-
8/13/2019 6.1. Antihipertensi
5/52
Combination Therapies
-adrenergic blockers and diuretics
ACE inhibitors and diuretics
Angiotensin II receptor antagonists anddiuretics
Calcium antagonists and ACE inhibitors
Other combinations
-
8/13/2019 6.1. Antihipertensi
6/52
Drugs used in hypertension
The four major groups of antihypertension drugs :
1. Diuretics
2. Sympathoplegics
3. Vasodilator4. Angiotensin antagonis
-
8/13/2019 6.1. Antihipertensi
7/52
-
8/13/2019 6.1. Antihipertensi
8/52
-
8/13/2019 6.1. Antihipertensi
9/52
Sympathoplegics
Sympathoplegics sympathetic nerve function inseveral ways
Effects : reduction of venous tone, Heart rate (HR),contractile force of the heart, Cardiac Output (CO) &
total peripheral resistance Compensatory responses & adverse effects are marked
Classification:
- Baroreceptor-sensitizing agents
- CNS-active agents
- Ganglion-blocking drugs
- Postganglionic Sympathetic nerve terminal blockers
- Adrenoceptor blockers
-
8/13/2019 6.1. Antihipertensi
10/52
-
8/13/2019 6.1. Antihipertensi
11/52
-
8/13/2019 6.1. Antihipertensi
12/52
CNS-Active Agents
Prototype : Alpha2-selective agonists (clonidine,methildopa)
Effects : reducing sympathetic outflow by activation of
2
receptors in the CNS
The drugs readily enters the CNS when given orally
Methildopais prodrug; it is converted tomethilepinephrine in the brain.
Tox: salt retention, rebound hypertension (suddendicontinuation of clonidine), hematologicimmunotoxicity-hemolytic anemia (methyldopa),sedation (both drugs)
-
8/13/2019 6.1. Antihipertensi
13/52
Ganglion-blocking drugs
Prototype : nicotinic blockers (trimetaphan,hexamethonium)
Effects: extremely powerful BP-lowering
Tox:- salt retention.
- blurred vision, constipation, urinary hesitancy,
sexual dysfunction (PS blockade).
- sexual disfunction, orthostatic hypotension
(Simpathetic blockade).
-
8/13/2019 6.1. Antihipertensi
14/52
-
8/13/2019 6.1. Antihipertensi
15/52
Adrenoceptor Blockers
Prototype : -blockers (prazosin-a selective agent,phentolamine, phenoxybenzamine), -blockers(propanolol)
Mechanism of action : Reduce vasc resistance & venous return (alpha-
blocker).
Reduce CO, decrease vasc resistance, reduce
angiotensin levels The non-selective -blockers are of no value in
chronic hypertension because of excessivecompensatory responses, especially tachycardia
-
8/13/2019 6.1. Antihipertensi
16/52
Vasodilator
Drugs that dilate blood vessels by actingdirectly on smooth muscle cells.
Four major mechanism :
- release of nitric oxide.
- opening of potassium channels.
- blockade of calcium channels.
- activation of D1 receptor.
-
8/13/2019 6.1. Antihipertensi
17/52
Vasodilator
Hydralazine & Minoxidil They have more effects on arterioles than on venous.
Orally active & suitable for chronic therapy.
Mechanism of action:
release of nitric oxide from endothelial cells(hydralazine)
potassium channel opener (minoxidil)
Toxicity:
tachycardia, salt&water retention, drug-inducedlupus erythematosus (hydralazine)
severe compensatory response, hirsuitisme,pericardial abnormality (Minoxidil)
-
8/13/2019 6.1. Antihipertensi
18/52
Vasodilator
Ca-channel Blocker
Prototype : nifedipine, verapamil, diltiazem
They are effective venodilator because they areorally active, suitable for chronic hypertensionof any severity.
They produce fewer compensatory response.
-
8/13/2019 6.1. Antihipertensi
19/52
Vasodilator
Nitroprusside & Diazoxide
Mechanism of action : nitroprussid release of nitric oxide.
diazoxide opens potassium channels, thus hyperpolarizing and relaxingsmooth muscle
These drugs given parenterally, used in hypertensive emergencies
Toxicity : excessive hypotension, tachycardia, cyanide toxicity (nitroprusside).
hypotension, hyperglycemia (because this drug reduces insulin release),salt&water retention
Fenolopam
Mechanism of action : D1 receptor activation (arteriolarvasodiation)
Given by IV infusion, used in hypertensive emergencies
-
8/13/2019 6.1. Antihipertensi
20/52
-
8/13/2019 6.1. Antihipertensi
21/52
-
8/13/2019 6.1. Antihipertensi
22/52
-
8/13/2019 6.1. Antihipertensi
23/52
-
8/13/2019 6.1. Antihipertensi
24/52
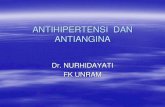
Renal Transport Mechanism
Proximal convoluted tubule (PCT) :
- reabsorption of amino acids, glucose, & numerous cations, NaCl,NaHCO3
- Carbonic anhydrase is the enzyme required for the bicarbonate
reabsorption process on the brush border and in the cytoplasm Thick portion of the ascending limb of the loop of Henle (TAL)
- Pumps NA, K, & Cl out of the lumen into the interstitium of thekidney
- A major site of calcium and magnesium reabsorption
-
8/13/2019 6.1. Antihipertensi
25/52
Renal Transport Mechanism
Distal convoluted tubule (DCT)
- pumps Na & Cl out of the lumen of the nephron via the carier
- reabsorption of Calcium under the control of parathyroid hormone(PTH)
Cortical collecting tubule (CCT)- the last tubular site of sodium reabsorption
- controlled by aldosterone
- the primary site of acidification of the urine and of potassiumexcretion
- Reabsorption of water under the control ADH
-
8/13/2019 6.1. Antihipertensi
26/52
Diuretics
These drugs lower Blood Pressure (BP) by
reduction of Blood volume (BV).
The most important diuretics for hypertension
therapy are The Thiazides and The loop diuretics. The Thiazidesadequate in mild hypertension.
The Loop diureticsadequate in moderate, severe
& malignant hypertension. Compensatory responses to BP-lowering are
minimal.
-
8/13/2019 6.1. Antihipertensi
27/52
-
8/13/2019 6.1. Antihipertensi
28/52
-
8/13/2019 6.1. Antihipertensi
29/52
Carbonic Anhydrase Inhibitors
Prototype : Acetazolamide. This diuretics are sulfonamide derivatives
Mechanism of action : inhibition of carbonic anhydrase in the brush border and intracellulercarbonic anhydrase in the PCT. This inhibition occurs in other tissues of the body as well asin the kidney
Effects :
- bicarbonate diuretics
- body bicarbonate depleted, and metabolic acidosis results.
- resulting in significant potassium wasting
Clinical Uses :
- treatment of glaukoma (major application)
- must be administered orally
- also used to prevent acute mountain (high-altitude) sickness.
- their diuretic effect only use if edema is accompanied by significant metabolic alkalosis. Toxicity : drowsiness, paresthesias, allergy (uncommon), formattion of renal stones
(alkalinization of the urine may cause precipitation of calcium salts), renal potassiumwasting, encephalopathy because of increased ammonia reabsorption.
-
8/13/2019 6.1. Antihipertensi
30/52
-
8/13/2019 6.1. Antihipertensi
31/52
Loop Diuretics
Prototype : Furosemide, bumetanide, torsemide(These are sulfonamidederivatives), ethacrinic acids
Mechanism of action : inhibit the cotransport of Na, K, & Cl. The loop diureticsare relatively short acting
Effects :
- produce a massive NaCl diuresis edema fluid rapidly excreted, Blood volumesignificantly reduced
- the diluting ability of the nephron is reduced
- Ca excretion is significantly increased
- moderately effective uricosuric (Ethacrinic acid)
- significant potassium (K) wasting and excretion H+hypokalemic alkalosis
- Inhibition of prostaglandin synthesis by AINS will decreases of the effficacy ofdiureticsespecially loop diuretic (because of prostaglandin are important inmaintaining glomerular filtration)
-
8/13/2019 6.1. Antihipertensi
32/52
Loop Diuretics
Clinical Use :
- treatment of edematous states (eg, heart failure, ascites)
- acute pulmonary edema
- treatment of severe hypercalcemia (that induced by malignancy)
note : diuresis without volume replacement will result inhemoconcentration
Toxicity :
- induce hypokalemic metabolic alkalosis
- cause hypovolemia and CV complication
- ototoxicity
- may cause sulfonamide allergy
-
8/13/2019 6.1. Antihipertensi
33/52
Thiazide Diuretics Prototype : Hydrochlorotiazide (HCT). All the members of
this group are sulfonamide derivatives
Mechanism of action : inhibit Na, Cl transport in the earlysegment of DCT
Effects :
- produce moderate sodium and chloride diuresis
- hypokalemic metabolic alkalosis may occur
- reduce intracellular sodium & promotes sodium-calciumexchangeurine calcium content decrease
- reduce BP (reduction blood volume, reduce vasc resistance)
-
8/13/2019 6.1. Antihipertensi
34/52
Thiazide Diuretics
Clinical use : hypertension, chonic therapy ofedematous (CHF), chronic renal calcium stoneformation
Toxicity :
- massive diuresis with hyponatremia
- potassium wasting
- hyperglycemia (in diabetic patient)
- increase of serum uric acid and lipid levels- potential sulfonamide allerginicity
-
8/13/2019 6.1. Antihipertensi
35/52
Potassium-Sparing Diuretics
Prototype : spironolactone, a steroid derivative; amiloride, triamterene Mechanism of action : a pharmacologic antagonist of aldosterone in the
collecting tubules
Effects :
- increase in sodium clearance
- decrease in K & H+
excretion (potassium-sparing diuretics)- may cause hyperkalemic metabolic acidosis
Clinical use :
- potassium wasting caused by chronic therspy with loop or thiazidediuretics
- Aldosteronism (that may occur in cirrhosis, heart failure)
Toxicity : hyperkalemia, gynecomastia, and anti-androgenic effects
-
8/13/2019 6.1. Antihipertensi
36/52
Osmotic Diuretics
Prototype : Mannitol(given by IV),
glycerin, isosorbide, and urea(rarely used)
Mechanism of action : they poorly reabsorbed from the tubule, remains inthe lumen and holds water by virtue of its osmotic effect.
Effects :
- the volume of urine is increased- reduce brain volume and intracranial pressure by osmotically extractingwater from the tissue into the blood. A similar effects occurs in the eye
Clinical use :
- to maintain high urine flow
- reducing IOP in acute glaucoma- reducing ICP in neurologic conditions
Toxicity : hyponatremia, pulmonary edema (caused by removal of waterfrom intracellular compartment), headche, nausea, & vomiting
-
8/13/2019 6.1. Antihipertensi
37/52
Antiduretic Hormone Agonists
Prototype : ADH (vasopressin), desmopressin. They aremust given parenterally
Mechanism of action : facilitates water reabsorptionfrom the collecting tubule by activating of adenyl
cyclase Effects : reduce in urine volume and increased its
concentration.
Clinical use : pituitary diabetes insipidus
Toxicity : hyponatremia (a large water load),hypertension in large doses
-
8/13/2019 6.1. Antihipertensi
38/52
Antidiuretic Hormone
Antagonists Prototype : Demeclocycline, lithium(given
orally adm)
Mechanism of action : inhibit the action of
ADH Clinical Use : Syndrome of inappropriate of
ADH secretion (SIADH)
Toxicity : bone and teeth abnormalities inchildren (demeclocycline)
-
8/13/2019 6.1. Antihipertensi
39/52
-
8/13/2019 6.1. Antihipertensi
40/52
1% dari penderita hipertensi akan mengalami krisishipertensi dengan gangguan kerusakan organ seperti :
Infark serebral (24.5%)
Ensefalopati (16.3%)
Perdarahan intraserebral/sub-araknoid (4.5%)
Gagal jantung akut dgn edema paru (36.8%) Miokard infark akut/angina tidak stabil (12%)
Diseksi aorta (2%)
Eklampsia(4.5%) Ginjal (1%)
-
8/13/2019 6.1. Antihipertensi
41/52
DEFINISI
Krisis hipertensiadalah suatu keadaan
peningkatan tekanan darah yang mendadak
(sistole >180 mmHg dan/atau diastole >120
mmHg), yang diperoleh dengan sekurangkurangnya dua kali pengukuran, dengan jarak
1-2 menit, pada penderita hipertensi, yang
membutuhkan penanggulangan segera
-
8/13/2019 6.1. Antihipertensi
42/52
KLASIFIKASI HIPERTENSI KRISIS1. H ipertensi emergensi
Kenaikan tekanan darah mendadak yang disertai kerusakanorgan target yang progresif disebut hipertensi emergensi. Padakeadaan ini diperlukan tindakan penurunan tekanan darah yangsegera dalam kurun waktu menit/jam.
2. H ipertensi urgensiKenaikan tekanan darah mendadak yang tidak disertaikerusakan organ target disebut hipertensi urgensi.
Penurunan tekanan darah pada keadaan ini harus dilaksanakandalam kurun waktu 24-48 jam.
Kedua jenis krisis hipertensi ini perlu dibedakan dengan caraanamnesis dan pemeriksaan fisik, karena baik faktor risiko dan
penanggulangannya berbeda.
-
8/13/2019 6.1. Antihipertensi
43/52
-
8/13/2019 6.1. Antihipertensi
44/52
VI. TATALAKSANA KRISIS
HIPERTENSI
Penatalaksanaan krisis hipertensi sebaiknya
dilakukan di rumah sakit, namun dapat
dilaksanakan di tempat pelayanan primersebagai pelayanan pendahuluan dengan
pemberian obat anti hipertensi oral.
Sebelum
RS
Di
RSTransportasi
Sebelum Rumah Sakit
-
8/13/2019 6.1. Antihipertensi
45/52
Obat-obatan yang beredar di Indonesia
Sebelum Rumah Sakit
-
8/13/2019 6.1. Antihipertensi
46/52
Obat-obatan yang digunakan pada
hipertensi emergensi
A.Clonidin (Catapres) IV
B.Diltiazem (Herbesser) IVC.Nicardipin (Perdipin) IV
D.Labetalol (Normodyne) IV
E.Nitroprusside (Nitropress, Nipride) IV
Cl idi (C t ) IV
-
8/13/2019 6.1. Antihipertensi
47/52
Clonidin (Catapres) IV
(150 mcg/ampul)
Clonidin 900 mcg dimasukkan dalam cairan infus glucosa 5%500cc dan diberikan dengan mikrodrip 12 tetes / menit, setiap15 menit dapat dinaikkan 4 tetes sampai tekanan darah yangdiharapkan tercapai.
Bila target tekanan darahtercapai pasien diobservasi selama 4jam kemudian diganti dengan tablet Clonidin oral sesuaikebutuhan.
Clonidin tidak boleh dihentikan mendadak, tetapi dosisditurunkanperlahan-lahan oleh karena bahaya rebound
phenomen, dimana tekanan darah naik secara cepat bila obatdihentikan.
-
8/13/2019 6.1. Antihipertensi
48/52
-
8/13/2019 6.1. Antihipertensi
49/52
Nicardipin (Perdipin) IV
(2 mg dan 10 mg/ampul)
Nicardipin diberikan 10-30 mcg/kgBB bolus.
Bila tekanan darah tetap stabil?diteruskan
dengan 0.5- 6 mcg/kgBB/menit sampai target
tekanan darah tercapai.
-
8/13/2019 6.1. Antihipertensi
50/52
Labetalol (Normodyne) IV*
Labetalol diberikan 20-80 mg IV bolus setiap 10
menit atau dapat diberikan dalam cairan infus dengandosis 2 mg/menit.
Nitroprusside (Nitropress, Nipride) IV*
Nitroprusside diberikan dalam cairan infus dengandosis 0.25-10.00 mcg/kg/menit
Hatihati, fotosensitif. Obat harus dilindungi daricahaya, misalnya dengan kain/ plastik hitam.
* Obat-obat ini belum beredar resmi di Indonesia
-
8/13/2019 6.1. Antihipertensi
51/52
KRISIS HIPERTENSI PADA
KEADAAN KHUSUS:
A. Krisis Hipertensi pada Gangguan Otak
B. Krisis Hipertensi pada Penyakit Jantung
C. Krisis Hipertensi pada Penyakit Ginjal
D. Krisis Hipertensi pada Gangguan Endokrin
E. Krisis Hipertensi pada Kehamilan
F. Krisis Hipertensi pada Pengguna Napza
-
8/13/2019 6.1. Antihipertensi
52/52
Obat-obat parenteral untuk penanganan hipertensiemergensi pada edema paru dan sindroma koroner akut